
Abstract
Objective
To investigate the changes in liver and kidney function, red blood cell (RBC) count and hemoglobin (HGB) levels in patients undergoing ultrasound-guided percutaneous microwave ablation (UPMWA) for uterine fibroids on postoperative day 1.
Methods
The changes in liver and kidney function, RBC count and HGB levels in 181 patients who underwent selective UPMWA in the Second Affiliated Hospital of Shantou University Medical College, China, between August 2017 and January 2023 were retrospectively analyzed.
Results
All patients underwent UPMWA for uterine fibroids; 179 patients had multiple uterine fibroids and 2 patients had single uterine fibroids. The maximum fibroid diameter ranged from 18 to 140 mm, with an average of 68.3 mm. Ultrasound imaging was used to confirm that the blood flow signal within the mass had disappeared in all patients, indicating that the ablation was effective. Within 24 h, compared with before UPMWA, levels of total bilirubin, direct bilirubin, indirect bilirubin and aspartate aminotransferase had significantly increased (p < 0.01), whereas levels of total protein, albumin, globulin, alanine aminotransferase, creatinine and urea had significantly decreased (p < 0.01). Acute kidney injury (AKI) occurred in 1 of the 181 patients. The RBC count and HGB levels decreased significantly after UPMWA (p < 0.01).
Conclusion
Ultrasound-guided percutaneous microwave ablation for uterine fibroids can impose a higher detoxification load on the liver and cause thermal damage to and the destruction of RBCs within local circulation, potentially leading to AKI. Protein levels significantly decreased after UPMWA. Therefore, perioperative organ function protection measures and treatment should be actively integrated into clinical practice to improve prognosis and enhance recovery.
Background
Ultrasound-guided percutaneous microwave ablation (UPMWA) is a minimally invasive treatment method. However, it can induce thermal denaturation and coagulative necrosis of the target tissues because ablation electrodes are inserted into the target lesions under ultrasound guidance at a temperature of 60 °C–100 °C and are eventually absorbed by the organism. This method has been widely used for the treatment of benign and malignant tumors of the liver, kidney, uterus and other organs [Citation1–5]. However, UPMWA has also been observed to result in acute kidney injury (AKI) [Citation6–8]. According to previous studies, the incidence of AKI is 1.5% after liver thermal ablation [Citation9], but it increases to 23.6% when the tumor volume is >5 cm [Citation10]. Given that uterine fibroids are often multiple and massive, treating them with UPMWA can involve prolonged thermal ablation, leading to the formation of a substantial amount of coagulative necrotic tissue. However, reports on the impact of UPMWA on liver and kidney function or on red blood cell (RBC) count and hemoglobin (HGB) levels are limited. The aim of this study is to provide valuable insights into perioperative organ function protection and the prediction of risks associated with UPMWA.
Materials and methods
Patients
The clinical data of 247 patients who underwent UPMWA in the Second Affiliated Hospital of Shantou University Medical College, China, between August 2017 and January 2023 were retrospectively analyzed. In this study, changes in liver and kidney function, RBC count and HGB levels after UPMWA were investigated. The inclusion criteria for patients were as follows: 1. patients scheduled for UPMWA therapy for uterine fibroids; 2. patients older than 18 years; 3. absence of any malignancy or haematological diseases; 4. completion of blood, liver function and kidney function tests before the operation and on day 1 after ablation; 5. normal liver and kidney function test results; 6. no prior treatment for uterine fibroids. Exclusion criteria: 1. history of rapid enlargement of uterine fibroids within a short timeframe (with the possibility of malignant degeneration of uterine fibroids); 2. serious insufficiency of the heart, liver, kidney and other vital organs; 3. pelvic infection or adhesion; 4. children and women who are menstruating, breastfeeding, pregnant or postmenopausal; 5. cognitive impairment; 6. abnormal blood coagulation; 7. history of myoma interventional and surgical operations. Prior to treatment, all patients provided informed consent through a preoperative consent form. This study was approved by the Clinical Ethics Committee of the Second Affiliated Hospital of Shantou University Medical College (ethical approval number: 2022-38).
