
Abstract
Aging-related diseases are a significant social concern due to rapid aging as life expectancy continues to increase and birth rates decline. This study conducted a meta-analysis to suggest guidelines maximizing effects of forest walking exercises on older adults’ cognitive and physical functions. We collected articles from national and international electronic search engines (RISS, NDSL, KISS, Pubmed, Embase, CINAHL, Riss, and Web of Science) published until February 28, 2021, wherein older adults participated in walking exercises. The overall effect sizes of walking exercise on the Mini-Mental State Examination (MMSE) and performance of activities of daily living (ADL), which are measures of cognitive function, were 0.772 and 0.527, respectively. The overall effect sizes of agility, cardiorespiratory endurance, and upper and lower body strengths, which are measures of physical function, were –0.670, 0.698, 0.685, and 0.433, respectively. The greatest moderation effect was observed for an experimental group size of 20–29 subjects, with complex exercises, exercising for 10 to 19 weeks, exercising three times per week, and for 60 minutes. The results of this study can help minimize errors when designing or assessing research on forest walking exercise programs or selecting appropriate assessment tools or measures.
1. Introduction
Medical advances have increased human life expectancy; however, the birth rate continues to decrease, accelerating global population aging (KOSTAT Citation2021; Jeon et al. 2012). The Organization for Economic Cooperation and Development (OECD) projected South Korea to have the highest percentage of the older adult population in the world by 2045 and the highest old-age dependency ratio among the OECD countries by 2060 (OECD Citation2020; Jeon and Khang 2012). Health spending for older adults aged above 65 years reached 37.6 trillion won in 2021, accounting for over 43% of the total health spending (HIRA and NHIS 2021). This suggests that the social costs generated by the older adult population require particular attention. The incidence of long-term treatment and chronic diseases requiring high costs increases with age. Therefore, along with providing treatment, preventive measures must be taken to reduce older adult patients’ financial burdens. In an aging society, functional independence is crucial in the health management of older adults compared to increasing life expectancy. Regular exercise is vital to prevent physical impairment and functional loss resulting from natural aging (Daley and Spinks Citation2000; Schoenfelder and Rubenstein Citation2004). In a study on older adult patients with chronic stroke, participating in weight shift, balance, and walking exercises for at least one year after the disease onset improved the performance of activities of daily living (ADLs), while regular walking in the older adults prevented chronic diseases and physical impairment (ACSM Citation2006). Another study reported that although individuals’ physical function and health deteriorate with age, regular exercise can help improve muscle strength, muscular endurance, flexibility, and balance reactions in older adults (Mills Citation1994; Kang Citation2007). Son and Lee (Citation2006) demonstrated that walking exercise significantly improves cardiorespiratory function in older adults. NIFoS (Citation2018) reported a study that 2 hours of forest walking improves concentration. Reports consistently show that walking positively affects various indices, including mood state, heart rate, blood pressure, cognitive function, body fat mass, and muscle mass (Shimada et al. Citation2014; Zheng et al. Citation2021; Bishnoi and Hernandez Citation2021). Walking is a free and easily accessible exercise that requires minimal preparation and walking in the forest can produce greater effectiveness through combination with environmental factors. It causes a lower impact on the musculoskeletal system and joints than running; thus, it is recommended for obese individuals or older adults. Walking improves cognitive function by affecting brain activation. In addition, regular physical activity helps maintain and improve brain function in older adults (Bherer et al. Citation2013; Hilman et al. 2008). Hence, it is necessary to synthesize the results of previous papers and examine the effect size through meta-analysis to verify effect of walking exercise affects the improvement of physical function in older adults (Roh and Park Citation2013). A meta-analysis determines the relationship between variables and their level of impact based on the results of studies using various methodologies, thereby deriving an evidence-based conclusion regarding an intervention’s effectiveness (Park and Shin Citation2011). Borenstein et al. (Citation2009) explained that due to their post-hoc nature, meta-analyses can help determine and provide future research directions rather than present a conclusion. To date, meta-analyses have conducted to measure the effect sizes of various kinds of exercise on older adults’ physical function (Gu and Conn Citation2008; Jung Citation2006). However, there is a lack of meta-analyses specifically investigating the effect of walking on older adults’ cognitive and physical functions. While studies have measured muscle strength and flexibility following an exercise intervention in older adults, further research examining upper and lower body strengths is needed since the aging-related loss of lower body strength is a significant risk factor for falls (Schoenfelder and Rubenstein Citation2004). Therefore, it is necessary to examine the effect size of walking on cognitive function and the function such as agility, cardiorespiratory endurance, and upper and lower body strengths in older adults based on multiple studies.
Hence, this study aimed to systematically analyze studies that examine the effect of walking exercise on older adults’ cognitive and physical functions and determine overall effect of walking exercises. This study’s results can help develop guidelines on walking exercises to improve older adults’ cognitive and physical functions.
2. Materials and methods
2.1. Research design
This study was a meta-analysis that examined the effect of national and international walking exercise intervention programs, including forest walking, on older adults’ cognitive and physical functions. The Preferred Reporting Items for Systematic and Meta-Analysis (PRISMA) guideline was followed when conducting this meta-analysis (Page et al. Citation2021).
