
Abstract
Background
Short-term exposure to major air pollutants (O3, CO, NO2, SO2, PM10, and PM2.5) has been associated with respiratory risk. However, evidence on the risk of chronic obstructive pulmonary disease (COPD) exacerbations is still limited. The present study aimed at evaluating the associations between short-term exposure to major air pollutants and the risk of COPD exacerbations.
Methods
After a systematic search up until March 30, 2016, in both English and Chinese electronic databases such as PubMed, EMBASE, and CNKI, the pooled relative risks and 95% confidence intervals were estimated by using the random-effects model. In addition, the population-attributable fractions (PAFs) were also calculated, and a subgroup analysis was conducted. Heterogeneity was assessed by I2.
Results
In total, 59 studies were included. In the single-pollutant model, the risks of COPD were calculated by each 10 μg/m3 increase in pollutant concentrations, with the exception of CO (100 μg/m3). There was a significant association between short-term exposure and COPD exacerbation risk for all the gaseous and particulate pollutants. The associations were strongest at lag0 and lag3 for gaseous and particulate air pollutants, respectively. The subgroup analysis not only further confirmed the overall adverse effects but also reduced the heterogeneities obviously. When 100% exposure was assumed, PAFs ranged from 0.60% to 4.31%, depending on the pollutants. The adverse health effects of SO2 and NO2 exposure were more significant in low-/middle-income countries than in high-income countries: SO2, relative risk: 1.012 (95% confidence interval: 1.001, 1.023); and NO2, relative risk: 1.019 (95% confidence interval: 1.014, 1.024).
Conclusion
Short-term exposure to air pollutants increases the burden of risk of COPD acute exacerbations significantly. Controlling ambient air pollution would provide benefits to COPD patients.
Introduction
Air pollution has been a serious environmental problem and a major concern for public health worldwide. It continues to be a major environmental health risk, particularly in developing countries where the motor vehicle traffic and industrialization increase quickly.Citation1 The respiratory system (tract and lung) is vulnerable to air pollutants, including ozone (O3), carbon monoxide (CO), nitrogen dioxide (NO2), sulfur dioxide (SO2), and particulate matters (PM2.5, PM10). In the course of pulmonary ventilation and gas exchange, these pollutants could induce oxidative stress and inflammation, resulting in airway injury and dysfunction.Citation2
Chronic obstructive pulmonary disease (COPD) is the third leading cause of mortality worldwide. It is estimated that the number of COPD patients has reached a record of 7.3 billion in 2015.Citation3 Factors that cause exacerbation of COPD include clinical and medical care status, natural and social environmental changes, and lifestyles.Citation4 The exacerbation symptoms mainly include the increase in dyspnea, sputum production, or purulence and then the emergency hospitalization or even mortality.Citation5 In some parts of the world, acute exacerbation of COPD accounts for 1 of 10 leading causes of hospital admission, which bring formidable challenges to the world health and socioeconomic systems.Citation6
The acute effects of air pollution exposure on COPD exacerbations have been investigated by several studies, but the results still remain inconsistent. Some reported that air pollutions significantly increased the risk of exacerbation or mortality,Citation7,Citation8 whereas others found no associationsCitation9,Citation10 or relationships only for selected pollutants.Citation11,Citation12 Moreover, several recent investigations were conducted in certain regions and were just focused on particulate air pollutions.
To the authors’ knowledge no comprehensive and systematic meta-analysis has yet been published to investigate the association of acute COPD exacerbations with short-term air pollutants exposure. Therefore, the aim of the present study was to systematically review the evidence evaluating the acute risk for COPD patients when exposed to short-term air pollution.
Methods
Search strategy
Systematic searches were performed to identify the studies on the associations between major air pollutants and COPD exacerbation. The comprehensive online electronic databases included both English and Chinese databases through March 30, 2016: Web of Science (1956–2016), Ovid MEDLINE and Ovid MEDLINE in the process (1946–2016), EMBASE (1974–2005), Environmental Sciences and Pollution Management Index, CINAHL, Google Scholar and Cochrane database (2005–2016), and CNKI. Moreover, references were checked for additional publication details. Supplementary material S1 contains the search strategy. Duration of up to 7 days (lag6) was selected. If the included papers had insufficient data, the corresponding authors were contacted by email, and the papers were excluded only if there was no response from the corresponding authors.
