
ABSTRACT
Background
Self-initiated self-repair of problems in speech production has been suggested to be associated with aphasia treatment gains and recovery, but the topic has been little studied. Similarly, the ability to learn novel words has been associated with anomia treatment benefits, although longitudinal data on such learning is lacking.
Aims
The present study’s aim was to examine whether and how self-initiated self-repairs in connected speech and the ability to learn novel vocabulary reflected recovery from aphasia as measured with cognitive-linguistic tests. Additionally, our aim was to explore whether self-initiated repair and novel word learning changed in parallel during recovery.
Methods & Procedures
Four people with aphasia (PWA) (2 anomic, 1 Wernicke, and 1 global aphasia) were tested in the subacute (11 to 68 days post stroke) and chronic (12 months post stroke) phases of recovery with cognitive-linguistic tests, connected speech tasks, and a computerized learning task. In the learning task, PWA associated 6 pseudowords with 6 unfamiliar referents. The associations were learned from an ambiguous setup with feedback. At both time points, learning was measured as correct immediate recognition of the items and recognition maintenance one week post-training. The proportion of self-initiated self-repairs and the proportion of unrepaired problems in connected speech were used as measures of self-repair behavior.
Outcomes & Results
All participants initiated self-repairs both in the subacute and chronic phases, and their self-repairs were most often related to aphasic difficulties in speech production. Between the subacute and chronic phases, self-repairs changed both in quality and quantity. The proportion of self-repair elements decreased in 4/4 participants and the proportion of unrepaired problem segments decreased in 3/4 participants. Of the participants, 3/4 showed significant novel word learning and/or maintenance already in the subacute phase and 4 /4 in the chronic phase.
Conclusion
Reduction in self-initiated self-repairs of speech reflected recovery from aphasia. Novel word learning improved during aphasia recovery from the subacute to the chronic phase. Novel word learning was possible even in subacute, severe aphasia and even in an ambiguous task set-up with no explicitly provided word-referent connections. Novel word learning and self-initiated self-repairs did not change in a clearly parallel manner; however, these findings need to be tested with a larger sample.
1. Introduction
Recovery from aphasia is modulated by a number of factors and is, to date, difficult to predict (Harvey et al., Citation2022; REhabilitation and recovery of peopLE with Aphasia after StrokE (RELEASE) Collaborators, Citation2021). Nevertheless, it is known that one of the key requirements for benefiting from direct aphasia interventions is the ability to learn (Basso, Citation2003). For instance, a good ability to learn novel vocabulary, such as pseudowords or words not familiar from before, has been found to be associated with gains in anomia treatment (Dignam et al., Citation2016). Besides learning ability, PWAs’ capacity to detect errors and self-repair their own speech has been suggested to be associated with recovery from aphasia (R. C. Marshall et al., Citation1994; Middleton et al., Citation2022; Tetnowski et al., Citation2021). As detection of errors, self-repair of speech, and novel word learning have been related to recovery, they merit further study.
In aphasia, self-repair often emerges in connection to word finding difficulty or word selection errors (Laakso, Citation1997), which are the most common and persistent symptoms of aphasia (Laine & Martin, Citation2006). Self-repair can also be found with phonological and morpho-syntactic errors, or even without any linguistic errors, if speakers want to change the content of their speech (Levelt, Citation1983). The current study uses the concept of self-initiated self-repair, which refers to overt efforts to deal with errors and other problems within the ongoing speech of a speaker. In self-initiated self-repair, the speaker first detects a problem in their utterance, for instance, by cutting off a word, pausing, or producing a vocalization/lexical particle (self-initiation), and, if successful, solves the problem by completing the repair segment (self-repair) to improve the comprehensibility of their speech to the interlocutor (Schegloff et al., Citation1977; Schegloff, Citation2007, p. 101). We chose to focus on PWAs’ self-initiated self-repair as self-initiations reflect detection of speech problems, which may be a skill that predicts good recovery from aphasia (R. C. Marshall et al., Citation1994). Self-repair of errors has also been associated with learning by Middleton et al. (Citation2022), who found enhanced learning in lexical access after self-initiated self-repair. Thus, we wanted to examine longitudinally how PWAs’ self-initiated self-repairs reflected their recovery from aphasia.
Research on the association of PWAs’ self-initiated self-repair with recovery from aphasia is still limited. Furthermore, most research evidence on self-repair and recovery is based on PWAs’ picture naming errors and the detection and repair of these errors, and not connected speech (e.g., R. C. Marshall et al., Citation1994; Middleton et al., Citation2022; Schwartz et al., Citation2016). Studying naming tasks of 30 people with different aphasia types and severities, R. C. Marshall et al. (Citation1994) found that greater pre-treatment self-initiation efforts, rather than the actual success of self-repair, predicted better recovery after three months of language treatment. More self-initiation effort and better outcomes according to cognitive-linguistic outcome measures were found by patients with better auditory comprehension and anomic or conduction aphasia rather than Wernicke’s or global aphasia. Based on these findings, R. C. Marshall et al. (Citation1994) suggested that self-repair could be one factor predicting aphasia treatment outcomes. Similarly, Schwartz et al. (Citation2016) found self-repair in naming tasks to be associated with aphasia treatment outcomes by patients with chronic mild-to-moderate aphasia and good comprehension. In contrast with R. C. Marshall et al. (Citation1994), in Schwartz et al.’s (Citation2016) study of 12 PWA, successful self-repair of semantic naming errors, that is, actual success, not just self-initiation, were associated with better outcomes. Improvement was interpreted as a learning effect. In addition, Middleton et al. (Citation2022) found learning from errors to be related to successful self-repair: if PWAs self-repaired naming errors spontaneously, they named those items more accurately at later sessions. The study concluded from this that vocabulary was learned incrementally through the successful correction of words.
Self-initiated self-repair in elicited naming tasks differs from the continuous spoken language typical of spontaneous conversation. In conversation, self-repair is essential for maintaining intersubjective understanding. Thus far, only a few studies have longitudinally examined repair in connected speech during recovery from aphasia. Recently, a study by Tetnowski et al. (Citation2021) pointed out the utility of examining speech problems (trouble sources) and repair as indices of improved communication in conversation. They found post-treatment changes in conversations of 20 people with different severities and mainly Broca’s or anomic aphasias: the trouble sources in PWAs’ speech decreased and the repair sequences shortened, but the changes in self-initiation of repairs and success of the self-repairs did not reach statistical significance. On the other hand, two case studies have shown different repair patterns when everyday conversations were examined pre and post a 2-month treatment: a participant with Broca’s aphasia produced more words to a conversation and self-repairs increased clearly (Boles, Citation1998), whereas conversation of a participant with mild aphasia did not show changes in the length of repair sequences (S. Fox et al., Citation2009). Thus, there may be variations in changes in connected speech in relation to the type or severity of aphasia.