Preparation and tests
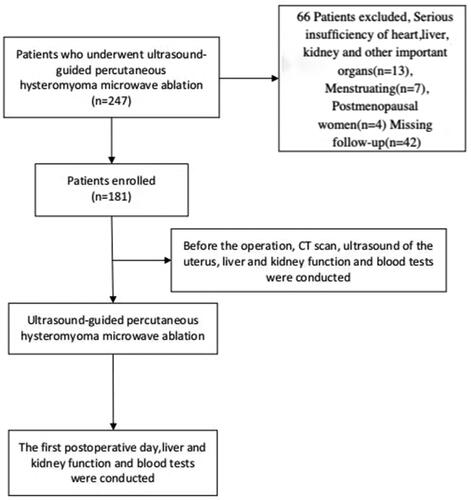
Before the operation, a comprehensive set of examinations was conducted, including computed tomography scan and ultrasound of the uterus, as well as liver and kidney function and blood tests. Patients with preexisting conditions, such as hypertension, diabetes and coronary diseases or other comorbidities, underwent consultation and specialized treatment with relevant specialists. On day 1 following ablation, postoperative follow-up blood tests were performed, and any significant abnormalities were promptly identified and treated ().
Figure 1. Study design flow chart.
Anesthesia procedures
As per the guidelines, patients were instructed to adhere to an 8-h solid food fasting and 2-h liquid fasting regimen prior to surgery. Intraoperative and postoperative fluid rehydration therapy was continued. No preoperative medications were administered. Ultrasound-guided percutaneous hysteromyoma microwave ablation procedures were performed under general endotracheal anesthesia. To reduce the effects of the anesthetic drugs on liver and kidney function, intravenous induction involved the administration of midazolam (0.05–0.1 mg/kg), propofol (2–3 mg/kg), fentanyl (2–3 μg/kg) or sufentanil (0.3–0.5 μg/kg), along with cis-atracurium (0.15 mg/kg) for neuromuscular blockade. Following tracheal intubation, patients were mechanically ventilated. Anesthesia was maintained through a continuous infusion of propofol (6–12 mg/kg/h), remifentanil (0.05–1 μg/kg/min) and cis-atracurium (0.05 mg/kg/h). All patients were treated with drugs after hepatorenal dysfunction was identified. Patients with renal insufficiency underwent a furosemide diuresis and sodium bicarbonate injection of alkalized urine. Patients with abnormal liver function were treated with sodium glucuronic acid injection or magnesium isoglycyrrhizinate injection.
Surgical procedures
Under the guidance of an RS80A ultrasound diagnostic instrument (Samsung Medison), artificial ascites was generated by a continuous drip of sterilized distilled water through a puncture needle. This technique aimed to create a barrier to thermally isolate the intestines. Similarly, a puncture needle was inserted into the uterine cavity to protect the endometrium. The percutaneous placement of electrodes (Model: ECO-100AI8, Nanjing Yigao Microwave System Engineering Company, Nanjing, China) at the uterine fibroids was performed, followed by multipoint ablations using a microwave therapy instrument (Model: ECO-100AI, Nanjing Yigao Microwave System Engineering Company) with a power range of 40–60 W. Each ablation point lasted between 3 and 10 min until complete coverage of the fibroids was achieved. Ultrasound imaging was employed to confirm the absence of blood flow signals within the mass and assess the effectiveness of the ablation. Subsequently, the artificial ascites were withdrawn using suction.
Assessment indicators
1. Change in liver function
Prior to and on the morning of postoperative day 1 following UPMWA, a routine fasting blood sample was collected to evaluate the levels of various liver function parameters, including total protein (TP), albumin (ALB), globulin (GLB), total bilirubin (T-Bil), direct bilirubin (D-Bil), indirect bilirubin (I-Bil), aspartate aminotransferase (AST) and alanine aminotransferase (ALT).
2. Change in kidney function
Similarly, a fasting blood sample was collected to assess the levels of urea (UREA) and creatinine (Cr) before the procedure and on the morning of postoperative day 1 following UPMWA. The diagnosis of AKI was based on the criteria outlined in the 2012 KDIGO Clinical Practice Guideline for Acute Kidney Injury [Citation11]. Acute kidney injury was diagnosed if any of the following conditions were met: 1) an increase in Cr levels >26.5 μmol/L within 48 h; 2) Cr levels exceeding 1.5 times the baseline value within 7 days; 3) urine output below 0.5 ml/(kg•h) for 6 h.