2.2. Literature selection criteria
Before conducting a literature search, studies satisfying the inclusion and exclusion criteria were selected from national and international data search engines following the PICOS (Participants, Intervention, Comparisons, Outcomes, Study Design) scheme (Choi et al. Citation2020). The participants were older adults. The older adults were selected to be 60 or more years of age. The interventions were programs involving forest walking or indoor walking. The comparator was a group that did not participate in a walking exercise program. The outcome was the effect of walking exercises on cognitive and physical functions, and only the studies that provided numerical data were included. Finally, the study designs were randomized controlled trials (RCTs) and non-RCTs (NRCTs). Domestic and foreign studies published in Korean or English were included to investigate the effect of walking exercise on disease prevention in older adults considering the global population aging. Case studies, meta-analyses, studies without original text, and single-group studies were excluded. Once the inclusion criteria were created, studies were searched and selected following the PRISMA Flow Diagram (Page et al. Citation2021).
2.3. Data search and selection process
Studies wherein a walking program was conducted among older adult subjects were searched without restricting the publication year. National and international studies published until February 28, 2021, the data of search date, were searched using Korean search engines, including RISS, NDSL, and KISS, and global search engines, including Pubmed, Embase, CINAHL, Riss, and Web of Science. The search was performed using the “AND” and “OR” operators. The search words used in the national and international search engines were as follows: (“walking” OR “forest walking” OR “walking in urban parks” OR “pedometer” OR “accelerometor” OR “accelerometer” OR “green space walking” OR “walking exercise in forest” OR “forest physical activity” OR “physical activity in forest” OR “forest exercise” OR “forest activity” OR “shinrin-yoku” OR “forest basking” OR “forest bathing” OR “forest therapy”) AND Mini-Mental State Examination (“MMSE”). Additionally, studies were added by manually searching the references of the searched studies. Duplicate articles were removed, and RefWorks was used for article management. The initial search was independently performed by two researchers. After reviewing the titles and abstracts of the studies, they selected studies following the inclusion and exclusion criteria. In case disagreements, they consulted a third researcher to conclude. The results of the final selected studies were extracted and analyzed.
2.4. Assessment of bias
An assessment of bias was conducted on the final selected studies. For, RCTs the Cochrane’s Risk-of-bias tool (RoB2) was used (sterne et sl. 2019). For NRCTs, the Risk of Bias Assessment tool for Non-randomized Study (RoBANS) was used (Kim et al. Citation2011). Two researchers collaboratively reviewed the assessment results for each domain.
2.5. Data management and analysis
A data format was mutually determined by the researchers. The format included study information (authors, publication year, and study country), subjects (age and sex), intervention method (number of intervention groups, exercise type, duration, frequency, time, and intensity), and outcomes (cognitive and physical functions).
A meta-analysis package for the R program was used to conduct a meta-analysis. Since studies vary in subjects, intervention methods, and research environments, a random effect model was used to calculate the mean effect size. The effect size was calculated for cognitive function (MMSE and ADL) and physical function (agility, cardiorespiratory endurance, and upper and lower body strengths). MMSE scores are a scale for assessing cognitive function. This consist of a total of 30 questions in 23 items. total score is 30 points. 9 out of 30 points or less are suspected of severe dementia, 10 ∼ 14 points are suspected of moderate dementia, 15 ∼ 19 points are suspected of mild dementia, 20 ∼ 24 points are borderline area, and 25 points or more mean normal state. ADL performance is an assessment of daily activities, which is performed to determine the ability to take care of oneself and maintain independence in basic daily life and is an important basis for assessing early-stage illness. Agility was measured by timed up and go (TUG); this is an indicator that measures of how quickly it takes person to stand up from a 43 cm chair, go and return to the target 2.4 m, and sit down on the chair. It is a fall risk assessment scale that determines that the longer it takes to perform, the higher the risk of decline in physical function and dementia. Cardiorespiratory endurance was measured by 6-minute walking test (6MWT); this is an indicator that measures of how far person walked a 45.7m rectangular course in 6 minutes. Upper body strength is a 30 lb dumbbell repetitive lift for 30 seconds. Lower body strength was measured by 30s sit to stand test; this is an indicator that measures the number of times person sitting down and standing up from a 43 cm chair for 30 seconds. Normal standards are different for each gender and age, and healthy middle-aged people can perform it more than 20 times.
The overall effect size was determined based on the obtained effect sizes. The outcome variable was the difference between the post-test and pre-test means. The effect size was converted to Hedge’s g, which reflects a corrected standardized mean difference to account for the varying sample size across the studies and confidence interval was 95% (Borenstein et al. Citation2009). A forest plot was used to graphically present each study’s effect size, statistical significance, and weightage, overall (mean) effect size, and statistical significance of the combined studies (Hwang Citation2020). Cohen (Citation1988) interpreted that an effect size is small if it is less than 0.10 ∼ 0.30, medium if it is less than 0.40 to 0.70, and large if it is 0.80 or higher. Heterogeneity was examined by creating a forest plot of average effect sizes and analyzed using the Q value representing the total variance and the I2 value representing the true variance. An I2 value ≤25% indicates low heterogeneity, 25-50% indicates moderate heterogeneity, and ≥75% indicates high heterogeneity (Higgins and Green Citation2016).