Spared new word-learning ability has been associated with positive aphasia treatment outcomes (Dignam et al., Citation2016). Lexical learning is a complex process that requires perception and recognition of words and the association of words with meanings. People with aphasia have varying deficits in their lexical representations and associations with meanings, which restricts the use of common words in the study of learning abilities. The use of novel, not previously known vocabulary has been shown to be useful in the study of learning ability without complicating factors (Peñaloza et al., Citation2022, Citation2016; Tuomiranta, Càmara et al., Citation2014; Tuomiranta, Grönroos et al., Citation2014). Research has provided evidence for spared learning abilities in some participants with chronic aphasia, but the capacity to learn new content varies (Peñaloza et al., Citation2022). Nevertheless, people with severe aphasia can also learn novel vocabulary, and learning can show modality effects depending on auditory and visual stimuli (Tuomiranta, Càmara et al., Citation2014). It is noteworthy that new word learning has not been studied extensively in subacute aphasia, or followed longitudinally until the chronic phase (see, however, Tuomiranta et al., Citation2019).
According to previous research, both PWAs’ self-initiated self-repairs and learning of new words may reflect recovery from aphasia. In both cases, previous research is sparse and has mostly examined chronic aphasia or had short follow-ups. To find factors that may predict recovery from aphasia, we think self-repair and new word learning from the subacute phase until the chronic phase, 12 months after the onset of aphasia, ought to be studied. Moreover, we think connected speech should be studied to examine the proportion of self-initiated self-repair and the proportion of speech problems that are left unrepaired during speech production. Self-initiation of self-repair reflects the detection of problems, whereas unrepaired problems may show a lack of detection. Although closely related research is still sparse, we have also chosen to look for parallels between the learning of novel vocabulary and self-initiated self-repair/unrepaired problems.
The main research objectives in this study were to follow up on both new word learning capacity and production of self-initiated self-repairs at two stages of aphasia recovery, in the subacute phase and in the chronic phase, in four individuals with post-stroke aphasia. Additionally, it was our aim to study possible parallels between learning and self-repairing abilities. The nature of the present study is an exploratory trial as these topics have not, to our knowledge, been studied together before. The research questions were as follows:
Does the ability to self-initiate self-repair and detect problems in connected speech change from the subacute to chronic recovery phase?
Does the performance in new vocabulary learning change from the subacute to chronic recovery phase?
Is there any parallelism between self-initiated self-repairs and new vocabulary learning during recovery in each of the cases studied?
2. Materials and methods
2.1 Participants
Four PWA (one male) from a university hospital clinic volunteered to take part in the study (see for demographic data of the participants). They were all monolinguals, with Finnish as their mother tongue. Their ages varied from 52 to 58 years at the time of their respective strokes, and for each participant, the stroke suffered was their first. No other neurological conditions or developmental issues were found in their health-related histories. The etiology for the left-hemispheric stroke was an infarction for three of the participants (A, B, D), while one (C) had suffered a subarachnoidal hemorrhage.
Table 1. Demographic information on the participants.
At the time of the first part of the study, all participants were in the subacute phase of recovery from aphasia (max. 68 days post-stroke). Two of the participants, A and B, had a mild, anomic aphasia with an Aphasia Quotient (AQ) corresponding to a non-aphasic measure in the Finnish version of the Western Aphasia Battery Aphasia (WAB; Pietilä et al., Citation2005), while other clinical assessment methods (see section 2.3) confirmed the diagnosis of aphasia. The aphasia symptoms of the other two participants, C and D, were clearly more severe: C had Wernicke’s aphasia and D had global aphasia with limited comprehensible verbal output.
At the time of the second part of the study (12 months post-stroke), all participants were in the chronic phase and reported having received speech and language therapy regularly during the year. The two participants with anomic aphasia continued to have mild symptoms of anomic aphasia. According to the results in the WAB (Pietilä et al., Citation2005), the aphasia symptoms of participant A had continued to reduce, while participant B presented a slightly lower AQ than in the subacute phase. Participant C, with initial Wernicke’s aphasia, had recovered to the extent that her aphasia could be classified as conduction aphasia. Participant D’s initial global aphasia had evolved into Broca’s aphasia, but his verbal output was still limited.
2.2 Timeline
The study was conducted at two stages of recovery from aphasia. The participants were first tested in the subacute recovery phase (min. 11 days post-stroke; max. 68 days post-stroke) at an inpatient rehabilitation unit. Aphasia tests were administered by the employed speech-language therapists of the rehabilitation unit and willing individuals were given information about the study. If they gave their consent, the first session of the new word learning task followed, administered by speech and language therapy master’s students. Exactly one week later, the participant was administered the maintenance test of the learning task as well as the rest of the cognitive-linguistic tests and tasks designed for obtaining connected speech samples.
At 12 months post-stroke, the participants were contacted and recruited to the second part of the study in the chronic recovery phase. This part took place either in the participants’ homes or at the university clinic (1 participant chose this option). The new word learning experiment was administered during the first session of the chronic phase, followed by the maintenance test at the beginning of the second session (one week after the first session) and cognitive-linguistic background tests as well as connected speech tasks thereafter. Depending on the severity of aphasia, a total of 3–4 sessions were required to complete the procedure in the chronic phase. All tests of the chronic recovery phase were conducted by master’s students in speech and language therapy.
2.3 Cognitive-linguistic tests, connected speech samples, and the new word learning procedure
All participants were tested prior to starting the first learning experiment in the subacute recovery phase with a test battery consisting of the Finnish version of the Western Aphasia Battery (WAB; Pietilä et al., Citation2005) and the Finnish version of the Boston Naming Test (BNT; Laine et al., Citation1997). Smaller scale tasks administered included a verbal short-term memory task and repetition of pseudowords from the Finnish version of the Temple Assessment of Language and Short-Term Memory in Aphasia (TALSA; Martin et al., Citation2018; Tuomiranta et al., Citation2009), as well as narration tasks including picture description and narration in relation to the topic “why are you in the hospital, tell me what happened”. At 12 months post-onset, the latter task was replaced with a theme interview on the first year post-stroke and aphasia symptoms. The theme interview was not structured but was designed to flexibly, with additional questions, ensure a maximal amount of connected speech data. All tests and tasks were either audio or video recorded.
The computerized new word learning experiment followed a setup originally created for an earlier study (Peñaloza et al., Citation2016), but with the addition of orthographic input to aid learning. Two separate versions of the experiment were created to be administered in the two recovery phases. The stimuli in both experiments consisted of 6 line drawings of unfamiliar but real objects of the Ancient Farming Equipment paradigm (Laine & Salmelin, Citation2010) and 6 trisyllabic pseudowords (CVCVCV) that followed the phonotactic rules of Finnish (see example in ). The complexity of the pictured stimuli and the bigram frequency of the pseudowords were matched across experiment versions. The auditorily presented pseudowords were created using Google Text-to-Speech (Google Text-to-Speech).
Figure 1. The computerized learning task: one example trial with feedback. The response is depicted as a colored circle. In this example, the participant has pushed the left mouse button. This was the correct response; a smiling emoji is shown as feedback.
