
ABSTRACT
Background
Preeclampsia (PE) is one of the leading disorders in pregnant women with maternal and fetal complications. Obesity is considered an important risk factor for the development of PE. Genetic variations in fat mass and obesity associated (FTO) gene may play a role in the development of PE. This study aimed to investigate the possible association between FTO gene rs9939609 and PE risk in a sample of Iranian pregnant women.
Material and methods
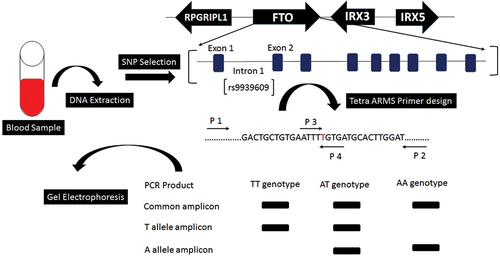
In this case–control study, 312 pregnant women were included, including 128 with PE and 184 without PE. Demographic data and blood samples were obtained from all individuals. The genotyping of rs9939609 polymorphisms was performed by the tetra‐primer amplification refractory mutation system‐polymerase chain reaction (TP‐ARMS‐PCR) method, and the results of TP‐ARMS‐PCR were confirmed using DNA sequencing.
Results
The genotype frequency was 50%, 47.7%, and 2.3% in pregnant patients and 37%, 47.8%, and 15.2% in healthy controls for TT, AT, and AA, respectively. The risk of PE was significantly reduced in the pregnant women having the AA genotype.
Conclusion
Based on the results of the present study, rs9939609 polymorphism in the FTO gene may play a protective role against PE. However, further studies are warranted.
Introduction
Preeclampsia (PE) is a pregnancy‑specific disorder that is clinically defined by hypertension (≥140/90 mmHg) and proteinuria (≥300 mg/day) after 20 weeks of gestation. The disease remains one of the leading causes of mortality and morbidity for both the mother and the fetus worldwide (Citation1–3). The incidence of PE is approximately between 3% and 8% of all pregnant women and up to 10% in developing countries (Citation4,Citation5). The pathogenic cause underlying PE is not fully understood; however, many risk factors may be involved in the development of PE, including maternal obesity, diabetes, chronic hypertension, and genetic factors (Citation6,Citation7).
Overweight and genetic factors account for 40–70% of the obesity-related causes, and obesity is the most common risk factor for PE (Citation8,Citation9). Therefore, finding the genetic markers for obesity and PE is clearly beneficial. One of the most common types of genetic markers in the human genome is single nucleotide polymorphisms (SNPs), which can be used to identify genes associated with complex diseases.
Several large-scale genome-wide association studies (GWAS) have shown that variations in the FTO gene, especially in the first intronic region of this gene, are associated with obesity (Citation10–12). Among all FTO gene variants, rs9939609 is of particular interest because it has a significant effect on obesity across different ethnicities (Citation13,Citation14). A meta-analysis from 12 case–control studies enrolling approximately 14,800 participants discovered that FTO rs9939609 polymorphism was significantly associated with the increased risk of obesity in children and adolescents (Citation15).
As obesity is an important risk factor for PE disorder and the FTO rs9939609 polymorphism has been associated with obesity in different populations, it is believed that another FTO polymorphism, rs9939689, increases blood pressure in Finnish and French Canadian women (Citation16,Citation17). However, few studies have been done on the effect of polymorphism of rs9939609 on PE. Our study examined the genetic relationship between the rs9939609 polymorphism and PE risk in Iranian women.
Material and methods
Study population
This study was a hospital-based case–control study that recruited 312 Iranian women (128 preeclamptic pregnant women as cases and 184 healthy pregnant women as controls). Written informed consent was obtained from all participants. The average age was 31.4, and 27.5 ± 5.2 years in the patients and controls, respectively. Study participants with chronic hypertension, diabetes mellitus, gestational diabetes, or kidney disease were excluded.