A meta-ANOVA was performed using frequency variables from walking programs to determine heterogeneity. To assess publication bias, the symmetry of a funnel plot was examined and visualized, followed by a test to assess the results’ consistency (Borenstein et al. Citation2009).
3. Results
3.1. Article selection
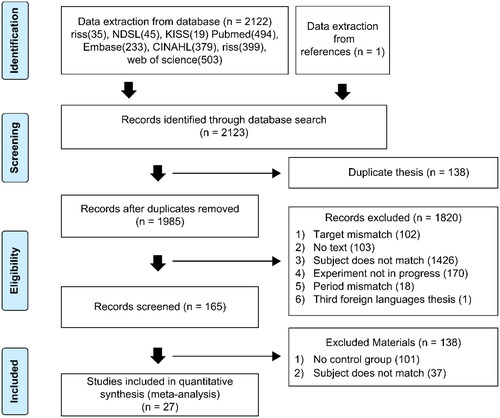
Including one from a reference review, a total of 2,123 studies were reviewed, selected, and organized using an article management program (ProQuest RefWorks). Among these, 138 duplicate studies, 102 studies with unmatched targets, 103 studies without original text, 1,463 studies with unmatched subjects, 170 studies without an experiment, 18 studies with unmatched study periods, 1 study written in a non-target language, and 101 studies without a comparator group were excluded. Two researchers independently collected and selected the studies. During disagreements, the researchers read the entire paper and made the final decision after reviewing the inclusion and exclusion criteria. If a study was excluded, they recorded the reason for the exclusion. A total of 27 papers eligible for a meta-analysis were eventually selected ().
Figure 1. PRISMA flow chart
3.2. Characteristics of selected articles
summarizes the characteristics of the 27 studies included in the meta-analysis, including authors, publication year, study country, sample size, study design, participants, intervention type, duration, frequency, time, intensity of exercise, and measurement tool. Publication years were evenly distributed from 2008 to 2021. One study (3.7%) was conducted before 2010, and 26 (96.3%) from 2010 to 2021. Twenty-one studies (77.8%) were published in South Korea, two (7.4%) in the United States, one (3.7%) in Finland, one (3.7%) in Germany, one (3.7%) in Brazil, and one (3.7%) in France. Fourteen studies (51.9%) were RCTs, and 13 (48.1%) were NRCTs. Fourteen studies (51.9%) had female subjects only, and 13 (48.1%) had mixed or unspecified sex. The subjects’ ages were evenly distributed from 60s to 70s years. Nineteen studies (70.4%) included healthy older adult subjects, and eight (29.6%) included older adult patients with cognitive decline, dementia, or Alzheimer’s disease. The intervention type was a complex exercise in 20 studies (74.1%) and walking exercise in 7 (25.9%). Complex exercise refers to exercises that combine aerobic and strength training. The intervention period ranged from 8 to 92 weeks. An intervention period of 12 weeks was the most common, used in 14 studies (51.9%). The weekly exercise frequency was twice in six studies (22.2%), three times in sixteen studies (59.3%), four times in two studies (7.4%), and five times or more in three studies (11.1%). The exercise time was 60 minutes in most studies (n = 16, 59.3%). Exercise intensity was presented in the heart rate reserve (HRR) and rating of perceived exertion (RPE). Nine studies (33.3%) did not describe how exercise intensity was determined ().
Table 1. Characteristics of selected articles
3.3. Quality assessment
A risk of bias assessment was performed to assess the methodological quality of the 27 selected studies to ensure the risk of biases and misinterpretations that stem from a study design or occur during a research process is minimized. The 14 RCTs assessed with RoB2 showed a low risk of bias (). The 13 NRCTs assessed with RoBANS also showed a low risk of bias ().
Table 2. Characteristics of selected articles
Table 3. Risk of bias for non-randomized controlled trial studies (RoBANS)
3.4. Effect size of walking exercise
Hedge’s g, or a corrected standardized mean difference, was calculated using the difference between the pre-test and post-test means, the standard deviations of the difference, and the sample size of the experimental and control groups from the 27 selected studies, which was visualized using a Forest plot to see the overall trend (see ).