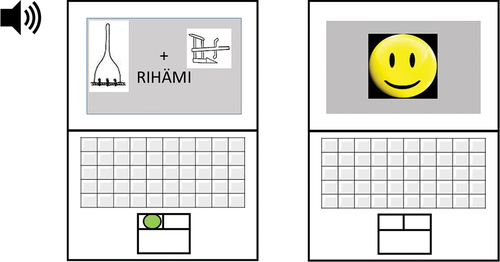
The experiment was performed using Presentation® software (Presentation® Software (Version 20.1)) on a laptop computer equipped with headphones and a touchpad mouse. The learning experiment consisted of a total of 210 learning trials, divided into 7 training blocks of 30 trials in each. In each trial, two pictured stimuli were presented simultaneously on the computer screen side by side, with a fixation cross between them. Simultaneously with the appearance of the pictured stimuli, the participant both heard and saw (in written form) below the pictures a pseudoword that was the correct match for one of the two pictures. The written word was displayed for 1 sec, which matched the average duration of the auditorily presented pseudowords. The pictured two stimuli remained on the screen until the participant selected one by pressing either the left or right button of the touchpad mouse. Following the response, the participant received immediate feedback on the accuracy of the response in the form of either a happy or a sad emoji. In each training block, each stimulus picture appeared 5 times as the correct choice and 5 times as the incorrect one. Moreover, the position of the pictures was balanced so that the correct option was the right-side picture as often as it was the left-side one. The test instructor sat beside the participant during the whole experiment and observed the performance in order to check for signs of fatigue, possible attentional decline, or perseveration of actions. The participants were able to rest after each of the 7 training blocks if they wished. After finishing the last training block, all participants were requested to take a short break. Following the break, the experiment continued with a recognition test that was similar to the training block but did not include feedback on the responses.
2.4 Analysis of the connected speech samples
Connected speech samples were obtained with WAB picture description (Pietilä et al., Citation2005), WAB interview (Pietilä et al., Citation2005), and theme interview questions. The samples were first transcribed from audio files. In the subacute phase of aphasia recovery, the duration of raw data with connected speech totaled 14 minutes. In the chronic phase, the duration of the raw data totaled 49 minutes. Together, the connected speech samples of the participants comprised 63 minutes (see Appendix 1).
Self-initiated self-repairs of speech were first analyzed qualitatively using conversation analysis. Self-repairs were identified, and the elements of the self-repair were segmented and annotated utilizing ELAN Computer software (ELAN computer software, version 5.9). In the present study, self-repair segments were defined as follows: i) the self-repair was verbally initiated by the aphasic speaker by interrupting speech, ii) the initiation was followed by self-repair elements, and iii) the self-repair segment was finished by the speaker, that is, the speaker did not continue repairing after the segment. As self-initiated self-repair segments in aphasia are complex, we chose to classify and count all the elements of self-repair to obtain a measure of their complexity (see and Examples 1 and 2 below for more detail Appendix 2).
Table 2. Definitions and examples of the different self-repair element types. The elements are presented in bold style.
By elements of self-repair, we refer to any instances of an attempt to repair ongoing speech or signs of word searching. The eleven different self-repair element types with examples from the data are presented in . These self-repair element types (pausing, non-lexical vocalization [e.g., uh], sound stretch within a word, cut-off word, repair particle [in Finnish, “eiku”, appr. “no I mean”], demonstrative pronoun, repetition, search question, meta-comment, and re-formulation) have previously been shown to be the most typical ones in Finnish aphasia data (Laakso, Citation1997; Laakso & Lehtola, Citation2003), and similar self-repair elements have also been observed in other languages, including English (Fox et al., Citation2010). One specification, adding a category of “filler word”, was made to the classification of elements based on the present data and more recent research (e.g., Wiklund & Laakso, Citation2021). All eleven self-repair element types were annotated with a separate tier in the ELAN template. Intersecting elements were counted separately, that is, if two types intersected, both types were added to the count to examine all elements of self-initiated self-repair in complex connected speech of the PWAs. All self-initiated self-repair segments, whether successful or not, were analyzed similarly.
In Example 1, PWA tells of the sudden beginning of her illness. In line 1, she cut-offs (indicated with a hyphen) and replaces a potential time expression (l- Monday night) and goes on to self-repair it further with a repair particle (no I mean Tuesday) and another cut-off (n- night before). The self-repair segment ends when the story continues (line 2). The self-repair segment has been underlined.
Example 1. A self-initiated self-repair segment (underlined) produced by participant B in the subacute phase. Free translation into English is presented in bold style under the original Finnish. The transcription conventions are explained in Appendix 2.
1 B: mä sain semmossen kohtauksen l- maanantaiyönä ≥e’ku≤ tiis-taiy- vastasena yönä
I had kind of seizure l- on Monday night ≥no I mean≤ Tues-day n- night before
2 (1.2) et mä en päässy sängyst ylös
(1.2) so that I couldn’t get out of bed
In Example 2, there are several self-initiation elements, including word searching. In line 1, there is sound stretch (vih:ree, “green”), cut-off (vih-), pronoun “tommosen” (that kind of), a repair particle “eiku” (no I mean), and search question combined with neologisms (what sainaks kuds). The neologisms were annotated as an unrepaired problem segment consisting of two words, as no self-repair was produced after them. In line 2, there is a phonemic re-formulation (saas > taas), and in line 3, there is a meta comment (I don’t know why I cannot say).
Example 2. A complex self-repair segment with unrepaired problems (underlined) was produced by participant C in the chronic phase. Self-repair and self-initiation elements have been underlined. Translation into English in bold. Neologisms in italics (not translated).
1 C: ja sit v on viel (.) vih:ree (.) vih- (.) tommosen (.) sairaan eikum mikä sainaks kuds (.)
and then v is also (.) gre:en (.) gre- (.) that kind of (.) sick no, I mean what sainaks kuds (.)
2 taas mä SAAS taas mul jäi (.) huk hukkaamatta tää (.)
again I SAAS {taas = again} again I left (.) los losing without this (.)
3 mä en tiiä miks mä en saa sanottuu
I don’t know why I cannot say
In statistical analysis, self-initiation elements were divided into three distinct groups: pausing, verbal self-initiation, and re-formulation to form bigger samples. Pausing as such does not indicate self-repair but is connected to speech difficulties and repair activities, verbal self-initiation elements reflect initial and ongoing effort to self-repair, and re-formulation provides the actual repair.
With the unrepaired problem segment, we refer to speech containing errors (such as paraphasia or neologisms) or lacking content (such as empty speech) with no evident self-repair elements during the production of the word(s) or utterance (see Example 3 with unrepaired neologisms). Unrepaired problem segments may reflect defects in the speech monitoring system (J. Marshall et al., Citation1998).
Example 3. Two unrepaired problem segments (underlined) produced by participant C in the subacute phase during the picture description of WAB (Pietilä et al., Citation2005). The comments of the speech and language therapist (T) administering the test are included. Translation into English in bold. Neologisms in italics (not translated).