Selection of studies
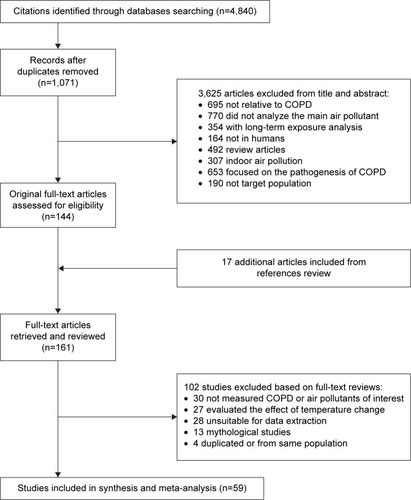
The inclusion criteria (Supplementary material S2) were as follows: 1) a case-crossover or time-series study; and 2) evaluation of the short-term effects of air pollutants on the acute risk of COPD with recorded end points. summarizes the selection procedures in a flow chart.
Figure 1 PRISMA flow chart of identified, included, and excluded studies.
One reviewer (JH Li) performed all the initial evaluations of titles and abstracts. The other investigator (QY Huang) randomly assessed 500 samples, and no controversy was found. Full text of these potential studies was then screened to determine the eligibility by these two authors independently. During full-text selection, conflicts were settled by consensus or adjusted by a third reviewer (SZ Sun).
Quality score assessment
This meta-analysis was conducted according to the items of PRISMA and MOOSE.Citation13,Citation14 Although Mustafic et al suggested to evaluate the quality of time-series or case-crossover studies,Citation15 there were still no validated scales recommended.Citation16 Therefore, a 4-component scoring system (0–1 point for each item) was designed as follows: 1) the quality of air pollution assessment (<25% of the values for one specific day were missing);Citation15 2) the validation of COPD exacerbation (the disease was coded according to the International Classification of Diseases, Revision 10, American Thoracic Society or other laboratory/clinical prognosis golden criteria, such as FEV1/FVC <0.7 for lung function); 3) the adjustment for confounders (temperature, seasonality, long-term trend, etc were adjusted); and 4) the generalizability of the outcomes (providing clear defined hospitals or health maintenance organizations).Citation17
Data extraction and statistical synthesis
The two investigators (JH Li and QY Huang) conducted the data extraction independently, and discordance was resolved by discussing with another researcher (LW Tian). By assuming a linear relationship between air pollution and COPD, the relative risks (RRs) with 95% confidence interval (CI) for a standardized increment of pollutants’ concentrations were pooled as follows: 10 μg/m3 for PM2.5, PM10, NO2, SO2, and O3 and 100 μg/m3 for CO. These values were frequently used in the previous air-pollution-related studies.Citation18 If percentage change with 95% CI were reported, then it could be transformed to RR with 95% CI. Besides, if odds ratios were found, they could be considered equivalent to RRs in time-series or case-crossover studies.Citation19 Then, the standardized risk was unified according to the method by Yang et al.Citation17
The present study was designed to have short-term exposure because the risk factors varied constantly in this period and could not be promptly confounded by fluctuating and meteorological parameters.Citation20 There had been no standard criteria for reporting lag patterns so far, and most studies employed single-day lag; therefore, lag selection procedure was based on “priori lag” theory of Atkinson et al.Citation11 Briefly, when only one lag estimate was presented, it would be adopted first; if numerous lags were reported, our selection was based on the following algorithms: 1) the most frequently used lag in all the selected studies was under consideration; and 2) compared to the cumulative/distributed lags, single lags were chosen as priorities.
