

Abstract
Purpose: To investigate the feasibility rate and the mid-term outcomes of fusion imaging-guided radiofrequency ablation (RFA) with artificial ascites or pleural effusion of hepatocellular carcinomas (HCCs) based on tumor locations.
Materials and Methods: In this single-center retrospective study, 456 patients with single HCCs ≤4 cm were referred for RFA from April 2019 to April 2020. The tumor locations were classified into a conventional location (CL) and difficult location (DL, close to the diaphragm/heart/major vessels/bile ducts/gastrointestinal tract/kidneys). This study assessed the feasibility rate of CT/MRI-US fusion system-guided RFA with artificial ascites or pleural effusion and the therapeutic outcomes including technical success, technique efficacy, and local tumor progression (LTP) according to tumor location. Cumulative LTP rates were estimated using the Kaplan–Meier method.
Results: 235 of 456 (51.5%) patients had HCCs in DL. Ablation was feasible in 431 of 456 (94.5%) patients. The feasibility rate was significantly lower in DL group than in CL group (89.8% [211/235] vs. 99.5% [220/221], p < 0.001). The technical success and technique efficacy rates were 100% [211/211] vs. 99.5% [219/220] and 98.6% [208/211] vs. 100% [220/220] in DL and CL groups, respectively (p > 0.05). The estimated 1-, 2-, and 3-year cumulative LTP rates in DL group were 1.0%, 2.5%, and 2.5%, respectively, and were not significantly different from the 2.3%, 3.9%, and 3.9% observed in CL group (p = 0.456).
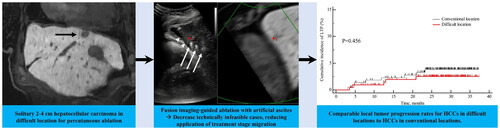
Conclusion: Fusion imaging-guided RFA with artificial ascites or pleural effusion could decrease technically infeasible cases and provide comparable LTP rates for HCCs in DL to HCCs in CL.
Graphical Abstract
Author contributions
Conceptualization: J.M.L.
Data curation: J.H.K.
Formal analysis: J.H.K.
Funding acquisition: J.M.L.
Investigation: J.M.L., J.Y.L., D.H.L.
Methodology: J.M.L., D.H.L., J.H.Y., I.J., J.H.K.
Project administration: J.M.L.
Resources: J.M.L.
Software: N/A
Supervision: J.M.L., J.Y.L., D.H.L., J.H.Y., I.J., J.Y., Y.J.K., S.J.Y.
Validation: N/A
Visualization: J.H.K.
Writing-original draft: J.M.L., J.H.K.
Writing-review & editing: J.M.L., J.H.Y., I.J., D.H.L., J.H.K., J.Y., Y.J.K., S.J.Y.
Disclosure statement
There are no relevant conflicts of interest related to the submitted work. J.M.L has received grants from Bayer Healthcare, Canon Healthcare, Philips Heathcare, GE Healthcare, CMS, Guerbet, Samsung Medison, and Bracco. J.M.L has received personal fees from Bayer Healthcare, Siemens Healthineer, Samsung Medison, Guerbet, and Philips Healthcare. J.H.Y has received honorarium from Bayer Healthcare and personal fee from Philips Healthcare. For the remaining authors none were declared.
Data availability statement
Raw data were generated at Seoul National University Hospital. Derived data supporting the findings of this study are available from the corresponding author J.M.L. on request.