

ABSTRACT
Introduction
In recent years, the demand for behavioral health services has grown. There is increased need for early access to behavioral health and improved understanding of the relationship between oral health and behavioral health.
Objective
The objective of this article is to provide understanding of how oral health and behavioral health can be integrated in health centers.
Methods
This paper discusses the relationship between oral health and behavioral health, reviews the history of integration, and highlights health centers that have developed systems for dental professionals to engage in two aspects of integration of behavioral and oral health (IBOH) – behavioral health screenings and referral management
Results
Health centers across the country are implementing strategies to increase access to oral health and behavioral health care through integration of the two disciplines.
Conclusion
In health centers, disciplines like primary medical care, dental care, behavioral health, and pharmacy are often co-located. This creates a unique opportunity to provide integrated care, including oral health and behavioral health.
Introduction
Health centers are community-based and patient-directed health care organizations that serve individuals who have limited access to health care.Citation1 Section 330 of the Public Health Service Act defines and authorizes the characteristics of health centers. There are now 1,370 health centers in the United States and its territories. In 2022, the health centers served 30 million people.Citation2 That same year, nearly 80% of health centers had dental programs, which served over 6 million individuals. Most health centers are multiple clinical sites with a variety of health care systems including dental, behavioral health, laboratory, pharmacy, podiatry, and optometry. Many health centers have at least one site where behavioral health and dental are in the same building, creating a scenario for the implementation of integration initiatives between the two disciplines.
Behavioral Health and Oral Health Connection
Behavioral health emerged in recent years as a priority for health care providers and patients. One in 5 adults experience mental illness every year and 1 in 6 people ages 6–17 experience a mental health disorder.Citation3 Depression and anxiety continue to be an issue in the United States.Citation4 Bi-directional relationships between oral health and behavioral health support efforts to integrate these two disciplines. To improve patient experience, oral health professionals need to understand how oral health interrelates with behavioral health. Due to the inherent invasive nature of oral health care, dental visits may be a source of anxiety for many individuals. Dental-related anxiety may reduce the likelihood of accessing oral health care, resulting in less chance for early intervention of oral diseases.
Poor oral health status can negatively affect a person’s quality of life. People with oral health diseases and conditions may experience challenges with employment and school, reduced engagement in social activities, and poor self-esteem. Alternatively, behavioral health conditions can have negative impacts on oral health.Citation5 Individuals with depression may neglect their oral health, leading to increased severity of disease. Individuals experiencing anxiety may hesitate to attend dental appointments and experience bruxism (tooth grinding).Citation6 Many behavioral health medications have oral health side effects.
Many populations are at risk of behavioral health conditions, such as individuals experiencing intimate partner violence (IPV). According to the Health Partners on IPV + Exploitation, 1 in 4 women and 1 in 9 men have experienced IPV.Citation7 Oral health professionals are often the first health care providers to see signs of abuse or trauma. A survey in 2017 found that 50% of dentists did not know where to refer patients who were experiencing IPV.Citation8 Research shows an association between IPV and poor physical and mental health.Citation9
Substance use disorders also have significant impacts on oral health. In 2020, the Department of Health and Human Services’ Substance Abuse and Mental Health Service Administration (SAMHSA) reported that 83.8 million people aged 12 and older used substances in the past year. Substances may include tobacco, illicit drugs, or opioids, all of which have an impact on oral health. In addition, nearly 90% of Americans with substance use disorder received no treatment.Citation10 Tobacco use increases an individual’s likelihood for periodontal disease and oral cancer. Some illicit drugs can cause severe destruction to the mouth through caries, periodontal disease and tooth loss.
History of Integration in Health Centers
Health centers are often innovators in integrated health initiatives because of characteristics that facilitate integration between disciplines. Many health centers have multiple disciplines located under one roof. Health centers may often have care coordinators who support patients in navigating both internal and external referrals to different health care disciplines. Intra-health center referrals are facilitated when the same electronic health record is used across departments. Additionally, many health centers have co-working spaces for team members from different disciplines. For example, nurses may work alongside dental hygienists and physical therapists. This creates increased and improved communication between healthcare providers. Because of these characteristics, the Health Resources and Services Administration (HRSA) has piloted many integration initiatives in health centers.
In the early 2000s, HRSA began initiatives to integrate behavioral health with primary care in health centers with a rationale that behavioral health and physical health were related and that providing behavioral healthcare in the primary care setting could reduce stigma, be cost effective and improve patient outcomes.