Figure 2. Effect size with MMSE scores
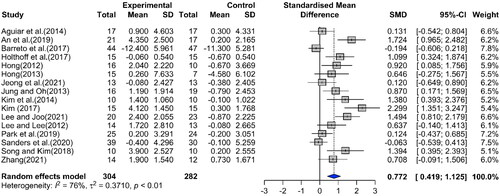
Figure 3. Effect size scores on activities of daily living
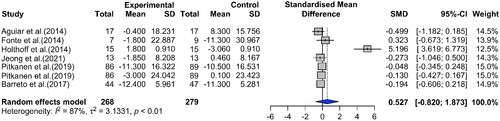
Figure 4. Effect size on agility
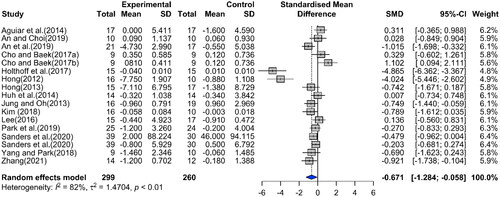
Figure 5. Effect size on cardiorespiratory endurance
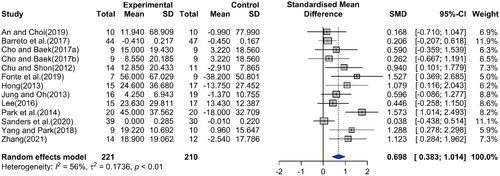
Figure 6. Effect size on upper body strength
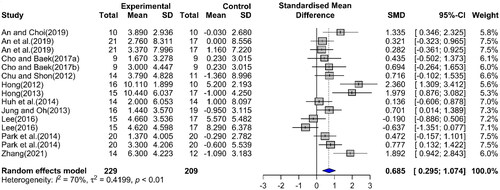
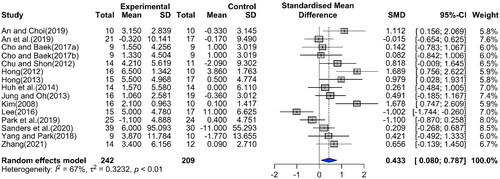
Figure 7. Effect size on lower body strength
1) Effect size of walking exercise on cognitive function
The effect of walking exercise on the MMSE scores and ADL performance, examined as measures of cognitive function, was examined.
Sixteen studies were included in the MMSE calculation of the effect sizes of walking. The overall effect size on MMSE scores was medium at 0.772 (95% Confidence Interval (CI): 0.419 ∼ 1.125) and was statistically significant as it did not include 0. This indicates that walking exercise substantially affects MMSE scores. The I2 value, which represents the heterogeneity in the overall effect size of MMSE scores, was 76%, indicating high heterogeneity (Q = 62.50, p <. 0001) (see ). Seven studies were included in calculating the effect size of walking on the ADL performance. The overall effect size was 0.527 (95% CI: –0.820 ∼ 1.873) and was not statistically significant. The I2 value was 87%, indicating high heterogeneity (Q = 45.73, p <. 0001) (see ).
2) Effect size of walking exercise on physical function
In 17 studies that examined agility, the overall effect size of walking exercise was –0.671 (95% CI: –1.284∼0.058), indicating that walking significantly affects agility. The I2 value was 82%, indicating high heterogeneity (Q = 88.87, p <. 0001; see ). The overall effect size of walking exercise on cardiorespiratory endurance examined in 13 studies was 0.698 (95% CI: 0.383 ∼ 1.041), indicating that walking significantly affects cardiorespiratory endurance. The I2 value of these studies was 56% (Q = 27.03, p = 0.0076; see ). The overall effect size of walking exercise on upper body strength examined in 15 studies was 0.685 (95% CI: 0.295 ∼ 1.074), indicating that walking significantly affects upper body strength. The I2 value of these studies was 70% (Q = 46.24, p <. 0001; see ). The overall effect size of walking exercise on lower body strength examined in 15 studies was 0.433 (95% CI: 0.080 ∼ 0.787), indicating that walking significantly affects lower body strength. The I2 value of these studies was 67% (Q = 41.91, p <. 0001; see ).
3.5. Heterogeneity test of effect size: moderation effect analysis
The MMSE scores (I2=76%, Q = 62.50, p <. 0001) and agility scores (I2=82%, Q = 88.87, p <. 0001) showed statistically significant effect sizes and high heterogeneity in the previous analysis. When effect sizes are heterogeneous across studies, a moderation effect analysis can identify the sources of heterogeneity (Page et al. Citation2021). Thus, a meta-ANOVA was conducted with sample size (experimental group), the type, duration, frequency, and time of exercise as the moderators (). During the analysis of the moderation effect on MMSE scores, walking had the highest effect size on MMSE scores when the sample size was 20-29, and a significant difference was found between the experimental group sizes (Qb=20.28, p =. 0001). For exercise types, walking had a higher effect size than complex exercise, with a significant difference between the experimental group sizes (Qb = 13.50, p =. 0002). An exercise duration of 10 ∼ 19 days had the largest effect size, with a significant difference between the experimental group sizes (Qb = 25.56, p =. 0001). An exercise time of 60 minutes had a largest effect size, with a significant difference between the experimental group sizes (Qb = 32.61, p =. 0001). Exercise frequency did not affect the mean effect size (Qb = 8.39, p =. 0387).
Table 4. Moderation effects on MMSE scores
During a moderation effect analysis on agility, the size of the experimental group (Qb = 3.54, p =. 3514), exercise type (Qb = 2.91, p =. 0879), the exercise duration (Qb = 1.46, p =. 4811), and exercise frequency (Qb = 9.50, p =. 0234) did not affect the mean effect size (). The largest effect size was observed for an exercise time of 60 minutes, with a significant difference between the experimental group sizes (Qb = 37.18, p =. 0001).