The heterogeneity was assessed by I2. When heterogeneity was significant (I2>25%), the random-effects model was applied; otherwise, the fixed-effects model was used.Citation21 In order to explore the sources of heterogeneity, subgroup and meta-regression analyses were performed based on study design, population location, age, and outcome category. In order to determine whether the findings could be affected by removing one or two studies, sensitivity analysis was conducted to explore robustness.Citation22 If the omission of any study would not affect the overall results, then the outcome of the review can be regarded with a higher degree of certainty.Citation23
The population-attributable fractions (PAFs) are reduced proportions of disease hospitalization or mortality in the population when the exposure risk factor was reduced to an expected scenario. First, they were assumed to be 100% in some industrialized areas according to the recognized method by Dr Mustafic.Citation15 Besides, in some light-polluted regions, the prevalence percentages were suggested to be assumed lower, in which case the estimated prevalence values were 80% and 20% in the present study.Citation19 The equation is as follows: {PAF = k*(RR−1)/[k*(RR−1) +1]} (where k indicates the air pollution exposure percentages).Citation15
Publication bias was evaluated by using Begg’s funnel plot method and confirmed by Egger’s method.Citation24 Asymmetry was then corrected through trim and fill method, and an adjusted summary was achieved by using all the original studies together with “filled” data.Citation19 Moreover, the pooled effect estimates based on income status of country defined by the gross national income per capita of World Bank were also explored.Citation25
The statistical analyses were conducted by using STATA Version 12.1 (STATA/SE, College Station, TX, USA) and R Software (Version 3.1.2). Significance for pooled estimates was defined as two-sided P<0.05.
Results
Literature search and study characteristics
shows the selection process of the identified 4,840 studies. A total of 59 studies fulfilled all the criteria and were included in the analysis, consisting of 13 case-crossover studies and 46 time-series studies.
summarizes the basic characteristics of the included publications. The number of populations ranged from 4,989 to 58 million. All the research studies were published between 1992 and 2015 and were performed in Asia (People’s Republic of China, Japan, Korea, and India), North America (the USA and Canada), South America (Mexico and Brazil), Australia, and Europe; 12 citations focused on the association between short-term air pollution exposure and COPD mortality, whereas 41 focused on the COPD emergency hospitalization. The final 6 citations paid attention to both. The most frequently reported age-group was all age-group, followed by the group >65 years old. shows the potentially adjusted confounders. Furthermore, Table S1 lists the components of air pollution and average concentrations. Most publications provided multiple estimates for single lags (eg, lag0, lag1, and lag2), whereas some provided cumulative or distributed lags that were adopted only in the overall analysis. The 4-score system showed that the majority was judged to be of good or intermediate quality.
Table 1 Contextual details of the studies included in the meta analysis
Overall analysis
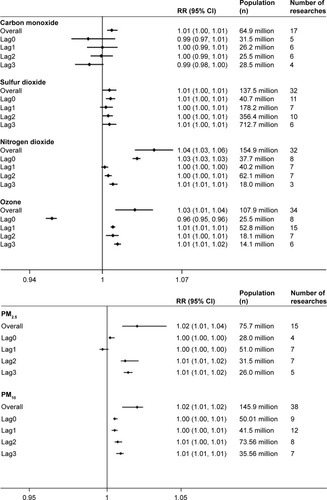
There was a significant association between short-term exposure and the risk of COPD exacerbations for all the gaseous and particulate pollutants (; ). Figure S1 shows the details explicitly. presents PAFs with all the prevalence of exposure. The associations, for gaseous air pollutants, were found to be strongest at lag0 and decreased as the time increased. Conversely, the most significant associations appeared at lag3 for particulate air pollutants.
Table 2 Subgroup analysis by gaseous and particulate pollutants
Figure 2 Associations between gaseous and particular air pollution and COPD risk stratified by time lag (days).
Through sensitivity analysis, after excluding studies that increased risk of bias, no difference was found in the overall effect estimates (Table S2). Publication bias was observed in pollutants of SO2, O3, and PM10 by using Egger’s test for asymmetry P<0.05 (; Figure S2). After adjusting the symmetry with the trim and fill method, it was found that the effect directions of all air pollutants did not change, but it yielded the effects adjusted for funnel plot asymmetry as expected.
Subgroup analyzes
Lag exposure
Based on the lag exposure subgroup analysis, it was found that the following outcome of lag subgroup analysis for each air pollutant were consistent with the results of overall analysis (RR [95% CI], I2, Egger’s test [P]): lag0 for SO2 (1.007 [1.003, 1.011]; 91.5%; P=0.31), NO2 (1.030 [1.026, 1.033]; 94.9%; P=0.78), and PM2.5 (1.002 [1.001, 1.005]; 76.8%; P=0.36); lag1 for CO (1.000 [0.985, 1.005]; 61.4%; P=0.41); lag3 for O3 (1.013 [1.010, 1.016]; 5.90%; P=0.35) and PM10 (1.009 [1.006, 1.011]; 55.8%; P=0.12). and Table S3 present more detailed results.