1 C: sitten on oiva lanki (1.1) ne pääsee järrvellä käymään (.) ne käy siel kattomas
then that’s fine lanki (1.1) they get to the lake (.) they go there to look at
2 T: joo-o (2.85) nii
yeah (2.85) yes
3 C: (1.4) ripantteja
(1.4) ripantteja
4 T: mm-mh
Inter-annotator reliability of the classification of self-initiated self-repair elements and unrepaired problem segments was analyzed of 10% (equaling 6.2 minutes and including data of all participants) of the data. The agreement on the identification and classification was high.
For statistical analysis, quantitative data on the samples was extracted in the form of the number of self-repair elements and unrepaired problem segments. The length of unrepaired problem segments was calculated as the number of words. Both the number of self-initiation elements and the number and length of unrepaired problem segments were contrasted with the total number of words in every sample to measure the proportions of self-repair elements and unrepaired problem segments in total speech.
For statistical analysis of change of cognitive-linguistic measures and self-repair phenomena (i) pausing, ii) production of verbal self-repair elements, and iii) re-formulations) as well as of unrepaired problem segments from the subacute to the chronic recovery phase, we applied Chi-Square Test/ Fisher’s Exact Test. All dependent variables measuring change during recovery of aphasia from the subacute to the chronic stage can be seen in .
Table 3. Dependent variables measuring change during recovery of aphasia from subacute to chronic stage.
Table 4. The changes observed in cognitive-linguistic measures from the subacute test (0–3 months post-stroke) to the chronic test (12 months post-stroke) as well as aphasia types of all participants at both time points.
Figure 2. The proportion of self-repair elements (pausing, verbal self-repair elements, and re-formulations) out of total words in the speech samples per participant. A–D, participant IDs; Sub, subacute phase; chro, chronic phase.
Figure 3. The proportion of words produced during unrepaired problem segments out of total words in the speech samples. A–D, participant IDs.
Statistical power suffered from the small sample size. The distributions are therefore presented as graphs on the proportions of total words produced.
2.5 Analysis of the new vocabulary learning data
Raw points achieved in the vocabulary learning experiment were collected from the log files of the Presentation software (Presentation® Software (Version 20.1)) separately for each participant at both time points for each of the 7 training blocks, as well as the recognition tests administered immediately after the training and 1 week later (max. 30 points in each). The mean of the raw points was also calculated for each participant over training sets 1–7. Raw points of 21 or higher were classified as significantly differing from the chance level and, therefore, demonstrating learning (Binomial test, p = .043). A participant achieving at least 21 raw points in the majority of the learning sets was classified as a successful learner with feedback. The same 21 raw points limit was utilized in the recognition test to separate participants that could also show their learning without feedback, and in the maintenance test 1 week post-training to show successful memory consolidation of the learned stimuli.
2.6 Analysis of the parallelism of self-repairs and new vocabulary learning
Parallels between self-repairs in connected speech and the vocabulary learning task was first studied on the individual participant level and then on the group level. As the first variable for self-repairs, we used the number of all self-repair elements produced in the speech samples divided by the total word count of the samples (proportion of self-repair). The second variable was the total word count of unrepaired problem segments divided by the total word count of the samples (i.e., the proportion of unrepaired problems).
For the new vocabulary learning ability, we had two variables: i) the raw points of recognition test and ii) the raw points of maintenance test. We used the raw points of the recognition test for analyzing the parallels between learning and self-repair to see if immediate learning ability was associated with spontaneous detection and repair of speech problems. Recognition raw points were chosen because they presented the widest variation between the participants in the subacute phase. Due to the small sample size, we applied scatter plots for each participant and for both recovery phases. Finally, we compared the participant-wise association of these variables in the acute and chronic phases side by side.
2.7 Study ethics
The study was reviewed and approved by the Helsinki University Hospital Ethics Committee. All participants provided their written informed consent to participate in the study. Researchers involved in handling the data signed their commitment to ethical principles in relation to confidential data.
3. Results
Cognitive-linguistic measures of aphasia recovery and the results of self-initiated self-repairs in connected speech are reported case by case in sections 3.1 and 3.2. Section 3.3 focuses on new vocabulary learning on both the individual and group levels, and section 3.4 focuses on parallels between self-repairs and new vocabulary learning.
3.1 Cognitive-linguistic measures of aphasia recovery
According to the cognitive-linguistic measures, all participants showed some recovery of aphasia from the subacute to the chronic phase (see ). The change was more substantial in the test results of participants C and D with more severe aphasia, but participants A and B with mild aphasia and high AQ in the subacute phase also showed a change in their picture naming results.
3.2 Self-repairs of connected speech and unrepaired problem segments
Self-repairs of connected speech differed according to the type and severity of aphasia (see ) and showed a change from the subacute phase to the chronic phase. However, for the self-repair phenomena and unrepaired problem segments, there was not enough statistical power because of the small amount of data, and, consequently, no statistical significance was found in the data. The proportions of self-repair elements (pausing, verbal self-initiation elements, and re-formulations) per total words produced are presented in and unrepaired problem segments in for each participant from the subacute to the chronic phase. Detailed information on the distribution of self-repair element types (pausing, non-lexical vocalization/ hesitation, sound stretch, cut-off of a word, repair particle, demonstrative pronoun, repetition, filler word, searching by question, meta comment, and re-formulation) is shown in . In the subacute recovery phase, silent pause was the most frequent element in all self-repairs of the participants’ connected speech, while later in the chronic phase, the most frequent type varied.
Table 5. The percentages of different self-repair elements in all self-repair segments of connected speech by participants A – D in two time points: the subacute (0–3 months post-stroke) and the chronic (12 months post-stroke) phase of recovery from aphasia.
3.2.1 Participant A
Participant A already had mild anomic aphasia in the subacute phase of recovery. Her verbal output was fluent with no paraphasia but contained pauses related to word searches. The same description applies to her output in the chronic phase. Accordingly, most of her self-repair elements were silent pauses in both phases of recovery (see and ). From the subacute to the chronic phase, the proportion of all self-repair elements of all produced words decreased from 12.5 to 4.6% during connected speech samples. Similarly, the unrepaired problem segments of participant A, as measured by number of words, decreased from 8.3% in the subacute phase to 1.0% in the chronic phase (see ).
3.2.2 Participant B
Participant B also had mild aphasia. Her output was fluent, with some evidence of anomia. In the subacute phase, B produced silent pauses but also a wide variety of verbal self-repair elements, including hesitant vocalizations, cut-off words, repair particles, repetitions, and pronouns instead of more specific words (see ). She also produced some re-formulations (see ). In the chronic phase, the proportion of pausing and verbal self-repair elements decreased, but re-formulations increased. The percentage of all self-repair elements of the total word count decreased during the follow-up period (19.4% vs. 12.9%; ). Unrepaired problem segments were almost non-existent in participant B’s connected speech in both recovery phases (see ).