3. Change in red blood cell count and hemoglobin levels
The RBC count and HGB levels were assessed by collecting a fasting blood sample before the procedure and on the morning of postoperative day 1 following UPMWA.
Statistical analysis
The data were analyzed using SPSS software, version 22. Paired t-tests were employed to compare variables. Statistical significance was determined using a p-value <0.05.
Results
1. General clinical data of the patients
This study included 181 patients, 179 with multiple uterine fibroids and 2 with single uterine fibroids. The age range was 22–52 years, with an average of 42 years. Their weight ranged from 40 to 87.5 kg, with an average of 57.6 kg. The maximum fibroid diameter ranged from 18 to 140 mm, with an average of 68.3 mm. All patients underwent UPMWA for uterine fibroids, and ultrasound imaging confirmed that the blood flow signal in the mass had disappeared, indicating that ablation was effective.
2. Comparison of liver function before and after ultrasound-guided percutaneous microwave ablation
Following UPMWA, a significant decrease in the levels of TP, ALB, GLB and ALT (p < 0.01) and a significant increase in the levels of T-Bil, D-Bil, I-Bil and AST (p < 0.01) was observed (). The liver function indexes of most patients (n = 174) were within the normal range, and patients with abnormal indexes (n = 7) were treated with sodium glucuronic acid injection or magnesium isoglycyrrhizinate injection for liver protection; these indexes generally returned to normal on postoperative day 5.
Table 1. Comparison Of liver function before and after UPMWA.
3. Comparison of kidney function before and after ultrasound-guided percutaneous microwave ablation
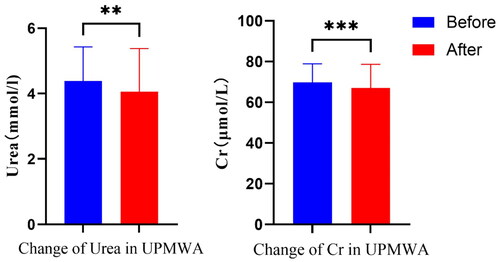
Among the 181 patients enrolled in the study, only 1 developed AKI. This was characterized by an increase in Cr levels from 65.3 to 171 μmol/L and UREA levels from 4.63 to 9.35 mmol/L early in the morning of the day after UPMWA, with Cr levels of 280 μmol/L and UREA levels of 10.9 mmol/L 2 days after ablation. After diuresis using furosemide and the alkalinisation of urine with sodium bicarbonate injection, the Cr and UREA levels were successfully reduced, eventually returning to normal by postoperative day 16. Overall, a significant decrease in Cr and UREA levels after UPMWA (p < 0.01) was identified ().
Table 2. Comparison of kidney function before and after UPMWA.
4. Comparison of red blood cell count and hemoglobin levels before and after ultrasound-guided percutaneous microwave ablation
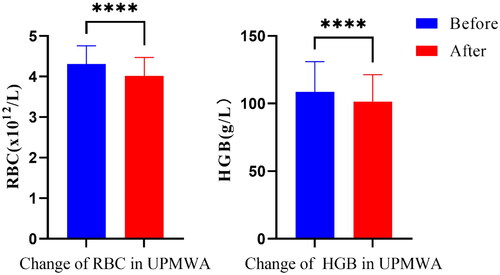
Data analysis revealed a statistically significant decrease in the RBC count and HGB levels after UPMWA (p < 0.01) ().
Table 3. Comparison of RBC and HGB levels before and after UPMWA.
Discussion
Uterine fibroids are the most prevalent benign tumors in women. In current clinical practice, the conventional surgical approach is being increasingly supplanted by minimally invasive and highly efficient thermal ablation procedures, which can also preserve patients’ reproductive and endocritic function [Citation12]. Ultrasound-guided percutaneous microwave ablation is not limited by the size or location of the lesion. It can establish a high-temperature thermal field in the target area through rapid heating and a short treatment duration, making it particularly suitable for managing large-volume tumors [Citation13–17]. However, case reports have highlighted potential organ function impairment during UPMWA, leading to prolonged hospital stays and suboptimal postoperative recovery [Citation9,Citation10,Citation12,Citation18].