Table 5. Moderation effect on agility
3.6. Publication Bias
A funnel plot analysis, generally recommended for visually analyzing plot symmetry, was used to assess publication bias, and the analysis results were validated using Egger’s regression test (Borenstein et al. Citation2009). A symmetrical funnel plot with studies evenly distributed throughout the funnel plot was observed for MMSE, agility, cardiorespiratory endurance, and upper and lower body strengths. Egger’s regression test was performed to confirm the result’s statistical significance, which showed a bias of 5.87 (t = 4.67, df = 14, p =. 0514) and –3.7001 (t=–2.05, df = 15, p =. 0584) for MMSE and agility, respectively; no significant asymmetry was observed, indicating no publication bias. Regarding cardiorespiratory endurance, upper body strength, and lower body strength, a bias of 3.0175 (t = 2.83, df = 11, p =. 0164), 6.3397 (t = 3.25, df = 13, p =. 0063), and 3.9287 (t = 2.22, df = 13, p =. 0446) was observed, respectively; publication bias existed for these variables. Publication bias was not assessed for ADL using the funnel plot and Egger’s regression analysis since there were fewer than 10 studies.
Discussion
Cognitive effects of walking fognitive effects of walkingalking with other exercise or
The overall effect size of walking exercise on MMSE scores as a measure of cognitive function in older adults was moderate at 0.772 (95% CI: 0.419 ∼ 1.125), indicating that these can improve cognitive function in older adults. Regular physical activity increases neuroplasticity in the brain, thereby positively affecting cognitive function (Voelcker‐Rehage et al. Citation2010, Hillman et al. Citation2008). This supports the results of this study wherein walking improved cognitive function (Colombe and Kramer Citation2003). A moderation effect analysis performed due to high heterogeneity showed significant differences in the effect of walking on MMSE scores according to the experimental group size and the type, duration, and time of exercise. Therefore, it is considered that a group of 20 ∼ 29 subjects and a combined exercise program including forest walking exercise are suitable for improving the cognitive function of the elderly (Kim and Yoo Citation2013, Spina et al. Citation1993). Walking exercise had the highest effect on MMSE scores for an exercise duration of 10 ∼ 19 weeks, an exercise frequency of three times per week, and an exercise time of 60 minutes. Walking can be recommended to anyone since it is an easily accessible aerobic exercise that can be performed anywhere at any time and does not require special skills. Han et al. (Citation2007) reported that an exercise program for older adults is the most effective if conducted for 8 to 12 weeks, consistent with our findings. The effect size of walking exercise on ADL scores as a measure of cognitive function was moderate at 0.527 (95% CI: -0.820 ∼ 1.873) and not statistically significant. Chu et al. (Citation2007) conducting a cognitive behavioral program among older adults with cognitive decline twice a week for six weeks (a total of 12 50-minute sessions) reported significant improvements in cognitive function by the program end but no significant difference in ADL performance, consistent with our results.
Second, the overall effect size of walking exercise on older adults’ agility was -0.671 (95% CI: -1.284∼-0.058) and was statistically significant. The I2 value for studies on agility was 82%, indicating high heterogeneity (Q = 88.87, p <. 0001). A moderation effects analysis showed that the experimental group size and the type, duration, and frequency of exercise did not affect the mean effect size; however, the exercise time was the only variable that had an effect. Since agility is highly associated with walking speed, balance, and ADL measures, our result demonstrates that regular exercise can promote normal walking and improve body stability (Rikli and Jones Citation2013). The effect size of walking exercise on cardiorespiratory endurance as a measure of physical function was 0.698 (95% CI: 0.383 ∼ 1.041) and was statistically significant. Cardiorespiratory endurance is crucial to older adults’ ADL performance, which can be improved by participating in an exercise program (Kim et al. Citation2015); our results thus confirm this finding by showing that participating in a walking program improves one’s ADL performance by improving cardiorespiratory function. The overall effect size of walking exercise on upper body strength was 0.685 (95% CI: 0.295 ∼ 1.074) and was statistically significant, and lower body strength was 0.433 (95% CI: 0.080 ∼ 0.787) and was statistically significant. Aging-related muscle mass and strength loss lead to muscle functional deterioration, reducing physical activity. Regular exercise delays functional muscle deterioration or improves muscle function and reduces the risk of falls, leading to a safer life (Kim Citation2013, Seo et al. Citation2014, Haskell and Phillips Citation1995). Our results show that improving muscle strength and muscular endurance positively affects daily life and that exercise promotes healthy living in older adults.