Study quality
This subgroup included 56 citations (20 studies fulfilling the high-quality score of 4 points and 36 studies receiving the middle quality score of 3 points). Except for SO2 and O3, all the other air pollutants revealed valid associations with COPD risk (Table S3). Among them [N, RR (95% CI); Egger’s test, P], NO2 (27 studies; 1.017 [1.015, 1.019]; P=0.147), CO (13 studies; 1.006 [1.002, 1.011]; P=0.163), PM2.5 (15 studies; 1.001 [1.000, 1.001]; P=0.187), and PM10 (34 studies; 1.001 [1.000, 1.001]; P=0.187) were proved to be unfavorable associations.
Property classification
As shown in , this analysis was conducted based on COPD exacerbation outcomes (hospitalization or mortality), geographical location (Asia or non-Asia), population age (all age or age >65 years), and study design (time-series or case-crossover). When classified by geographical locations, the positive relationships were more significant in Asian countries than in the non-Asian countries for air pollutants. Similar associations were also observed in age subgroups: there was a tendency toward stronger relationships between these air pollutants and COPD. The property subgroups of case-crossover study and COPD deaths had borderline significance.
Figure 3 Subgroup analysis for all gaseous and particulate air pollutants stratified by outcome, location, age, and study design.
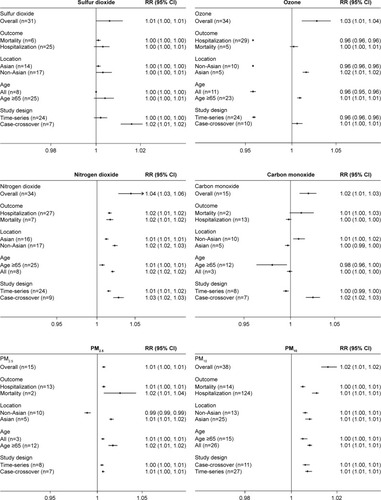
Furthermore, it was also identified that subgroup of age >65 years for SO2 and O3, COPD mortality subgroup for NO2, CO, and PM2.5, and subgroup of non-Asia population for PM10 reduced the heterogeneities of their pooled effects compared to overall analyzes. Table S4 shows further details.
Stratification by national income
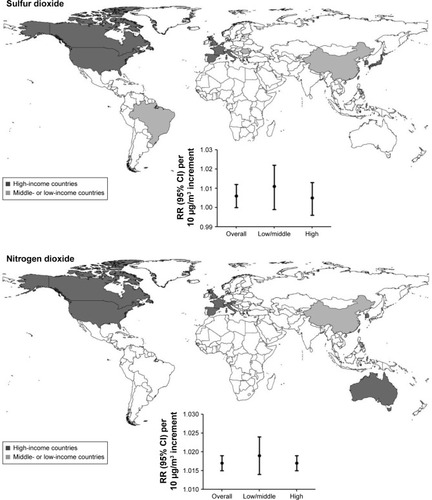
Among all the included studies, 20% of the publications were from low-/middle-income countries in which ~60% of the population originated from the People’s Republic of China. SO2, NO2, and PM10 were commonly measured in low-/middle-income countries, such as Mexico and Brazil. Compared with the developed countries, the SO2 and NO2 short-time exposure showed more pronounced associations with COPD acute risk in the developing countries. For them, the RRs (95% CI) in low-/middle-income and high-income countries were as follows: SO2, 1.012 (1.001, 1.023) and 1.005 (0.996, 1.014); and NO2, 1.019 (1.014, 1.024) and 1.017 (1.015, 1.019) (). The mean concentrations of SO2 and NO2 in low-/middle-income countries were relatively higher than those of high-income countries, which was particularly concerning for the reason that these countries have disproportionate burdens of global acute exacerbation of COPD.
Figure 4 Cartogram identifying associations between sulfur dioxide and nitrogen dioxide short-term exposure and COPD risk stratified by countries of high- and low-/middle-income levels.
Heterogeneity by meta-regression
Considering the substantial heterogeneity exhibited in the overall analysis, meta-regression analysis identified that study design of NO2 (coefficient =−0.166; P=0.014) and O3 (coefficient =−0.072; P=0.017) contributed to heterogeneities significantly (Table S4). However, heterogeneity exploration similar to subgroups of location, age, and COPD subtype showed no significant contributors.