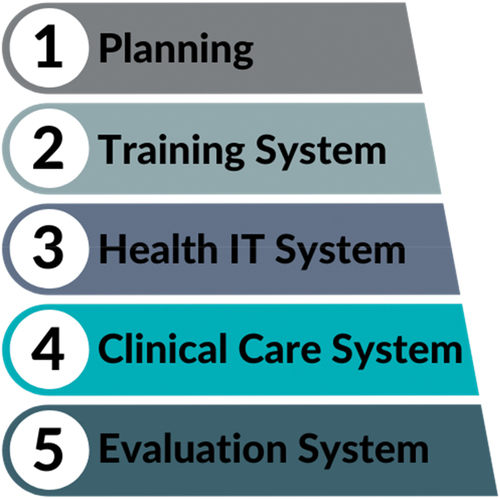
In 2014, HRSA released the Integration of Oral Health and Primary Care Practice (IOHPCP) initiative. In this initiative, which described oral health core clinical competency domains for primary care professionals, the aim was to increase access to oral health care and provide early detection of oral diseases.Citation11 In 2015, HRSA partnered with the National Network for Oral Health Access (NNOHA) to pilot the implementation of the oral health core clinical competency domains. NNOHA released a user’s guide that established a systems-based framework for IOHPCP. The systems are training, health information technology, clinical care, and evaluation.Citation12 The user-guide framework is now utilized by many health centers across the country to integrate primary care and oral health.
Integration of Behavioral Health and Oral Health in Health Centers
One NNOHA priority is to evaluate and scan the healthcare environment for emerging trends and areas of need. Starting in 2018, NNOHA began identifying innovative health centers that were improving access to behavioral health care through the integration of behavioral health and oral health (IBOH). As a result, NNOHA began developing technical assistance resources related to IBOH. The COVID-19 pandemic further revealed the need to increase access to behavioral health care. In 2021, nearly half of Americans reported symptoms of anxiety or depression. In addition, 10% felt that their behavioral health needs were not being met.Citation13
Health centers are annually required to report a set of clinical quality measures to HRSA. In 2003, HRSA released a behavioral health measure. The measure is the percentage of patients (aged 12 and older) who were screened for depression with a standardized tool and, if the screening was positive, had a follow-up plan documented. This measure is integrated, allowing the depression screening to be completed in all types of practice settings, including dental clinics. However, initially very few health centers completed depression screenings in the dental clinic. In 2020, the behavioral health measure dropped by over 7% from 2019. As of 2022, the measure had not rebounded to the pre-pandemic percentage.Citation2 As the demand for behavioral health services continued to increase, health centers began to consider increasing access by having other disciplines conduct behavioral health screenings.
In 2020, NNOHA established the IBOH Learning Collaborative, a project funded through NNOHA’s HRSA National Training and Technical Assistance Partnership. The IBOH Learning Collaborative was created in response to the growing need to increase access to behavioral health care and the need for oral health professionals to understand the relationship between oral health and behavioral health. Historically, behavioral health and oral health integration most commonly included dental providers referring to behavioral health professionals when a patient presented with extreme anxiety about dental care. The aim of the IBOH Learning Collaborative is to support health centers in integrating behavioral health screenings in the dental clinic and increasing bi-directional referrals between behavioral health and dental.
Learning Collaborative Structure
NNOHA piloted the IBOH Learning Collaborative using the previously developed IOHPCP framework used for the integration of oral health core clinical competencies. The pilot cohort (2020) included 12 health centers from all over the United States. The application included information about the health centers’ electronic medical record and dental record systems, readiness to implement IBOH, and a vision statement for IBOH. After the pilot cohort in 2020, NNOHA determined that the IOHPCP framework could be used successfully for IBOH. From 2020 to 2023, NNOHA has worked with 39 health centers through the IBOH Learning Collaborative.
The learning collaborative is virtual and consists of four one-hour webinars over the course of four months. Each webinar covers one of the systems in the IOHPCP framework (). The majority of health centers doing IBOH utilize the Patient Health Questionnaire (PHQ), a validated depressive symptom screening scale.
Figure 1. Integration of oral health and primary care practice framework.
Between each webinar, the health centers engage in group coaching calls with an IBOH faculty member. The coaching calls are grouped by region or state to help facilitate shared understanding of state practice acts, Medicaid reimbursement, and the current climate of behavioral health needs in the area. During these coaching calls, the clinics can share implementation strategies and promising practices. Faculty provide guidance and support. Health centers participating in the learning collaborative must submit monthly data on three measures:
Number and percent of patients who received a behavioral health screening.