Our study is meaningful as we determined the effect sizes of walking exercise on older adults’ cognitive functions, agility, cardiorespiratory endurance, upper body strength, and lower body strength and the overall effect of all studies combined. Additionally, we analyzed the effect size of walking exercise for varying sample sizes, study designs, sexes, ages, exercise types, durations, frequencies, and time, and obtained essential data for developing a forest walking program for older adults. The effects of walking may be maximized by using the appropriate exercise duration and intensity for each individual to improve their cardiorespiratory function and adding flexibility exercises, such as stretching. We combined and quantitatively analyzed previous findings to produce more generalizable results, thereby reducing the need for repeated research and providing data for better decisions when developing a forest walking program. We also explored various study designs used to assess the effectiveness of walking exercise programs through a literature review. Our findings can help minimize errors when designing or assessing research on walking exercise programs and forest walking program or selecting appropriate assessment tools or measures.
Conclusion
This study performed a meta-analysis to assess the effects of walking exercise programs for older adults based on the RCTs and NRCTs results assessing cognitive and physical functions. Our analysis demonstrates that walking exercise programs can improve older adults’ cognitive and physical functions, which is a significant finding considering the ongoing global population aging. This result indicates that walking exercise improves overall cognitive function and physical fitness and creates positive changes of body composition in older adults, which can further improve their ability to perform daily activities and, consequently, improve their quality of life and reduce the medical costs of aging societies.
Declaration of interest
The authors report there are no competing interests to declare.
Additional information
Funding
References
*References marked with an asterisk indicate studies included in the meta-analysis.
- *Aguiar P, Monteiro L, Feres A, Gomes I, Melo A. 2014. Rivastigmine transdermal patch and physical exercises for Alzheimer's disease: a randomized clinical trial. Curr Alzheimer Res. 11(6):532–537. doi: 10.2174/1567205011666140618102224.
- *Ahn NY, Ju YS, Lee GH, Kim KJ. 2019. Changes of Body Composition, Physical Fitness, and Cognitive Function after 16-week Regular Exercise Training in Elder Women with Dementia. JCD. 21(1):110–117. doi: 10.47684/jcd.2019.03.21.1.110.
- *An SH, Choi YC. 2019. Effects of Combined Exercise on Functional Fitness, Cognitive Function and Blood Lipids in Elderly Women. KSSS. 28(2):967–975.
- *Cho YM, Baek YH. 2017. Effects of Exercise Training Types on Body Composition and Senior fitness test, Age related hormone in Elderly Females. KSSS. 26(4): 943–953.
- *Chu YK, Shon JH. 2012. Effect of Combined Exercise Program for 16 Weeks on Health-Related Physical Fitness and Depression in Elderly Women. JCD. 14(3):105–114.
- *de Souto Barreto P, Cesari M, Denormandie P, Armaingaud D, Vellas B, Rolland Y. 2017. Exercise or Social Intervention for Nursing Home Residents with Dementia: A Pilot Randomized, Controlled Trial. J Am Geriatr Soc. 65(9):E123–E129. doi: 10.1111/jgs.14947.
- *Fonte C, Smania N, Pedrinolla A, Munari D, Gandolfi M, Picelli A, Venturelli M. 2019. Comparison between physical and cognitive treatment in patients with MIC and Alzheimer’s disease. Aging (Albany NY). 11(10):3138.
- *Holthoff VA, Marschner K, Scharf M, Steding J, Meyer S, Koch R, Donix M. 2015. Effects of physical activity training in patients with Alzheimer’s dementia: results of a pilot RCT study. PLoS one. 10(4):e0121478. doi: 10.1371/journal.pone.0121478.
- *Hong SY. 2012. Effects of an 8-week Individualized Exercise Program on Parameters of Functional Capacity, Mobility and Cognitive Function in Elderly Persons with Dementia. J KSLES. 19(3):352–361.
- *Hong, S.Y. 2013. Effects of Multi-component Exercise Intervention on the Physical and Cognitive Function of Demented Older Patients: 24-week Pilot Study. KGS. 33(2):257–273.
- *Huh YG, Jung WS, Lee MG. 2014. Effects of a 13-week outdoor group walking exercise on depression and its’ related variables in elderly women. KSSS. 23(2):1351–1364.
- *Jeong MK, Park KW, Ryu JK, Kim GM, Jung HH, Park H. 2021. Multi-component intervention program on habitual physical activity parameters and cognitive function in patients with mild cognitive impairment: a randomized controlled trial. IJERPH. 18(12):6240. doi: 10.3390/ijerph18126240.
- *Jung YJ, Oh DJ. 2013. The Effects of 12 weeks-home Support Exercise Program on Elderly dementia Female Senior Fitness, Cognitive function. KSSS. 22(4): 1015–1024.
- *Kim BY. 2008. The Effects of Walking Exercise during 12 Weeks on the Cardiorespiratory Function and Physical Fitness in Elderly Women. KSSLS. 33:851–862. doi: 10.51979/KSSLS.2008.08.33.851.
- *Kim NI. 2017. The Effects of Walking Meditation Program on Autonomous Nervous System and Risk Factors of Dementia in Elderly Women. KJGD. 25(1):15–23.
- *Kim TS, Yoon JH, Lee BK. 2014. Neuro-Cognitive Influence of Walking Exercise through the Regulation of Neurotrophic Factors in Aging Women. KSSLS. 55:559–571. doi: 10.51979/KSSLS.2014.02.55.559.