Discussion
Principal findings
To the authors’ concurrent knowledge, this was the first study to report the comprehensive association between main gaseous and particulate pollutants’ short-term exposure and COPD acute risk, indicating that improving air quality could reduce the risk of sudden onset of COPD and the burden of COPD worldwide. The present study found a significant association between short-term exposure to major air pollutants and COPD emergency risk, especially for O3 and NO2. Subgroup analysis showed lower heterogeneities and yielded similar associations in the overall analysis. The pooled estimates stratified by financial levels demonstrated stronger associations in low-/middle-income countries than in high-income countries.
Potential mechanisms
There were plenty of in vivo and in vitro studies to explain the plausible biomedical mechanisms for the relationship between short-term air pollution exposure and adverse outcome of COPD.Citation26,Citation27 One of the main mechanisms was oxidative-mediated.Citation28 Air pollution could absorb chemical substances from the environment, which participated in the production process of reactive oxygen species.Citation29 Oxidative stress could cause an injury in the epithelium of the airway, making the airways of COPD patients more sensitive to further damage, and impair the resistance ability of the immune system.Citation2 Another pathogenesis mechanism is that air pollutants can cause inflammation in the lungs and can further impair the reduced pulmonary function in COPD patients.Citation30 However, the COPD exacerbation-relevant determinants are still largely unknown. As most research studies have focused on smoking and pneumonia risk for COPD exacerbation,Citation4,Citation31,Citation32 further studies considering the significant roles of environmental pollution are required.
Interpretation
In the present analysis, all the air pollutants showed acute disadvantageous effects on COPD patients, especially NO2 and O3. Both of these two gaseous pollutants caused an increased risk of COPD significantly (RR, 95% CI): 1.04, (1.03, 1.06); and 1.03, (1.01, 1.04). One study reported that every 10 μg/m3 increase of O3 and NO2 would result in 0.58% and 0.38% increment in the COPD risk, respectively.Citation33 In addition, exposure to SO2 and CO showed weaker associations with COPD in the present study, which was consistent with a previous study. Fusco et al found that no effects were identified for SO2, and only weak associations was found for CO (2.8% increase per interquartile range (IQR), 1.5 mg/m3).Citation34 NO2 and O3 played important roles in acute respiratory attack, whereas CO seemed to be strongly associated with seasonality, especially in warmer seasons. In combination studies, it was difficult to separate all the estimates of CO by the adjustment of seasonality.Citation34,Citation35 For the different effects of O3 compared to other pollutants, the most important factor is the properties of O3. It is the component of photochemical reaction and shows obvious seasonality fluctuation that could affect the exacerbation rate of COPD patients.Citation15 Moreover, it is relatively more complex to form O3 in the ambient air, depending closely on solar radiation and brightness.Citation36 As for the adjustment of temperature, different methods adopted cause RR estimates to vary, and in the pooled analysis, it is hard to just limit the pollutants to a certain period.Citation37
Particulate pollutants have always been considered to be responsible for the most adverse cardiovascular and respiratory diseases, and some adverse impacts induced by PM2.5 might be aggravated by PM10.Citation19 In the present study, particulate pollutants showed significant adverse impact on COPD patients, which further confirmed that elevated levels of particulate matters in polluted environments could promote the exacerbation of COPD. A study in New Zealand reported an 3.37% increase for each 14.8 mcg/m3 increase in PM10, and an Australian study also showed a 4% increase in admissions for every 10 μg/m3 increase of PM10.Citation38 However, there were still limited studies about PM10 in developing countries. In an Asian time-series study, per 10 μg/m3 increase in PM10 indicated an 0.36% increase in respiratory mortality.Citation39 Because of a disproportional burden of COPD exacerbation in these middle-/lower-income counties, more studies on PM10 are required to explore the combined effects of particulate pollutants.