Number and percent of patients with a behavioral screening that screened positive.
Number and percent of patients referred to the behavioral health department.
Barriers for Integration
Many dental team members who participated in the IBOH Learning Collaborative reported initial discomfort and lack of confidence in conducting depression screenings. They also shared that they are often unaware of the organization’s policy for patients experiencing a behavioral health crisis. The learning collaborative supported health centers to conduct additional training with dental staff and create dental appointment workflows and scripts that incorporated the screening tool. In addition, health centers developed decision trees to identify when a behavioral health referral is needed based on the screening results. This decision tree also includes references to the health center’s behavioral health crisis policy. Health centers are encouraged to have initial and ongoing trainings with the dental team to increase knowledge and comfort on behavioral health.
Many oral health professionals begin the learning collaborative with concerns about having enough time in the dental appointment to integrate behavioral health screenings. Usually, after multiple test cycles of completing screenings during the appointment, this concern subsides. There are multiple strategies to reduce the amount of time needed to complete the behavioral health screening. For example, the screening tool can be delivered upon patient check-in along with the other intake forms. This reduces the time during the actual appointment to deliver the screening. Instead, the dental provider can focus on reviewing the results and providing education.
Health centers report that health information technology (HIT) is the biggest barrier to full implementation of IBOH. Health center dental and medical departments often have different electronic health record systems that do not communicate. This poses difficulties in documenting behavioral health screenings performed in the dental clinic, viewing screening results and sending and tracking referrals across disciplines. Unified HIT systems expedite the documentation of the screening and the referral process between departments. Also, they assist with follow-up and help the departments know when the patient received behavioral health treatment after a referral. During the learning collaborative, health centers are encouraged to work with their HIT team early in the planning stages to develop work-arounds if the health center does not have an integrated electronic health record (her).
Health Centers in Action: Asian Health Services
One of the earliest national adopters of IBOH was Asian Health Services (AHS) in Oakland, California. Dr. Huong Le, chief dental officer of AHS, initiated an IBOH program after an experience with an adolescent patient. At the end of a patient’s appointment, Dr. Le told the patient they looked forward to seeing them again in six months. The patient responded, “No, you won’t see me in six months because I am going to kill myself when I get home.” The patient and Dr. Le went to a private office. During their discussion, Dr. Le learned that the young patient had been in foster care, going from home to home for years. The patient was tired of living in an unstable arrangement and was unhappy. Dr. Le supported the patient by connecting them to suicide support resources. After the patient left, Dr. Le realized she had received little training as a dentist on behavioral health emergencies. Over the next few days, she considered what else could have been done for this young patient and other patients in similar situations.
Dental patients traditionally see their dentists more times a year than they see their primary care providers. The dental appointments are also longer than medical visits. During these appointments, dental team members often become the patient’s confidant, learning about their personal lives and struggles. Dr. Le worked in collaboration with AHS’ Chief Medical Officer (CMO) and Behavioral Health Manager (BHM) to pilot an IBOH project in 2015.
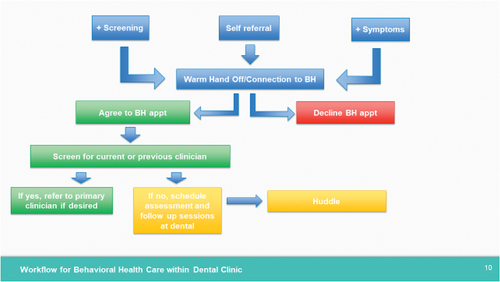
The pilot started out with a target patient population – patients aged 65 years and older. This population accounts for over 30% of dental patients at AHS. Dental staff uses the same form their medical department uses, the PHQ-9. Before the screening program began, the integration champions, CMO, CDO, and BHM, designed a plan for referrals for patients who scored positive on the PHQ-9 (). On the first day of the implementation, a patient wrote on her PHQ-9 form that she was contemplating suicide. This was the first test of the referral process. Fortunately, the AHS team had a formal process in place. The patient was immediately seen by a licensed clinical social worker (LCSW) for her crisis needs.
Figure 2. Workflow for behavioral health care in the dental clinic.