3.2.3 Participant C
In the subacute phase of aphasia recovery, participant C was diagnosed with typical Wernicke’s aphasia with fluent but paraphasic speech production with neologisms. At 12 months post-stroke, her aphasia had become milder and was classified as conduction aphasia. Paraphasia was still present, but neologisms were fewer. In both recovery phases, participant C used a large scale of different self-repair elements (see ). The most frequent self-repair element was the silent pause in both recovery phases. In the subacute phase, she also produced many non-lexical vocalization/ hesitations, cut-off words, and re-formulations (see ). Other element types were more infrequent. In the chronic phase, the proportion of hesitant vocalizations of all self-repair elements decreased from 16 to 1%, and the most frequent types, besides the silent pauses, were cut-off words and re-formulations, reflecting self-repair of speech problems (). The proportion of self-repair elements of the total number of words in the connected speech samples remained almost the same during the follow-up (21.4% in the subacute sample, 20.0% in the chronic sample; see ). However, a clear reduction was seen in the proportion of unrepaired problem segments of the total amount of words in the connected speech samples (23.1% in the subacute sample, 8.0% in the chronic sample; see ).
3.2.4 Participant D
Participant D with global aphasia produced very limited connected speech in the subacute phase of aphasia recovery. In line with this, the occurrences of self-repairs were few. He answered questions in very few words, producing neologisms, but tried to continue speaking after the tester’s requests. At 12 months post-stroke, his global aphasia had resolved into Broca’s aphasia and his language production had become slightly more fluent, though still containing utterances that could be classified as neologisms. The total word count of connected speech did not notably grow from the subacute to the chronic phase. At both recovery phases, only a few self-repair element types were available to this participant (see ). Silent pause, repetition, re-formulation, and cut-off were the most frequent element types. In addition, he produced some non-lexical vocalization in the subacute phase and repetition and cut-off in the chronic phase. The percentage of self-repair elements of the total number of words reduced from the subacute phase (36.3%) to the chronic phase (24.6%; see ). At the same time, the percentage of unrepaired problem segments of the total word count reduced from 30.4 to 21.2% (see ).
3.3 New vocabulary learning
All participants showed some learning and maintenance of new vocabulary as measured by correct recognition of the items (at the minimum 21 accurate trials out of 30 in the recognition test, p = .043 in the Binomial test). depicts the learning and maintenance curves of all participants in the two recovery phases (subacute and chronic). In both phases, all participants completed the recognition test twice: immediately after the vocabulary learning experiment (measuring immediate learning) and again one week later (measuring maintenance). In cases of poor immediate learning or maintenance, learning with feedback, measured during the actual training, was also examined.
Figure 4. Learning and maintenance of new vocabulary by participants A–D in the subacute (0–3 months post-stroke) and the chronic (12 months post-stroke) phase of recovery from aphasia. Learning and maintenance are measured by accurate recognition of the items. The dashed line shows the level of significant performance as measured by the Binomial test.
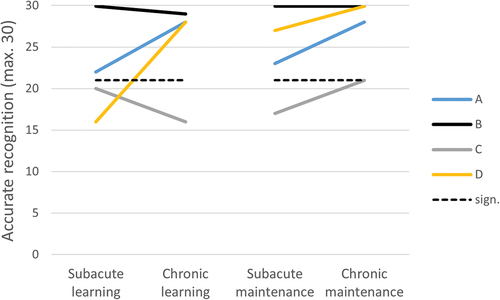
Participants A and B with mild anomic aphasia recognized a significant number of the learned items in all four recognition tests over the follow-up period. The performance of participant B was at the ceiling in 3 out of 4 tests, her only single error occurring in the immediate learning test of the chronic phase. Participant A performed better in the chronic phase than in the subacute phase. Participant C with initial Wernicke’s aphasia and later conduction aphasia only reached the level of significant performance in 1 out of the 4 recognition tests (the maintenance test of the chronic recovery phase). Interestingly, her recognition performance in the subacute phase dropped during the maintenance period, while the opposite occurred in the chronic phase. Learning with feedback (i.e., performance during actual training blocks with continuous feedback on performance) reached significance in only one training block, (the last block of the subacute phase). Participant D with the most severe aphasia performed at chance level in the immediate recognition test of the subacute recovery phase (and also in all training blocks), but all three later recognition tests (subacute maintenance and both tests of the chronic phase) showed high levels of learning and maintenance of the new vocabulary.
3.4 Parallels between new vocabulary learning and self-repairs of connected speech
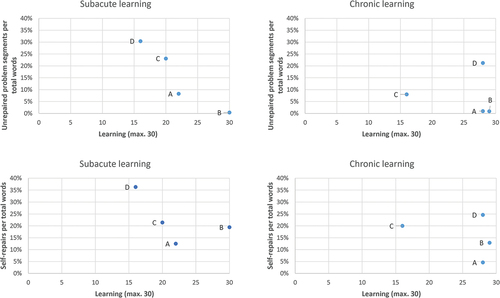
The parallels between new vocabulary learning with factors connected to self-repairs, that is, the proportion of self-repair elements and the proportion of unrepaired problems in total speech, were observed using scatter plots (see ). We looked at the initial learning both in the subacute and chronic recovery phases. Regarding the proportion of self-repair elements, we looked at Self-repair elements/number of words in sample (%) produced during connected speech, and as a second measure regarding proportion of unrepaired problems, Words in unrepaired problem segments/number of words in sample (%) in connected speech. The scatter plots of show pairwise the change in problem segments and vocabulary learning (top row) and self-repairs and vocabulary learning (bottom row) from the subacute to the chronic phase. Participant A with anomic aphasia left fewer problem segments unrepaired and produced fewer self-repairs as her vocabulary learning improved. The other participant with anomic aphasia (B) performed at the ceiling in relation to vocabulary learning and left no problem segments unrepaired in the subacute phase. However, a decrease was seen in the proportion of self-repairs in her connected speech from the subacute to the chronic phase. Participant C, with initial Wernicke’s aphasia resolving into conduction aphasia, left fewer problem segments unrepaired in the chronic than the subacute phase, while the proportion of self-repairs in her connected speech decreased only slightly. In learning, her results weakened. Participant D, with initial global aphasia resolving into Broca’s aphasia, showed, contrary to C, a systematic improvement in relation to unrepaired problems, self-repairs, and vocabulary learning.
Figure 5. On the top row: The proportion of words produced by participants A–D during unrepaired problem segments in the subacute and the chronic phase out of total words in the speech samples. On the bottom row: The proportion of self-repair elements (pausing, verbal self-repair elements, and re-formulations) in the subacute and the chronic phase out of total words in the speech samples.
4. Discussion
The present explorative trial followed up on self-repair and new word learning in four participants with post-stroke aphasia, from the subacute phase of recovery to the chronic phase. We are not aware of earlier longitudinal reports on new word learning in aphasia, and the findings on the development of self-repairs in aphasia are contradictory and little studied. In addition, the study explored the possible parallels between learning capacity and the self-repairs of connected speech. Although some related research concerning the association between self-repairs and aphasia treatment outcomes is available (Boles, Citation1998; R. C. Marshall et al., Citation1994; Schwartz et al., Citation2016; Tetnowski et al., Citation2021), the parallels between self-repairs and learning of novel vocabulary have not previously been examined.