The heterogeneities of the air pollutants CO, NO2, and O3 were more significant than that of SO2. For particulate pollutants, the heterogeneity of PM2.5 was greater than that of PM10. Subgroup analysis indicated that lag exposure and age >65 years contributed heterogeneities more significantly. In individual studies, they measured daily variations of each pollutant in limited areas for the time period from 0 to 7 days and adjusted different kinds of confounders.Citation27 Therefore, lag exposure for them would be a source of heterogeneity. Subgroup of mortality and age >65 years were also the origins for heterogeneity because COPD showed signs between the ages of 35 and 40 years primarily and it then developed very fast after 65 years. Once exposed to risk factors, COPD patients would exacerbate quickly, and mortality rate increased.Citation40 A high quality study with higher score tends to have the higher methodological quality.Citation41
The current analysis also indicated that the association between SO2 and NO2 short-term exposure and COPD acute risk seemed to be more pronounced in low-/middle-income countries than in high-income countries, and only 20% of the included studies were from low-/middle-income countries, and more than half of them originated from the People’s Republic of China (). This finding was of great importance because urban cities in some developing countries were in a rapid industrialization process and under the threat of severe environmental problems.Citation42 Moreover, data from these countries were scarce, resulting from a lack of cohesive air quality policies, inadequate environmental monitoring, and a paucity of disease surveillance data.Citation19 More monitoring information is in great demand for developing countries in order to investigate the health impacts of air pollutants. Considering the severe air pollution and disproportionate burden of COPD acute risk in the developing countries, this highlighted issue needs more attention.
Practical implications
The findings of the present study have provided evidence for the association between short-term air pollution exposure and the risk of COPD exacerbations. This called for improvement and implementation of regulations on the air quality that will provide measurable benefits to public health. More policies should be implemented to reduce major air pollutants, such as adoption the absorbers of noxious gases before release, utilization of environmentally-friendly fuels, and adoption of advanced technologies.Citation43 Our results urge future research studies on the relationship between concentration of air pollutants and the risk estimation and also for more cooperative actions to issue alerts to high-risk populations in order to facilitate substantial public health benefits.
Limitations
It was acknowledged that several limitations should be considered. First, the lag selection in methodologies was controversial. Exclusion of any lag from lag0 to lag7 might miss considerable information for pooled analysis. In this analysis, all the methodologies used had been reviewed. Therefore, the “priori lag” method was chosen based on the most commonly used approach. Besides, there were still potential sources of bias in the present study: the estimates included were from each publication, and whether multiple hospitalizations might occur for the same patients was not identified. Moreover, the concentration–response relationships are really fundamental references in air quality standards, but lack of details to construct the dose–response functions may limit the ability for setting criteria. Finally, for the air pollutants under the single-pollutant model, underlying interactive effects might exist.Citation44 There was no clearly stated selection of models in combined analysis, and most of the parameters preferred the idea that multiple models for air pollutions in meta-analysis were still imperfect;Citation45 therefore, the single-air pollutant model was used in the present study for estimations.
Conclusion
This systematic review and meta-analysis confirmed that short-term exposure to major air pollutants could significantly increase the risk for COPD exacerbations. Environmental and public health policies that can decrease the concentrations of air pollution might reduce the exacerbation burden of COPD.
Acknowledgments
This work was supported by the National Natural Science Foundation of China (41272180).
Disclosure
The authors report no conflicts of interest in this work.