The dental clinic was successful in the pilot in the first six months of integration. In fact, AHS leadership approved the hiring of a LCSW to work in the new dental clinic. This dental clinic was not co-located with a medical clinic on-site; therefore, it was important to have a LCSW embedded in the dental clinic. The first LCSW was hired in December 2017. The AHS team learned that the IBOH program allowed them to capture patients who may have missed their depression screening in the medical clinic. Before the program, annual data of AHS showed only 70% of patients received depression screenings. After the program, over 80% of AHS patients received depression screenings. shows PHQ-9 screening and referral data for the dental program from January 2021 to June 2023.
Figure 3. PHQ-9 screening and referral data from 2021 to 2023.

Although the AHS team continues to see success with the IBOH program, they are still learning to navigate challenges. AHS experienced some staffing shortages requiring the LCSW originally dedicated to the dental clinic to see patients from other departments. This new challenge requires AHS to prioritize referrals based on their screening results.
Dr. Le and the AHS team have received many accolades for their IBOH program, being recognized by HRSA and the Oakland Mayor’s Coalition. They have learned the value of IBOH for their patients and healthcare team. A patient who was taking care of their partner with Parkinson’s Disease was able to see the LCSW in the dental clinic while their partner was being seen for dental services at the same time. An adolescent patient told the AHS counselor how happy they were that they could now receive behavioral health counseling in a dental clinic without their parents’ or friends’ knowledge compared to a counseling center or a medical clinic. The AHS IBOH program has seen reduced stigma around behavioral health and improved patient satisfaction.
Health Centers in Action: Vista Community Clinic
Vista Community Clinic (VCC), a health center in Southern California, aims to provide comprehensive, whole-person care. With an integration mission in mind, the VCC dental department embarked on an integration project with behavioral health.
At the onset of the pandemic, VCC recognized the rising stressors affecting their patients’ health and well-being. At the same time, the California Dental Board distributed information about rising concerns about patients’ behavioral health to all dental licensees. This prompted VCC’s chief dental officer, Dr. Rebecca Cornille, to form a new Integration Committee including the director of dental operations, a dental team champion, the behavioral health operations manager, and the clinical informatics director. This group was tasked with developing a protocol for assessing the behavioral health needs of patients seen in the dental clinic and conducting linkages to care. Coincidentally, NNOHA launched its first IBOH learning collaborative at the same time. Through the guidance of this collaborative, VCC developed an integration strategy with three objectives: (1) identify dental patients in need of behavioral health services, (2) create awareness around behavioral health services available at VCC, and (3) develop a smooth workflow for sharing patients, without upending dental or behavioral health appointment schedules.
The Integration Committee worked through process mapping, training, and pilot testing utilizing small scale tests until a workflow that met program objectives was finalized. The process was aided by the fact that VCC uses electronic dental and medical records that are fully interoperable. Training for the dental team on behavioral health operations was conducted by a medical assistant from the behavioral health department. VCC outlined the team members’ unique responsibilities for each step of the assessment and referral process, addressed how to approach patients about behavioral health screenings, administration and scoring of the behavioral health screening tools, and follow-up procedures for positive results. The Clinical Informatics team provided additional training to assist in navigating new electronic health record modules for accurate data entry.
For consistency, the dental team uses the same two assessment tools used in the primary care clinic, the PHQ-2 and PHQ-9. Sets of both questionnaires have been printed and laminated in the dental clinic. While waiting for their dentist following radiographs, all patients aged 12 and older presenting for initial or recall exams independently complete the PHQ-2. After review with the clinician, patients with a score of 1 or higher then complete the PHQ-9 and results are entered into the patient’s electronic health record.
With the assistance of the behavioral health clinicians, a workflow was developed to provide the most appropriate support based on the patients’ PHQ results. For routine referrals, the behavioral health team will contact the patient to schedule an appointment. If a patient scores positive for suicidal ideations, dental team contacts the behavioral health department for an immediate consult and urgent referral.
At VCC, the implementation of this integration strategy has been a slow, yet strategic journey. About three years ago, the Integration Committee first began meeting bi-weekly. A pilot program was completed at VCC’s largest clinic where dental and behavioral health are co-located. The pandemic brought challenges related to staffing as well as limited access to behavioral health services due to increased demand and the need for more bilingual counselors in the department. As staffing and access improved, implementation was rolled out to additional dental sites.