In this study, a retrospective analysis of clinical data from 181 patients who underwent UPMWA for uterine fibroids was performed. Following UPMWA treatment, a significant increase in T-Bil, D-Bil, I-Bil and AST levels () was identified, and a significant decrease in the levels of ALT, primarily present in hepatocytes, was observed. Additionally, the RBC count and HGB levels decreased (), clearly indicating thermal damage to RBCs within local circulation during thermal ablation [Citation10]. These findings suggest that although thermal ablation does not directly damage liver cells, the absorption of necrotic tissue, along with the thermal destruction and increased hemolysis of RBCs within local circulation, contributes to an increased detoxification load on the liver.
Figure 2. The comparison of the values of liver function before and after UPMWA. (*p < 0.05, as determined by a t-test comparing the values before and after UPMWA).
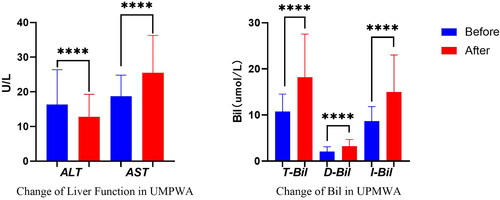
Figure 3. The comparison of the values of RBC and HGB before and after UPMWA. (*p < 0.05, as determined by a t-test comparing the values before and after UPMWA).
In this study, after UPMWA, TP, ALB and GLB levels decreased, which is a novel finding in cases of thermal ablation treatment. Since the blood samples were obtained on the day following UPMWA, the decrease in TP levels within such a short timeframe cannot be attributed to liver protein synthesis inhibition or increased body catabolism after acute injury. This decrease may be attributed to the thermal damage of protein within local circulation or the increased permeability of local vascular and cellular membranes following thermal injury, leading to the osmotic transfer of intravascular fluid and protein. Further studies are needed to elucidate the exact mechanisms underlying these protein changes and to explore potential strategies for minimizing their impact during UPMWA procedures.
After thermal ablation, the reabsorbed necrotic tissue, toxins and free HGB in circulation can undergo hepatic metabolism before being filtered through the glomerulus. Especially in an acidic environment, these substances are prone to deposition at renal tubules, leading to blockages and potential kidney injury. Studies have demonstrated that free HGB can trigger oxidative stress and disrupt the barrier function of renal tubular epithelial cells [Citation19,Citation20]. Moreover, an increased concentration of free HGB is considered an independent risk factor for AKI [Citation21,Citation22]. In this study, among the 181 patients who underwent UPMWA, 1 patient experienced AKI. This is consistent with other reports on the postoperative incidence of AKI after uterine fibroid thermal ablation [Citation6,Citation7] and is a notably lower AKI incidence rate than that reported after microwave ablation for hepatic tumors [Citation9,Citation10,Citation22]. This association has been attributed to the rich blood supply in the liver and thermal hemolysis. However, in the statistical analysis of all cases in this study, a significant decrease was observed in both Cr and UREA levels after UPMWA (). Further analysis revealed that the patient who developed AKI postoperatively was one of the early cases in our hospital undergoing UPMWA for uterine fibroids and did not receive any specific perioperative protective measures. Consequently, preventive strategies were applied to subsequent cases, which can be summarized as follows: 1. administration of diuretics, such as furosemide and low-dose sodium bicarbonate, to alkalize urine during the ablation procedure, aiming to prevent deposition and blockage in the renal tubules; 2. implementation of rapid intraoperative fluid replacement to dilute circulating blood, thereby reducing cell injury resulting from thermal ablation and improving renal perfusion; 3. continuous infusion of cooled saline into the abdominal and uterine cavities to mitigate thermal damage to RBCs, tissues and organs (temperature monitoring and hypothermia prevention should be carefully observed during the procedure); 4. use of anesthesia drugs with little effect on liver and kidney function during surgery. Fentanyl is hydrolyzed by nonspecific esterase and therefore has no obvious effect on the liver function of patients, and propofol can protect liver cells by removing oxygen free radicals. In addition, the decomposition of atracurium is mainly eliminated by the Hofmann effect, and its action time is not affected by liver and kidney function. The decrease in Cr and UREA levels observed in this study may be attributed to the implementation of these preventive strategies during UPMWA.