Genotyping of rs9939609 polymorphism
Peripheral blood samples were collected in EDTA tubes from all participants, and the total genomic DNA was extracted using salting-out procedure (Citation18). The rs9939609 was genotyped by tetra-primer amplification refractory mutation system polymerase chain reaction method (TP-ARMS-PCR) (Citation19), which applies two pairs of primers to distinguish both alleles of rs9939609 in a single PCR reaction. Primer sequences are presented in () were designed using Primer1 online software (http://primer1.soton.ac.uk/primer1.html). The TP-ARMS-PCR was performed in a total volume of 20 μL, including 0.5 μL (10 pmol) for each outer primer, 1 μL (10 pmol) for inner primers, 10 μL Taq DNA Polymerase 2× Master Mix Red (Amplicon, Denmark), 2 μL of DNA template, and 5 μL distilled water. The thermal cycling was performed on a GeneTouch (BIOER, China) with the following program: the initial denaturation step at 95°C for 2 min, 35 cycles of 95°C for 30 s (denaturation), 59.5°C by 50 s (annealing), and 72°C by 45 s (extension), and followed by a final extension step at 72°C for 5 min. The amplification products were visualized by 2% agarose gel electrophoresis at 100 v for 30 min. Sanger sequencing was performed to verify the genotyping of rs9939609 by TP-ARMS-PCR method.
Table 1. Primer sequences for genotyping FTO rs9939609.
Statistical analysis
The data analyses were carried out using SPSS software version 24 (SPSS Inc., Chicago, USA) and SNPStats online software available from http://bioinfo.iconcologia.net/SNPstats. The chi-squared test was used to calculate allele and genotype frequencies, as well as the Hardy-Weinberg equilibrium. Binary logistic regression analysis was performed to calculate the odds ratio (OR) and its 95% confidence interval (CI) to analyze the multiple risk factors such as age, BMI, and gestational age caused by genotypes of rs9939609, and in all analyses, p-value less than 0.05 is typically considered to be statistically significant. Multiple inheritance models (co-dominant, dominant, recessive, over-dominant, and log-additive) were carried out for statistical analysis. AIC (Akaike Information Criterion) and BIC (Bayesian Information Criterion) values were utilized to determine the best inheritance model and the suitable model being the one with the lowest these values.
Results
The demographic and clinical features of study participants are presented in . There were statistically significant differences in the maternal age, loss of pregnancy, the pre-pregnancy body mass index (BMI), and gestational age between PE patients and controls.
Table 2. Clinical characteristics and demographic variables in the study participants.
The genotypes of the FTO rs9939609 SNP were analyzed using TP-ARMS-PCR and subsequent gel electrophoresis. An electropherogram of different genotypes is shown in . Three genotypes were detected based on their band sizes. The heterozygous (AT) genotype showed three bands: 194 bp, 278 bp, and 429 bp. Homozygous (TT) genotype revealed two bands: 278 bp and 429 bp, as well as homozygous (AA) genotype indicated by two bands: 194 bp and 429 bp. The results obtained from genotyping using TP-ARMS-PCR were in concordance with the sequencing results . In contrast to PE patients, healthy controls had a genotype distribution that was consistent with the Hardy-Weinberg principle. In women with PE, homozygous genotype AA of rs9939609 is statistically significantly less common than in controls: 2.3 versus 15.2%. The distribution of genotypes of the studied SNP is graphically illustrated in . The results showed that FTO rs9939609 was associated with PE in codominant, dominant, and recessive genetic models. The recessive model with the lowest AIC and BIC values was considered the best-fit model (). Binary logistic regression analysis showed that the AA genotype of rs9939609 exhibited a protective role against PE (adjusted OR = 0.046, 95% CI: 0.004-0.469, p = 0.009) after adjusting for age, BMI, and gestational age ().