Critical to the program’s success is its ability to screen dental patients for behavioral health problems combined with the ability of the behavioral health team to provide any needed services in a timely fashion. On a monthly basis, the Integration Committee reviews program outcomes using a custom HIT report that tracks the number of PHQ-2s completed in dental; PHQ-2 screenings that result in PHQ-9 screenings and associated scores; and formal behavioral health referrals issued and completed. To date, 153 PHQ screenings have been completed. Of those 153 screenings, 67 required a PHQ-9. There have been nine formal behavioral health referrals with six patients screened with potential suicidal risk. These results indicate that an integration project between two partner disciplines can successfully identify patients in need of behavioral health services and connect them to much-needed care.
Conclusion
Health centers continue to show innovation to increase access to healthcare. With the clear relationships between behavioral health and oral health, dental professionals should consider integrating behavioral health screenings as a regular part of care. This article reviews strategies to integrate behavioral health screenings in dental clinics at health centers. Health is not simply physical well-being, but also mental and social well-being. Integration of behavioral health and oral health can increase access to behavioral health services, reduce stigma around behavioral health, and improve overall health outcomes.
Disclosure Statement
No potential conflict of interest was reported by the author(s).
Additional information
Notes on contributors
Candace L. H. Owen
Candace L. H. Owen is the Senior Director of Education and Strategic Partnerships for the National Network for Oral Health Access. She is also a registered dental hygienist. Her work focuses on increasing access to health for underserved populations, the oral health workforce, and advancing oral health equity.
Huong Le
Huong Le has been the Chief Dental Officer for Asian Health Services for over 20 years. She oversees several dental sites that serve low-income and uninsured Bay Area residents. She received her Doctorate of Dental Surgery from the University of Texas, Houston. Dr. Le serves on many boards and committees to support communities throughout California and nationwide.
Rebecca A. Cornille
Rebecca A. Cornille is the Chief Dental Officer at Vista Community Clinic. She was named Chief Dental Officer in 2020. Dr. Cornille also has a wide range of teaching, writing, and speaking experience as well as community volunteerism. She received her Doctorate of Dental Surgery from the University of Missouri–Kansas City School of Dentistry.
References
- Health Resources and Services Administration. Bureau of Primary Health Care. What is a health center? https://bphc.hrsa.gov/about-health-centers/what-health-center.
- Health Resources and Services Administration. Health center program uniform data system (UDS). August, 2023. https://data.hrsa.gov/tools/data-reporting/program-data?type=AWARDEE.
- Whitney D, Peterson M. US national and state-level prevalence of mental health disorders and disparities of mental health care use in children. JAMA Pediatr. 2019;173(4):389–5. doi:10.1001/jamapediatrics.2018.5399.
- National Institute of Mental Health. Mental health statistics, major depression. 2020. https://www.nimh.nih.gov/health/statistics/major-depression.
- National Council for Mental Wellbeing. Oral health, mental health and substance use treatment. September, 2021. https://www.thenationalcouncil.org/resources/oral-health-mental-health-substance-use-treatment-toolkit/.
- Kisely S. No mental health without oral health. Can J Psychiatry. 2016;61(5):277–282. doi:10.1177/0706743716632523. Epub 2016 Feb 10. PMID: 27254802; PMCID: PMC4841282.
- Health Partners on IPV+Exploitation. https://healthpartnersipve.org/. Accessed September, 2022.
- Parish C, Pereyra M, Abel, et al. Intimate partner violence screening in the dental setting. JADA. 2018;149(2):112–121. doi:10.1016/j.adaj.2017.09.003.
- Dillon G, Hussain R, Loxton D, Rahman. Mental and physical health and intimate partner violence against women: a review of the literature. Int J Family Med. 2013;2013:313909. doi:10.1155/2013/313909.
- Substance Abuse and Mental Health Service Administration. 2020 National survey on drug use and health, national presentation. July, 2022. https://www.samhsa.gov/data/report/2020-nsduh-national-oas.
- U.S. Department of Health and Human Services. Health resources and services administration. Integration of oral health and Primary care practice. February, 2014. https://drive.google.com/file/d/1f1vREBtbIMKzLDoSYGxnuSvJjm2ZQKau/view.
- National Network for Oral Health Access. A user’s guide for the implementation of interprofessional oral health core clinical competencies. 2015. https://drive.google.com/file/d/17DXVcpniu5793pVPIG0FrKpLI_D2-AUx/view.
- National Institute for Health. Mental health during the COVID-19 pandemic. September, 2023. https://covid19.nih.gov/covid-19-topics/mental-health.