Figure 4. The comparison of the values of kidney function before and after UPMWA. (*p < 0.05, as determined by a t-test comparing the values before and after UPMWA).
This study has several limitations. First, it is a single-centre and retrospective study with a relatively small sample size, which may introduce potential biases and limit the generalizability of the findings. Moreover, the postoperative data were collected only on day 1 following UPMWA and therefore lack the continuous and dynamic monitoring of outcome measures. To strengthen the conclusions drawn from this study, future research should focus on multi-centre, large-scale, prospective studies with long-term follow-up to provide additional evidence.
In summary, UPMWA for uterine fibroids should be conducted prudently to avoid its metabolic burden on the liver, thermal damage to the RBC count and protein levels within local circulation, and the potential development of AKI. The implementation of preventive strategies such as local cooling, urine alkalization and the appropriate use of diuretics is essential to safeguard organ function and tissue integrity. Furthermore, close attention should be given to the decrease in protein levels following UPMWA to enhance recovery.
Ethical approval and consent to participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the Research Ethics Committee of The Second Affiliated Hospital of Shantou University Medical College (ethical approval number: 2022-38). Due to the nature of retrospective study and anonymized patien’s information, informed consent is waived with the approval of Ethics Committee of The Second Affiliated Hospital of Shantou University Medical College. All methods were carried out in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable.
Authors’ contributions
Study design: Huang XY, Lu QS, Wu SP, Huang HM, Zhang YF
Data acquisition: Huang XY, Lu QS, Wu SP, Huang HM, Zhang YF
Data analysis and interpretation: Huang XY, Zhang YF
Manuscript preparation: Huang XY, Lu QS, Wu SP, Huang HM, Zhang YF
Critical revision of the manuscript for intellectual content: Zhang YF
Manuscript review: Huang XY, Lu QS, Wu SP, Huang HM, Zhang YF
Obtaining financing: Huang XY
Acknowledgements
N/A.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The data are not publicly available due to their containing information that could compromise the privacy of research participants.
Additional information
Funding
Reference
- Kim-Fuchs C, Candinas D, Lachenmayer A. The role of conventional and stereotactic microwave ablation for intrahepatic cholangiocarcinoma. J Clin Med. 2021;10(13):1. doi: 10.3390/jcm10132963.
- Hui TC, Kwan J, Pua U. Advanced techniques in the percutaneous ablation of liver tumours. Diagnostics (Basel). 2021;11(4):585. doi: 10.3390/diagnostics11040585.
- Ren C, Liang P, Yu XL, et al. Percutaneous microwave ablation of adrenal tumours under ultrasound guidance in 33 patients with 35 tumours: a single-centre experience. Int J Hyperthermia. 2016;32(5):517–7. doi: 10.3109/02656736.2016.1164905.
- Lee JS, Hong GY, Lee KH, et al. Safety and efficacy of ultrasound-guided High-Intensity focused ultrasound treatment for uterine fibroids and Adenomyosis. Ultrasound Med Biol. 2019;45(12):3214–3221. doi: 10.1016/j.ultrasmedbio.2019.08.022.
- Yang Y, Hao Y, Zhang J, et al. Ultrasound-guided percutaneous microwave ablation for subserosal uterine myomas. J Minim Invasive Gynecol. 2019;26(3):544–550. doi: 10.1016/j.jmig.2018.06.014.
- Jeng CJ, Ou KY, Long CY, et al. 500 cases of high-intensity focused ultrasound (HIFU) ablated uterine fibroids and adenomyosis. Taiwan J Obstet Gynecol. 2020;59(6):865–871. doi: 10.1016/j.tjog.2020.09.013.