Figure 1. Electrophoresis pattern for identification of the FTO rs9939609 genotypes. Lanes 1 and 5: AT genotype; lanes 2 and 7: AA genotype; lanes 3 and 6: TT genotype; lane 4: 100 bp DNA ladder; lane 8: NTC (non-template control).
Figure 2. Sequencing result for FTO rs9939609 polymorphism. (a) TT genotype; (b) AT genotype; (c) AA genotype.
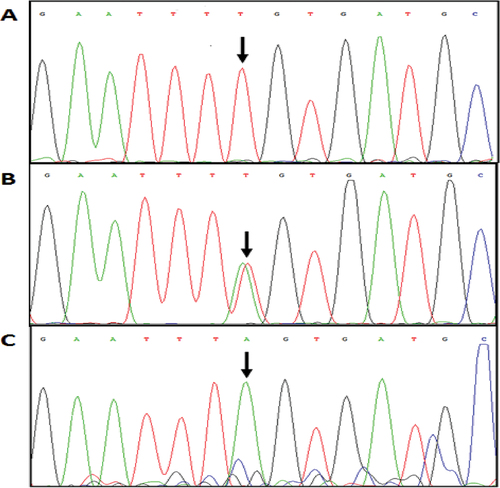
Figure 3. Genotypic distribution of rs9939609 in case and healthy subjects, where the red and green bar represents the cases and controls group respectively. AA and TT are the homozygotic genotypes at some location while AT is heterozygotic.
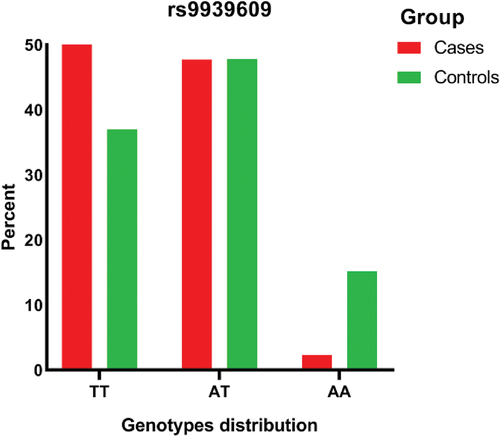
Table 3. Association analysis between FTO SNP (rs9939609) and risk of PE under different genetic models.
Table 4. Binary logistic regression analysis to determine the effect of age, BMI, gestational age, and rs9939609 on the risk of PE.
Discussion
In developed countries, obesity is a serious epidemic that is increasingly spreading to developing nations (Citation20). Obesity prevalence rates among Iranian adults were 22.7% nationwide in 2016.
Furthermore, obesity prevalence rates in Iran were differently significant between male and female (15.3% and 29.8%, respectively) (Citation21). There are millions of pregnant women suffering from PE in the world (Citation22); it has brought an unbearable psychological impact for many families. Obesity is regarded as a significant risk factor for PE, since FTO has been identified as the first obesity-related gene and several studies have shown that FTO plays an important role in obesity. The FTO gene is found on chromosome 16q12.2 in humans. The protein encoded by FTO is an enzyme known as the fat mass and obesity-associated protein (FTO). The connection between FTO gene and PE can provide an important clue about the genetic basis of PE. FTO proteins have been shown to play a role in adipogenesis through the target of the mammalian target protein rapamycin (mTOR) or post-transcriptional control of downstream molecular expression (Citation23). The availability of nutrients and growth hormones triggers the mTOR pathway, which controls protein expression and cell growth. Several obstetric problems can emerge as a result of disrupted mTOR signaling (Citation24). SNP association studies may provide valuable insights into the genetic basis of PE. In the present study, we investigated the possible association between the risk of PE and rs9939609 polymorphism, localized in the intron 1 of the FTO gene in an Iranian pregnant woman. Our results have shown that the FTO rs9939609 polymorphism is associated with PE under the codominant (p = 0.0001), dominant (p = 0.022), and recessive (p < 0.0001) inheritance models. In the most likely model, the FTO rs9939609 AA genotype decreases the risk of PE (p < 0.0001; odds ratio [OR] = 0.13; 95% confidence interval [CI] = (0.04-0.45)) under the recessive inheritance model.