References
- BerendNContribution of air pollution to COPD and small airway dysfunctionRespirology201621223724426412571
- LiXYGilmourPSDonaldsonKMacNeeWFree radical activity and pro-inflammatory effects of particulate air pollution (PM10) in vivo and in vitroThorax199651121612228994518
- Lopez-CamposJLTanWSorianoJBGlobal burden of COPDRespirology2016211142326494423
- Garcia-AymerichJMonsóEMarradesRMRisk factors for hospitalization for a chronic obstructive pulmonary disease exacerbationAm J Respir Crit Care Med20011641002100711587986
- HawkinsNMViraniSCeconiCHeart failure and chronic obstructive pulmonary disease: the challenges facing physicians and health servicesEur Heart J201334362795280323832490
- LindenauerPKPekowPGaoSCrawfordASGutierrezBBenjaminEMQuality of care for patients hospitalized for acute exacerbations of chronic obstructive pulmonary diseaseAnn Intern Med200614489490316785478
- NeubergerMRabczenkoDMoshammerHExtended effects of air pollution on cardiopulmonary mortality in ViennaAtmos Environ2007413885498556
- PeelJLTolbertPEKleinMAmbient air pollution and respiratory emergency department visitsEpidemiology200516216417415703530
- XuZYuDJingLXuXAir pollution and daily mortality in Shenyang, ChinaArch Environ Health200055211512010821512
- YangQChenYKrewskiDBurnettRTShiYMcGrailKMEffect of short-term exposure to low levels of gaseous pollutants on chronic obstructive pulmonary disease hospitalizationsEnviron Res20059919910516053934
- AtkinsonRWCareyIMKentAJvan StaaTPAndersonHRCookDGLong-term exposure to outdoor air pollution and the incidence of chronic obstructive pulmonary disease in a national English cohortOccup Environ Med2015721424825146191
- PetersAWichmannHETuchTHeinrichJHeyderJRespiratory effects are associated with the number of ultrafine particlesAm J Respir Crit Care Med19971554137613839105082
- MoherDLiberatiATetzlaffJAltmanDGPreferred reporting items for systematic reviews and meta-analyses: the PRISMA statementBMJ2009339b253519622551
- StroupDFBerlinJAMortonSCMeta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis of Observational Studies in Epidemiology (MOOSE) groupJAMA2000283152008201210789670
- MustaficHJabrePCaussinCMain air pollutants and myocardial infarction: a systematic review and meta-analysisJAMA2012307771372122337682
- SavovicJWeeksLSterneJAEvaluation of the Cochrane Collaboration’s tool for assessing the risk of bias in randomized trials: focus groups, online survey, proposed recommendations and their implementationSyst Rev201433724731537
- YangWSWangXDengQFanWYWangWYAn evidence-based appraisal of global association between air pollution and risk of strokeInt J Cardiol2014175230731324866079
- PolonieckiJDAtkinsonRWde LeonAPAndersonHRDaily time series for cardiovascular hospital admissions and previous day’s air pollution in London, UKOccup Environ Med19975485355409326156
- ShahASLangrishJPNairHGlobal association of air pollution and heart failure: a systematic review and meta-analysisLancet201338298971039104823849322
- KanHJiaJChenBAcute stroke mortality and air pollution: new evidence from Shanghai, ChinaJ Occup Health200345532132314646274
- MantelNHaenszelWStatistical aspects of the analysis of data from retrospective studies of diseaseJ Natl Cancer Inst19592271974813655060
- HuangQLiJSunYWangRChengXChenHEfficacy of EGFR tyrosine kinase inhibitors in the adjuvant treatment for operable non-small-cell lung cancer by a meta-analysisChest201514961384139226836897
- LiJHuangQZengFThe prognostic value of global DNA hypomethylation in cancer: a meta-analysisPLoS One201499e10629025184628
- AtkinsonRKangSAndersonHMillsIWaltonHEpidemiological time series studies of PM2.5 and daily mortality and hospital admissions: a systematic review and meta-analysisThorax201469766066524706041
- BarnettAGWilliamsGMSchwartzJThe effects of air pollution on hospitalizations for cardiovascular disease in elderly people in Australian and New Zealand citiesEnviron Health Perspect200611471018102316835053
- GarshickEEffects of short- and long-term exposures to ambient air pollution on COPDEur Respir J201444355856125176946
- SunyerJUrban air pollution and chronic obstructive pulmonary disease: a reviewEur Respir J2001171024103311488305
- MacNeeWDonaldsonKExacerbations of COPDChest20001175390S397S10843983
- KasemoBLausmaaJMaterial-tissue interfaces: the role of surface properties and processesEnviron Health Perspect1994102Suppl 54145
- AbbeyDEBurchetteRJKnutsenSFMcDonnellWFLebowitzMDEnrightPLLong-term particulate and other air pollutants and lung function in nonsmokersAm J Respir Crit Care Med199815812892989655742