- *Lee CM, Lee NH. 2012. Effects of Combined Exercise on Neurothophic Factors and Cognitive Function in Elderly Women. KPEAGW. 26(1):173–189.
- *Lee CS, Joo DJ. 2021. The Effects of Good Posture Walking on Preventing Fall and Improving Cognitive Ability of Older Adults. JHSS21. 12(3):2379–2392.
- *Lee SC. 2016. The Effects of a Regular Walking Program on Body Composition, Functional Fitness, and Anxiety and Depression in Elderly Women. KSIM. 4(2):67–76.
- *Park HT, Park JH, Na HR, Hiroyuki S, Kim GM, Jung MK, Park KW. 2019. Combined Intervention of Physical Activity, Aerobic Exercise, and Cognitive Exercise Intervention to Prevent Cognitive Decline for Patients with Mild Cognitive Impairment: A Randomized Controlled Clinical Study. J Clin Med. 8(7):940. doi: 10.3390/jcm8070940.
- *Park HW, Lee WB, Han TY, Kwon HJ, Hur S. 2014. Effect of community health center exercise class program on body composition, physical fitness and blood components in elderly women. KSSS. 23(4):891–900.
- *Pitkänen A, Alanen HM, Kampman O, Suontaka-Jamalainen K, Leinonen E. 2019. Implementing physical exercise and music interventions for patients suffering from dementia on an acute psychogeriatric inpatient ward. Nord J Psychiatry. 73(7):401–408. doi: 10.1080/08039488.2019.1645205.
- *Sanders LMJ, Hortobágyi T, Karssemeijer EGA, Van der Zee EA, Scherder EJA, Van Heuvelen MJG. 2020. Effects of low-and high-intensity physical exercise on physical and cognitive function in older persons with dementia: a randomized controlled trial. Alzheimer's Res Ther. 12:1–15.
- *Song CH, Kim KH. 2018. The Effect of Health Promotion Exercise on Alzheimer's Dementia-related Factors and Cognitive Function in Elderly Women. KSSS. 27(3):1219–1228.
- *Yang DJ, Park HS. 2018. Effect of complex exercise program using outdoor exercise equipment on health-related physical strength, blood glucose and peripheral arteries of elderly women. KSSS. 27(4):979–991.
- *Zhang SA. 2021. Effects of Walking and Band Exercising on Cognitive Function, Dementia-related Factor and Senior Fitness of the Elderly Women with Mild Cognitive Impairment. KWS. 16(2):291–298.
- ACSM (American College of Sports Medicine). 2006. ACSM's guidelines for exercise testing and prescription, 7th edition. Philadelphia: Lippincott Williams & Wilkins.
- Bherer L, Erickson KI, Liu-Ambrose T. 2013. Physical exercise and brain functions in older adults. J Aging Res. 2013. doi: 10.1155/2013/197326.
- Bishnoi A, Hernandez ME. 2021. Dual task walking costs in older adults with mild cognitive impairment: a systematic review and meta-analysis. Aging Ment Health. 25(9):1618–1629. doi: 10.1080/13607863.2020.1802576.
- Borenstein M, Hedges LV, Higgins JPT, Rothstein HR. 2009. Introduction to meta-anaylsis. West Sussex: John Wiley & Sons Ltd.
- Choi EH, Kim MJ, Lee EN. 2020. [A Meta-Analysis on the Effects of Mind-Body Therapy on Patients with Irritable Bowel Syndrome]. J Korean Acad Nurs. 50(3):385–400. doi: 10.4040/jkan.19224.
- Chu SK, Yoo JH, Lee CY. 2007. The Effects of a Cognitive Behavior Program on Cognition, Depression, and Activities of Daily Living in Elderly with Cognitive Impairment. J Korean Acad Nurs. 7(7): 1049–1060. doi: 10.4040/jkan.2007.37.7.1049.
- Cohen J. 1988. Statistical Power Analysis for the Behavioral Science (2nd ed). New Jersey: Lawrence Erlbaum Associates.
- Colombe S, Kramer AG. 2003. Fitness effects on the cognitive function of older adults: A meta-analytic study. Psychol Sci. 14(2): 125–130. doi: 10.1111/1467-9280.t01-1-01430.
- Daley MJ, Spinks WL. 2000. Exercise, mobility and aging. Sports Med. 29(1):1–12. doi: 10.2165/00007256-200029010-00001.
- Gu MO, Conn VS. 2008. Meta-analysis of the effects of exercise interventions on functional status in older adults. Res Nurs Health. 31(6):594–603. doi: 10.1002/nur.20290.
- Han YS, Choi JH, Lee PY. 2007. Development and effect of the customized health gymnastics program for the frail old. Korean J Phys Educ. 46(5): 595–606.
- Haskell WL, Phillips WT. 1995. Exercise Training, Fitness, Health, and Longevity. Perspectives in exercise science and sports medicine: Exercise in older adults. pp 11-52.
- Higgins JPT, Green S. 2016. Cochrane handbook for systematic reviews of interventions version 5.1.0 [Online]. London: The Cochrane Collaboration. Available from: http://handbook.cochrane.org.