Few studies have investigated the association between rs9939609 and PE, which did not show any significant results (Citation25,Citation26). Samaan et al. performed a meta-analysis including four studies and reported a significant inverse association between rs9939609 and depression (Citation27). On the other hand, depression may increase the risk of PE in women (Citation28,Citation29). Therefore, it is reasonable to hypothesize the genetic factors that show protective effects on depression can be related to a low risk of PE.
Despite the importance of the present findings, this case–control study has several limitations. First, the sample size of Iranian women (128 cases and 184 controls) was relatively small. Second, the means of age and BMI were significantly different between patients and healthy control groups, although the effect of these parameters on the results was adjusted by regression analysis. Third, there is a lack of information about lifestyle factors including physical activity and diet, which could cause a bias between rs9939609 association and BMI or preeclampsia.
Conclusion
Our findings provide for the first time that the FTO rs9939609 polymorphism may be associated with a lower risk of PE under the recessive inheritance pattern in an Iranian population. The possible association between fat-mass-associated SNP rs9939609 and PE should be further investigated with larger sample sizes and with possibilities of stratifying the sample according to the degree of severity and the gestation weeks at the onset of the disease.
Authors’ contributions
GHAT, AF, MFH, AS, and SD designed the study, and carried out the data collection. MSK, JB, MGH, and GHAT were involved in the design of the study, analysis of the data, and critically reviewed the manuscript. This study was conducted at the Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Availability of data and material
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Institutional consent forms were used in this study.
Ethics approval and consent to participate
The current study was approved by the ethics committee of AJA University of Medical Sciences. IR.AJAUMS.REC.1400.312.
Disclosure statement
The authors declare that they have no competing interests.
Additional information
Funding
References
- Ghulmiyyah L, Sibai B. Maternal mortality from preeclampsia/eclampsia. In: Seminars in perinatology . Elsevier. 2012;36(1):56–7.
- Hutcheon JA, Lisonkova S, Joseph K. Epidemiology of pre-eclampsia and the other hypertensive disorders of pregnancy. Best Pract Res Clin Obstetr Gynaecol. 2011;25(4):391–403.
- Duley L. The global impact of pre-eclampsia and eclampsia. In: Seminars in perinatology . Elsevier. 2009;33(3):130–137.
- Nakimuli A, Chazara O, Byamugisha J, et al. Pregnancy, parturition and preeclampsia in women of African ancestry. Am J Clin Exp Obstet Gynecol. 2014;210(6):510–520. e1.
- Vata PK, Chauhan NM, Nallathambi A, et al. Assessment of prevalence of preeclampsia from dilla region of Ethiopia. BMC Res Notes. 2015;8(1):1–6.
- Jeyabalan A. Epidemiology of preeclampsia: impact of obesity. Nutr Rev. 2013;71(suppl_1):S18–25.
- Dekker G, Sibai B. Primary, secondary, and tertiary prevention of pre-eclampsia. The Lancet. 2001;357(9251):209–215.
- Abraham T, Andrea MP. The relationship between obesity and pre-eclampsia: incidental risks and identification of potential biomarkers for pre-eclampsia. Cells. 2022;11(9):1548.
- McPherson R. Genetic contributors to obesity. Can J Cardiol. 2007;23:23A–27A.
- Kim YJ, Lee HS, Kim YK, et al. Association of metabolites with obesity and type 2 diabetes based on FTO genotype. PLoS ONE. 2016;11(6):e0156612.
- Scuteri A, Sanna S, Chen WM, et al. Genome-wide association scan shows genetic variants in the FTO gene are associated with obesity-related traits. PLoS Genet. 2007;3(7):e115.