4.1 Discussion of the results
4.1.1 Changes in self-initiated self-repairs and unrepaired problems in connected speech from the subacute to the chronic recovery phase
All four participants, despite differing aphasia types and severities, initiated self-repairs during connected speech, both in the subacute and the chronic recovery phases. The types of self-repair elements were in line with earlier research conducted with Finnish aphasia data (Laakso, Citation1997; Laakso & Lehtola, Citation2003; Laakso, Citation2015). Pausing was clearly shown in the self-repairs of all participants, which is similar to previous research (Samuelsson & Hydén, Citation2017). What has not previously been observed but which we observed in our study, is qualitative changes in the use of self-repair elements from the subacute phase to the chronic phase. The proportion of silent pauses, sound stretches, and non-lexical vocalizations decreased, and cut-off words and re-formulations, reflecting more efficient self-repair, increased. Quantitative changes in the number of self-repairs and unrepaired problems were also seen from the subacute to the chronic aphasia recovery phase. Firstly, the proportion of self-repair of the total word count decreased in all four participants. Secondly, we found that the proportion of unrepaired problem segments decreased from the subacute to the chronic phase in the three participants who notably produced them. Decreases in self-repair and unrepaired problems are in line with the results of an earlier study on conversational speech (Tetnowski et al., Citation2021). However, as in this earlier study, in our data these changes did not reach statistical significance. The findings are also similar to the finding that attempts to self-repair speech in the subacute phase correlate with recovery from aphasia (Marshall et al., Citation1994). Similar observations on decreasing self-repair in our study and these two studies are of particular interest, as the design of the previous studies differs from the design of the present one in many ways (e.g., institutional conversation in Tetnowski et al., Citation2021 or naming tasks in Marshall et al., Citation1994 vs. connected, interview, and monologue speech in the present study). This suggests that self-repair behavior could be used as a measure of recovery, independent of which kind of speech data is used. However, the small number of studies in this regard calls for caution in generalizing the results.
If we look at the four cases individually, the aphasia recovery paths can be seen to differ. The aphasia of both A and B were of a mild anomic type, but the changes in self-repair and unrepaired problems were different. Compared to B, A had fewer self-repair elements and more unrepaired problem segments in the subacute phase but self-repaired most of her speech problems in the chronic phase, thus becoming more efficient in self-repair. B had more self-repair elements, but very few unrepaired speech problems in the subacute phase. B thus detected and self-repaired her speech problems already in the subacute phase, and self-repairs decreased in the chronic phase. The observed variation in mild anomic aphasia is not in line with the earlier observations that more self-repair can be found by participants with anomic aphasia (e.g., R. C. Marshall et al., Citation1994). The initial Wernicke’s aphasia of participant C resolved to conduction aphasia in the chronic phase. C produced self-repair segments of relatively stable frequency during the follow-up, but the proportion of unrepaired problem segments decreased clearly. Thus, it seems that, similarly to A, participant C succeeded better in self-repairing her verbal output in the chronic phase of recovery than in the subacute phase. This observation of improvement in the detection and self-repair of neologistic errors is in line with some earlier reports on Wernicke’s aphasia (R. C. Marshall et al., Citation1994) or jargon aphasia (Eaton et al., Citation2011). The only non-fluent participant of the present study (D) had initial global aphasia, which resolved to Broca’s aphasia in the chronic phase. For participant D, both the proportion of self-repaired and unrepaired problem segments decreased. In other words, as his speech production improved, participant D produced fewer self-repairs and fewer unrepaired problem segments in the chronic phase than in the subacute phase. Still, in his speech, the proportion of self-repairs and problem segments was greater than it was for the other participants. The decrease in D’s self-repair is in contrast with a single-case study of Broca’s aphasia, in which self-repairs tripled after treatment (Boles, Citation1998). However, the multi-case design with a small number of participants does not allow strong conclusions to be drawn on the effect of aphasia severity or type on the self-repair results.
4.1.2 New word learning
All four participants showed significant capacity to acquire new vocabulary in the chronic recovery phase, three of them (A, B, and D) already in the subacute phase. Wide variation in new word learning and maintenance ability in chronic aphasia has been observed in earlier research (Dignam et al., Citation2016; Peñaloza et al., Citation2016; Tuomiranta, Càmara et al., Citation2014; Tuomiranta, Grönroos et al., Citation2014; Tuomiranta et al., Citation2012), but evidence is limited for non-chronic aphasia (Tuomiranta et al., Citation2019). In the present study, the widest variation in performance was seen in the immediate recognition test of the subacute phase. The two participants with the most severe aphasia did not reach a performance level significantly better than that of chance. At the same time, the performance of participant B with mild anomic aphasia was at the ceiling. At one week post-training (maintenance test), the performance of participants A and B with mild anomic aphasia stayed stable, while the performance of participant C dropped and participant D with global aphasia showed a steep rise in performance, outperforming participant A. Successful new word learning and maintenance has previously been reported in severe aphasia (Tuomiranta, Càmara et al., Citation2014), but not in an experiment with word-referent ambiguity, such as the present one (Peñaloza et al., Citation2016). The present experimental design differed from the earlier design of Peñaloza and colleagues by the addition of orthographic input. The addition was made due to the earlier observation of significant orthography-based but poor auditory learning ability in at least some PWA (Tuomiranta, Càmara et al., Citation2014) to ensure the possibility of learning for participants with this learning profile.
Participants A and B with mild anomic aphasia could learn and maintain vocabulary at both time points: in the subacute and chronic recovery phases. Participant A performed at a higher level in the chronic phase than the subacute phase of recovery, possibly reflecting functional recovery in her learning-related neural networks. Participant B performed at the ceiling in both phases, which makes further conclusions on her recovery out of reach. Like participant A, participants with more severe aphasia, C and D, also improved in their learning results from the subacute to the chronic phase. The accuracy of participant C’s responses declined to the maintenance test of the subacute phase, but in the chronic phase, she reached significant learning in the maintenance test. Participant D, with the most severe aphasia, did evidently learn at a high level already in the subacute phase, even though his immediate recognition accuracy was low. The maintenance test 1 week post-training, with no training between the tests, showed high accuracy (90%), with participant D outperforming 13/14 of the chronic participants of the earlier study by Peñaloza et al. (Citation2016), all of whom actually had less severe aphasia than participant D.
It is essential to bear in mind that the present experiment was modified from the original one (Peñaloza et al., Citation2016) in relation to input modalities. Still, keeping in mind the word-referent ambiguity of the experiment set-up, a closer reference point cannot be found in aphasia research, as the vast majority of learning studies of aphasia have been conducted with simple associative learning tasks with no ambiguity (Peñaloza et al., Citation2022). In the chronic recovery phase, the immediate recognition accuracy of participant D was more in line with his maintenance accuracy than in the subacute phase. These results pointed to a high level of learning and full maintenance of the novel word-reference pairs. In spite of his severe aphasia, he showed a higher level of learning than participant A with mild aphasia. Earlier evidence of novel word learning in aphasia emphasizes the probable multifactoriality of succeeding in this task, as the variability in learning profiles is wide. The effect of aphasia severity on learning has been found in previous studies (Dignam et al., Citation2016; Peñaloza et al., Citation2016), but some cases have shown excellent learning ability and long-term maintenance despite moderate aphasia (Tuomiranta, Càmara et al., Citation2014; Tuomiranta, Grönroos et al., Citation2014). Participant D of the present study, despite severe aphasia, is clearly one of the strong learners, having outperformed participant A with mild aphasia, and so no effect of aphasia severity on learning can be seen in the present study. In sum, all participants showed learning and maintenance of learning results in both phases of aphasia recovery, but the pace of their learning varied.