- Hillman CH, Erickson KI, Kramer AF. 2008. Be smart, exercise your heart: exercise effects on brain and cognition. Nat Rev Neurosci. 9(1): 58–65. doi: 10.1038/nrn2298.
- HIRA (Health Insurance Review and Assessment Service), NHIS (National Health Insurance Service). 2021. 2020 National health insurance statistical yearbook. Available from: https://www.hira.or.kr.
- Hwang SD. 2020. Meta-analysis using R. Seoul: Hakjisa.
- Jeon HS, Kahng SK. 2012. Age Differences in the Predictors of Medical Service Use between Young-Old and Old-Old: Implications for Medical Service in Aging Society. Health Soc Welfare Rev. 32(1):28–57.
- Jung YS. 2006. A meta analysis of the effects of exercise programs in older adults. Unpublished doctoral dissertation. Seoul: Ewha Womans University.
- Kang JS. 2007. Effects of a regular walking exercise on functional improvement in the Korean elderly. Unpublished master's thesis. Seoul: Yonsei University.
- Kim DW, Ahn JD, Shin SK. 2015. The Effects of Flexibility and Resistance Exercise for 16weeks on Growth Factor Hormone, Senior Fitness and Life Quality (SF-36) in Elderly Women. KJGD. 23(4): 261–272.
- Kim NJ. 2013. Effects of Elastic Band and Pilates Exercise on Atherosclerosis Indices and Inflammation Related Markers in Elderly Obese Women. KPEAGW. 27(1): 79–92.
- Kim SW, Yoo HS. 2013. Effects of chronic aerobic exercise on cognitive function of older adults an examination of P300-. KSSS. 22(4): 411–428.
- Kim SY, Park JE, Seo HJ, Seo HS, Son HJ, Shin CM, Lee YJ, Jang BH. 2011. NECA's guidance for undertaking systematic reviews and meta-analyses for intervention. National Evidence-based healthcare Collaborating Agency Team of New Health Technology Assessment.
- KOSTAT (Statistics Korea). 2021. 2020 Future Population Projections. Available from: https://kostat.go.kr.
- Mills EM. 1994. The effect of low-intensity aerobic exercise on muscle strength, flexibility, and balance among sedentary elderly person. Nurs Res. 43(4):207–211.
- NIFoS (National Institute of Forest Science). 2018. NIFoSNews. Available from: https://know.nifos.go.kr/webzine.
- OECD (Organization for Economic Cooperation and Development). 2020. Health Statistics. Available from: https://www.oecd.org.
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, et al. 2021. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg, 88:105906. doi: 10.1016/j.ijsu.2021.105906.
- Park EY, Shin IS. 2011. The effects of transitional education programs on adaptive behavior in students with developmental disabilities: A meta analysis. Disabil Employ. 21:59–78.
- Rikli RE, Jones CJ. 2013. Senior fitness test manual. Champaign (IL): Human Kinetics.
- Roh KH, Park HA. 2013. A Meta-analysis of the Effect of Walking Exercise on Lower Limb Muscle Endurance, Whole Body Endurance and Upper Body Flexibility in Elders. J Koeran Acad Nurs. 43(4):536–546. doi: 10.4040/jkan.2013.43.4.536.
- Schoenfelder DP, Rubenstein LM. 2004. An exercise program to improve fall-related outcomes in elderly nursing home residents. Appl Nurs Res. 17(1):21–31. doi: 10.1016/j.apnr.2003.10.008.
- Seo DI, Han YR, Kim IH, Oh HO, Park ST, So WY. 2014. The Effect of 8 Weeks of Pilates on Physical Fitness and Fall Efficacy in Elderly Women. KSW. 9(4): 201–208.
- Shimada H, Makizako H, Tsutsumimoto K, Uemura K, Anan Y, Suzuki T. 2014. Cognitive function and gait speed under normal and dual-task walking among older adults with mild cognitive impairment. BMC Neurol. 14(1):1–8.
- Son JU, Lee JH. 2006. The effect of the walking exercise on physiological index, physical fitness, self esteem, depression and life satisfaction in the institutionalized elderly women. J Korean Acad Community Health Nurs. 17, 5–16.
- Spina RJ, Ogawa T, Miler TR, Kohrt WM, Ehsani AA. 1993. Effect of exercise training on left ventricular performance in older women free of cardiopulmonary disease. Am J Cardiol. 71(1): 99–104. doi: 10.1016/0002-9149(93)90718-r.
- Sterne JAC. et al. 2019 RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 366. doi: 10.1136/bmj.l4898.
- Voelcker‐Rehage C, Godde B, Staudinger UM. 2010. Physical and motor fitness are both related to cognition in old age. Eur J Neurosci. 31(1): 167–176. doi: 10.1111/j.1460-9568.2009.07014.x.
- Zheng Y, Meng Z, Zhi X, Liang Z. 2021. Dual-task training to improve cognitive impairment and walking function in Parkinson's disease patients: A brief review. Sports Med Health Sci. 3(4):202–206. doi: 10.1016/j.smhs.2021.10.003.