- Frayling TM, Timpson NJ, Weedon MN, et al. A common variant in the FTO gene is associated with body mass index and predisposes to childhood and adult obesity. Sci. 2007;316(5826):889–894.
- da Fonseca ACP, Abreu GM, Zembrzuski VM, et al. The association of the fat mass and obesity-associated gene (FTO) rs9939609 polymorphism and the severe obesity in a Brazilian population. Diabet, Metabol Syndr Obesity Target Therapy. 2019;12:667.
- Gu HF, Alvarsson A, Brismar K. The common FTO genetic polymorphism rs9939609 is associated with increased BMI in type 1 diabetes but not with diabetic nephropathy. Biomarker Insights BMI. 2010;5:S4599.
- Quan L, Wang H, Tian Y, et al. Association of fat-mass and obesity-associated gene FTO rs9939609 polymorphism with the risk of obesity among children and adolescents: a meta-analysis. Eur Rev Med Pharmacol Sci. 2015;19(4):614–623.
- Lappalainen T, Kolehmainen M, Schwab US, et al. Association of the FTO gene variant (rs9939609) with cardiovascular disease in men with abnormal glucose metabolism–The Finnish diabetes prevention study. Nutrition, Metabolism and Cardiovascular Diseases. 2011;21(9):691–698.
- Pausova Z, Syme C, Abrahamowicz M, et al. A common variant of the FTO gene is associated with not only increased adiposity but also elevated blood pressure in French Canadians. Circulation: Cardiovascular Genetics. 2009;2(3):260–269.
- Miller S, Dykes D, Polesky H. A simple salting out procedure for extracting DNA from human nucleated cells. Nucleic Acids Res. 1988;16(3):1215.
- Ye S, Dhillon S, Ke X, et al. An efficient procedure for genotyping single nucleotide polymorphisms. Nucleic Acids Res. 2001;29(17):e88–88.
- Roberts JM, Bodnar LM, Patrick TE, et al. The role of obesity in preeclampsia. Pregnan Hypertens Int J Women’s Cardiovas Health. 2011;1(1):6–16.
- Djalalinia S, Saeedi Moghaddam S, Sheidaei A, et al. Patterns of obesity and overweight in the Iranian population: findings of STEPs 2016. Front Endocrinol (Lausanne). 2020;11:42.
- Kuklina EV, Ayala C, Callaghan WM. Hypertensive disorders and severe obstetric morbidity in the United States. Obstetr Gynecol. 2009;113(6):1299–1306.
- Lan N, Lu Y, Zhang Y, et al. FTO–a common genetic basis for obesity and cancer. Front Genet. 2020;11:559138.
- Tsai K, Tullis B, Jensen T, et al. Differential expression of mTOR related molecules in the placenta from gestational diabetes mellitus (GDM), intrauterine growth restriction (IUGR) and preeclampsia patients. Reprod Biol. 2021;21(2):100503.
- Klemetti M, Hiltunen LM, Heino S, et al. An obesity-related FTO variant and the risk of preeclampsia in a Finnish study population. J Pregnancy. 2011;2011:2011.
- Andraweera PH, Dekker GA, Leemaqz S, et al. The obesity associated FTO gene variant and the risk of adverse pregnancy outcomes: evidence from the SCOPE study. Obesity. 2016;24(12):2600–2607.
- Samaan Z, Anand S, Zhang X, et al. The protective effect of the obesity-associated rs9939609 a variant in fat mass-and obesity-associated gene on depression. Mol Psychiatry. 2013;18(12):1281–1286.
- Palmsten K, Setoguchi S, Margulis AV, et al. Elevated risk of preeclampsia in pregnant women with depression: depression or antidepressants? Am J Epidemiol. 2012;175(10):988–997.
- Qiu C, Williams MA, Calderon-Margalit R, et al. Preeclampsia risk in relation to maternal mood and anxiety disorders diagnosed before or during early pregnancy. Am J Hypertens. 2009;22(4):397–402.