- Chen J, Chen W, Zhang L, et al. Safety of ultrasound-guided ultrasound ablation for uterine fibroids and adenomyosis: a review of 9988 cases. Ultrason Sonochem. 2015;27:671–676. doi: 10.1016/j.ultsonch.2015.05.031.
- Liu F, Yu X, Liang P, et al. Ultrasonography-guided percutaneous microwave ablation for large hepatic cavernous haemangiomas. Int J Hyperthermia. 2018;34(7):1061–1066. doi: 10.1080/02656736.2017.1392045.
- Yang Y, Liu F, Yu J, et al. Risk factor analysis of acute kidney injury after microwave ablation of hepatocellular carcinoma: a retrospective study. Front Oncol. 2020;10:1408. doi: 10.3389/fonc.2020.01408.
- Ding M, Ma S, Tang X, et al. Oliguric acute kidney injury after microwave ablation of large liver tumors: incidence and preventive measures. Int J Hyperthermia. 2019;35(1):141–149. doi: 10.1080/02656736.2018.1487589.
- Khwaja A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin Pract. 2012;120(4):c179–c184. doi: 10.1159/000339789.
- Tsai MC, Chang LT, Tam KW. Comparison of high-intensity focused ultrasound and conventional surgery for patients with uterine myomas: a systematic review and meta-analysis. J Minim Invasive Gynecol. 2021;28(10):1712–1724. doi: 10.1016/j.jmig.2021.06.002.
- Hinshaw JL, Lubner MG, Ziemlewicz TJ, et al. Percutaneous tumor ablation tools: microwave, radiofrequency, or cryoablation–what should you use and why? Radiographics. 2014;34(5):1344–1362. doi: 10.1148/rg.345140054.
- Zhou W, Arellano RS. Thermal ablation of T1c renal cell carcinoma: a comparative assessment of technical performance, procedural outcome, and safety of microwave ablation, radiofrequency ablation, and cryoablation. J Vasc Interv Radiol. 2018;29(7):943–951. doi: 10.1016/j.jvir.2017.12.020.
- Liu L, Wang T, Lei B. Ultrasound-guided microwave ablation in the management of symptomatic uterine myomas: a systematic review and meta-analysis. J Minim Invasive Gynecol. 2021;28(12):1982–1992. doi: 10.1016/j.jmig.2021.06.020.
- Lin XL, Hai N, Zhang J, et al. Comparison between microwave ablation and radiofrequency ablation for treating symptomatic uterine adenomyosis. Int J Hyperthermia. 2020;37(1):151–156. doi: 10.1080/02656736.2019.1708481.
- Ierardi AM, Petrillo M, Fumarola EM, et al. Percutaneous microwave ablation of uterine fibroids: correlation between shrinkage and trend symptoms. Minim Invasive Ther Allied Technol. 2021;30(1):33–39. doi: 10.1080/13645706.2019.1668417.
- Zhang L, Zhang W, Orsi F, et al. Ultrasound-guided high intensity focused ultrasound for the treatment of gynaecological diseases: a review of safety and efficacy. Int J Hyperthermia. 2015;31(3):280–284. doi: 10.3109/02656736.2014.996790.
- Van Avondt K, Nur E, Zeerleder S. Mechanisms of haemolysis-induced kidney injury. Nat Rev Nephrol. 2019;15(11):671–692. doi: 10.1038/s41581-019-0181-0.
- Deuel JW, Schaer CA, Boretti FS, et al. Hemoglobinuria-related acute kidney injury is driven by intrarenal oxidative reactions triggering a heme toxicity response. Cell Death Dis. 2016;7(1):e2064–e2064. doi: 10.1038/cddis.2015.392.
- Graw JA, Hildebrandt P, Krannich A, et al. The role of cell-free hemoglobin and haptoglobin in acute kidney injury in critically ill adults with ARDS and therapy with VV ECMO. Crit Care. 2022;26(1):50. doi: 10.1186/s13054-022-03894-5.
- Tang X, Ding M, Lu B, et al. Outcomes of ultrasound-guided percutaneous microwave ablation versus surgical resection for symptomatic large hepatic hemangiomas. Int J Hyperthermia. 2019;36(1):632–639. doi: 10.1080/02656736.2019.1624837.