4.1.3 Parallels between self-repairs and new vocabulary learning
Novel word learning and self-initiated self-repairs did not change in a clearly parallel manner from the subacute phase to the chronic phase. Participants who had large proportions of unrepaired problem segments in connected speech performed weaker on the new vocabulary recognition test in the subacute phase. This suggests that a lack of self-repair of problems may be related to weaker learning of new words, in line with Middleton et al. (Citation2022), who found self-repair of errors to be connected to learning. However, in the chronic phase, this was not true, as D had more unrepaired problems than C, but learned better. Furthermore, in the chronic phase, more self-repair effort (i.e., more self-repair elements produced per total word count), did not coincide with better learning, as C with high self-repair effort was poor in learning, and the other three participants, A, B, and D, performed very well although their self-repair efforts varied.
If we now shift the focus onto the actual learning capacity and long-term maintenance of the novel word-referent pairs, no relationships with measures of self-repairs can be found in this limited multi-case data. Novel word learning has been shown to rely on multiple neural networks and the functionality of one of them – the episodic-lexical interface – is essential for long-term learning of new material. This interface enables the fast mapping of words and their referents together and, finally, memory consolidation (Rodríguez-Fornells et al., Citation2009). These phases have been shown to be functional in many PWA, too. Depending on the integrity of this interface, PWA may show good or poor learning regardless of how severe or mild their aphasia is or how they succeed in detecting problems and initiating self-repair in their speech. However, these findings need to be tested with a larger sample.
4.2 Discussion of the data and methods
Some limitations concerning the data and methods need to be highlighted. The present study had a longitudinal multi-case design, but it was originally planned as a group study. Data collection had to be interrupted in March 2020 due to the COVID-19 pandemic. Consequently, the data are limited, albeit motivated by a desire to explore a new area of research. Two of the participants had mild aphasia, which implies that extensive recovery was not possible for them, while it was possible for the more severe participants during the follow-up period. This may lower the validity of the data. Furthermore, the cognitive-linguistic test battery had to be kept short for practical reasons when conducting the experiment in the hospital rehabilitation unit.
Regarding self-repairs, it is important to keep in mind that the incidence of self-repairs, even produced by the same speaker, may vary from one situation to another in a free conversation (Laakso, Citation1997). For this reason, the connected speech samples were collected in similar situations in both the sub-acute and chronic phases. The results from connected speech may not be generalized to natural, everyday conversations. Promisingly, the results of self-repair phenomena were nevertheless in line with previous studies on conversational (Tetnowski et al., Citation2021) and naming performance (R. C. Marshall et al., Citation1994) data.
The abovementioned facts naturally complicate the application of the results. Nevertheless, this study provides new longitudinal follow-up data on aphasia, on both novel word learning and self-initiated self-repairs of connected speech. Furthermore, the possible relationship between learning and self-repair is explored.
4.3 Conclusions
Decreasing self-initiated self-repairs of connected speech reflect recovery from aphasia, but potentially in different amounts and paces depending on aphasia type and severity. The proportion of unrepaired problem segments decreases from the subacute to the chronic phase. Novel-word learning improves during aphasia recovery from the subacute to the chronic phase but may show a different pattern in fluent aphasia. Novel word learning is possible even in subacute, severe non-fluent aphasia and even in an ambiguous task set-up with no explicitly provided word-referent connections. No clear parallels between novel word learning and self-initiated self-repairs were found in the present study, but these findings need to be tested with a larger sample.
7 Author contributions
L.T. took on the main responsibility for writing the manuscript, designed and supervised the data collection, and analyzed part of the data. L.E. took part in writing the manuscript, designed the classification for self-repairs, annotated and analyzed all of the self-repair data, and took part in the data collection. M.L. took part in writing the manuscript and supervised and interpreted the analysis of the self-repair data.
Acknowledgments
We would like to thank all of the participants for their enthusiastic participation, the master’s students who collected most of the data, clinical speech-language therapists Taina Jääskeläinen, Riitta-Leena Manninen, Johanna Rantanen, and Noora Rautiainen, neurologist Eeva Karhunen at Helsinki University Hospital, who referred the participants to this study, and professor Jyrki Tuomainen and University of Helsinki biostatisticians, who provided expertise in statistical analysis.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Basso, A. (2003). Aphasia and its therapy. Oxford University Press.
- Boles, L.(1998). Conversational discourse analysis as a method for evaluating progress in aphasia: A case report. Journal of Communication Disorders, 31(3), 261–273. https://doi.org/10.1016/s0021-9924(98)00005-7
- Dignam, J., Copland, D., Rawlings, A., O’Brien, K., Burfein, P., & Rodriguez, A. D. (2016). The relationship between novel word learning and anomia treatment success in adults with chronic aphasia. Neuropsychologia, 81, 186–197. https://doi.org/10.1016/j.neuropsychologia.2015.12.026
- Eaton, E., Marshall, J., & Pring, T. (2011). Mechanisms of change in the evolution of jargon aphasia. Aphasiology, 25(12), 1543–1561. https://doi.org/10.1080/02687038.2011.624584
- ELAN computer software (Version 5.9). (2020). Max Planck Institute for Psycholinguistics. The Language Archive. Retrieved from https://archive.mpi.nl/tla/elan.
- Fox, S., Armstrong, E., & Boles, L. (2009). Conversational treatment in mild aphasia: A case study. Aphasiology, 23(7–8), 951–964. https://doi.org/10.1080/02687030802669526
- Fox, B., Maschler, S., & Uhmann, S. (2010). A cross-linguistic study of self-repair: evidence from English, German and Hebrew. Journal of Pragmatics, 42(9), 2487–2505. https://doi.org/10.1016/j.pragma.2010.02.006
- Google Text-to-Speech. https://cloud.google.com/text-to-speech
- Harvey, D. Y., Parchure, S., & Hamilton, R. H. (2022). Factors predicting long-term recovery from post-stroke aphasia. Aphasiology, 36(11), 1351–1372. https://doi.org/10.1080/02687038.2021.1966374
- Laakso, M. (1997). Self-initiated repair by fluent aphasic speakers in conversation. sstudia Fennica Linguistica 8. Finnish Literature Society.
- Laakso, M.(2015). Collaborative participation in aphasic word searching: Comparison between significant others and speech and language therapists. Aphasiology, 29(3), 269–290. https://doi.org/10.1080/02687038.2013.878450
- Laakso, M., & Lehtola, M. (2003). Sanojen hakeminen afaattisen henkilön ja läheisen keskustelussa. Puhe ja Kieli, 23(1), 1–24. https://journal.fi/pk/article/view/8079
- Laine, M., Koivuselkä-Sallinen, P., Hänninen, R., & Niemi, J. (1997). the finnish version of the boston naming test. Psykologien Kustannus.
- Laine, M., & Martin, N. (2006). Anomia. theoretical and clinical aspects. Routledge.
- Laine, M., & Salmelin, R. (2010). Neurocognition of new word learning in the native tongue: Lessons from the ancient farming equipment paradigm. Language Learning, 60(s2), 25–44. https://doi.org/10.1111/j.1467-9922.2010.00599.x
- Levelt, W. J. M. (1983). Monitoring and self-repair in speech. Cognition, 14(1), 41–104. https://doi.org/10.1016/0010-0277(83)90026-4
- Marshall, R. C., Neuburger, S. I., & Phillips, D. S. (1994). Verbal self-correction and improvement in treated aphasic clients. Aphasiology, 8(6), 535–547. https://doi.org/10.1080/02687039408248680
- Marshall, J., Robson, J., Pring, T., & Chiat, S. (1998). Why does monitoring fail in jargon aphasia? Comprehension, judgment, and therapy evidence. Brain and Language, 63(1), 79–107. https://doi.org/10.1006/brln.1997.1936
- Martin, N., Minkina, I., Kohen, F. P., & Kalinyak-Fliszar, M. (2018). Assessment of linguistic and verbal short-term memory components of language abilities in aphasia. Journal of Neurolinguistics, 48, 199–225. https://doi.org/10.1016/j.jneuroling.2018.02.006
- Middleton, E. L., Schwartz, M. F., Dell, G. S., & Brecher, A. (2022). Learning from errors: Exploration of the monitoring learning effect. Cognition, 224, 105057. https://doi.org/10.1016/j.cognition.2022.105057
- Peñaloza, C., Martin, N., Laine, M., & Rodríguez-Fornells, A. (2022). Language learning in aphasia: A narrative review and critical analysis of the literature with implications for language therapy. Neuroscience and Biobehavioral Reviews, 141, 104825. https://doi.org/10.1016/j.neubiorev.2022.104825
- Peñaloza, C., Mirman, D., Tuomiranta, L., Benetello, A., Heikius, I.-M., Järvinen, S., Majos, M. C., Cardona, P., Juncadella, M., Laine, M., Martin, N., & Rodríguez-Fornells, A. (2016). Novel word acquisition in aphasia: Facing the word-referent ambiguity of natural language learning contexts. Cortex, 79, 14–31. https://doi.org/10.1016/j.cortex.2016.03.009
- Pietilä, M.-L., Lehtihalmes, M., Klippi, A., & Lempinen, M. (2005). The finnish version of the western aphasia battery. handbook. Kertesz, A. (1982). The Western Aphasia Battery. Psykologien Kustannus.
- Presentation® software (Version 20.1). (2017). Neurobehavioral Systems. www.neurobs.com
- REhabilitation and recovery of peopLE with Aphasia after StrokE (RELEASE) Collaborators. (2021).Predictors of poststroke aphasia recovery: A systematic review-informed individual participant data meta-analysis.Stroke, 52(5),1778–1787. https://doi.org/10.1161/STROKEAHA.120.031162. https://doi.org/10.1161/STROKEAHA.120.031162
- Rodríguez-Fornells, A., Cunillera, T., Mestres-Missé, A., & de Diego-Balaguer, R. (2009). Neurophysiological mechanisms involved in language learning in adults. Philosophical Transactions of the Royal Society of London Series B, Biological Sciences, 364(1536), 3711–3735. https://doi.org/10.1098/rstb.2009.0130
- Samuelsson, C., & Hydén, L.-C. (2017). Collaboration, trouble and repair in multiparty interactions involving couples with dementia or aphasia. International Journal of Speech-Language Pathology, 19(5), 454–464. https://doi.org/10.1080/17549507.2016.1221448
- Schegloff, E. A. (2007). Sequence organization in interaction: A primer in conversation analysis. Cambridge University Press. https://doi.org/10.1017/CBO9780511791208
- Schegloff, E. A., Jefferson, G., & Sacks, H. (1977). The preference for self-correction in the organization of repair in conversation. Language, 53(2), 361–382. https://doi.org/10.1353/lan.1977.0041
- Schwartz, M. F., Middleton, E. L., Brecher, A., Gagliardi, M., & Garvey, K. (2016). Does naming accuracy improve through self-monitoring of errors? Neuropsychologia, 84, 272–281. https://doi.org/10.1016/j.neuropsychologia.2016.01.027
- Tetnowski, J. T., Tetnowski, J. A., & Damico, J. S. (2021). Patterns of conversation trouble source and repair as indices of improved conversation in aphasia: A multiple-case study using conversation analysis. American Journal of Speech-Language Pathology, 30(1S), 326–343. https://doi.org/10.1044/2020_AJSLP-19-00100
- Tuomiranta, L., Càmara, E., Froudist Walsh, S., Ripolles, P., Saunavaara, J. P., Parkkola, R., Martin, N., Rodriguez-Fornells, A., & Laine, M. (2014). Hidden word learning capacity through orthography in aphasia. Cortex, 50, 174–191. https://doi.org/10.1016/j.cortex.2013.10.003
- Tuomiranta, L., Grönroos, A.-M., Martin, N., & Laine, M. (2014). Vocabulary acquisition in aphasia: Modality can matter. Journal of Neurolinguistics, 32, 42–58. https://doi.org/10.1016/j.jneuroling.2014.08.006
- Tuomiranta, L., Laine, M., & Martin, N. (2009). Adaptation of the Temple Assessment of Language and Short-Term Memory in Aphasia (TALSA) into the Finnish language. Unpublished Manual.
- Tuomiranta, L., Peñaloza, C., Manninen, R.-L., Parkkonen, E., Rantanen, J., Rautiainen, N., Martin, N., Rodriguez-Fornells, A., Laine, M., Laakso, M., Parkkonen, E., Rantanen, J., Rautiainen, N., Martin, N., Rodriguez-Fornells, A., Laine, M., Laakso, M., Rantanen, J., Rautiainen, N., … Laakso, M. (2019). New word learning under word-referent ambiguity in severe aphasia: Evidence from two case studies. Frontiers in Human Neuroscience, 13, 13. https://doi.org/10.3389/conf.fnhum.2019.01.00048
- Tuomiranta, L., Rautakoski, P., Rinne, J. O., Martin, N., & Laine, M. (2012). Long-term maintenance of novel vocabulary in persons with chronic aphasia. Aphasiology, 26(8), 1053–1073. https://doi.org/10.1080/02687038.2012.693583
- Wiklund, M., & Laakso, M.(2021). Comparison of disfluent and ungrammatical speech of preadolescents with and without ASD. Journal of Autism & Developmental Disorders, 51(8), 2773–2789. https://doi.org/10.1007/s10803-020-04747-2
Appendix 1
Words produced in the connected speech samples
Appendix 2
Key to transcription conventions
(.) pause indicating a word search
: stretched sound
si- unfinished word
n’t loss of a vowel
> < faster speech
< > slower speech
HEI raised voice
£ £ laughing voice.