- KesslerRFallerMFourgautGMennecierBWeitzenblumEPredictive factors of hospitalization for acute exacerbation in a series of 64 patients with chronic obstructive pulmonary diseaseAm J Respir Crit Care Med199915981581649872834
- AnthonisenNRSmoking, lung function and mortalityThorax20005572973010950888
- GhozikaliMGMosaferiMSafariGHJaafariJEffect of exposure to O(3), NO(2), and SO(2) on chronic obstructive pulmonary disease hospitalizations in Tabriz, IranEnviron Sci Pollut Res Int20152242817282325217280
- FuscoDForastiereFMichelozziPAir pollution and hospital admissions for respiratory conditions in Rome, ItalyEur Respir J2001171143115011491157
- PitardAVielJFSome methods to address collinearity among pollutants in epidemiological time seriesStat Med19971655275449089961
- ChardonBHostSLefrancAMillardFGremyIWhat exposure indicator should be used to study the short-term respiratory health effect of photochemical air pollution? A case study in the Paris metropolitan areaEnvironnement, Risques & Santé200765345353
- EilsteinDQuenelPHedelinGKleinpeterJArveilerDSchafferPAir pollution and myocardial infarction. Strasbourg France, 1984–1989Rev Epidemiol Sante Publique20014911325 French11226915
- MeszarosDMarkosJFitzGeraldDGWaltersEHWood-BakerRAn observational study of PM10 and hospital admissions for acute exacerbations of chronic respiratory disease in Tasmania, Australia 1992–2002BMJ Open Respir Res201521e000063
- AtkinsonRWCohenAMehtaSAndersonHRSystematic review and meta-analysis of epidemiological time-series studies on outdoor air pollution and health in AsiaAir Qual Atmos Health201154383391
- PavordIDJonesPWBurgelPRRabeKFExacerbations of COPDInt J Chron Obstruct Pulmon Dis201611213026937187
- SterneJACEggerMSmitGDInvestigating and dealing with publication and other biases in meta-analysisBMJ200132310110511451790
- KanHChenBHongCHealth impact of outdoor air pollution in China: current knowledge and future research needsEnviron Health Perspect20091175A18719478975
- ZhangJJSmithKRHousehold air pollution from coal and biomass fuels in China: measurements, health impacts, and interventionsEnviron Health Perspect2007115684885517589590
- SchwartzJMorrisRAir pollution and hospital admissions for cardiovascular disease in Detroit, MichiganAm J Epidemiol1995142123357785670
- GasparriniAArmstrongBReducing and meta-analysing estimates from distributed lag non-linear modelsBMC Med Res Methodol201313123297754
- KloogINordioFZanobettiACoullBAKoutrakisPSchwartzJDShort term effects of particle exposure on hospital admissions in the Mid-Atlantic states: a population estimatePloS One201492e8857824516670
- MengXWangCCaoDWongC-MKanHShort-term effect of ambient air pollution on COPD mortality in four Chinese citiesAtmospheric Environment201377149154
- Tellez-RojoMRomieuIRuiz-VelascoSLezanaMHernandez-AvilaMDaily respiratory mortality and PM10 pollution in Mexico City: importance of considering place of deathEuropean Respiratory Journal200016339139611028649
- WordleyJWaltersSAyresJGShort term variations in hospital admissions and mortality and particulate air pollutionOccupational and Environmental Medicine19975421081169072018
- YorifujiTSuzukiEKashimaSHourly differences in air pollution and risk of respiratory disease in the elderly: a time-stratified case-crossover studyEnvironmental Health20141316725115710
- SchikowskiTAdamMMarconAAssociation of ambient air pollution with the prevalence and incidence of COPDEur Respir J201444361462624488569
- TaoYMiSZhouSWangSXieXAir pollution and hospital admissions for respiratory diseases in Lanzhou, ChinaEnvironmental Pollution201418519620124286694
- MoolgavkarSHLuebeckEGAndersonELAir pollution and hospital admissions for respiratory causes in Minneapolis-St. Paul and BirminghamEpidemiology19973643709209848
- HinwoodADe KlerkNRodriguezCThe relationship between changes in daily air pollution and hospitalizations in Perth, Australia 1992–1998: a case-crossover studyInternational Journal of Environmental Health Research2006161274616507479
- MilutinovicSNikicDStosicLStankovicABogdanovicDShort-term association between air pollution and emergency room admissions for chronic obstructive pulmonary disease in Nis, SerbiaCentral European Journal of Public Health2009171819418713
- ArbexMAde Souza ConceiçãoGMCendonSPUrban air pollution and chronic obstructive pulmonary disease-related emergency department visitsJournal of Epidemiology and Community Health2009631077778319468016
- ForastiereFStafoggiaMBertiGParticulate matter and daily mortality: a case-crossover analysis of individual effect modifiersEpidemiology200819457158018467959
- KoFWTamWWongTWTemporal relationship between air pollutants and hospital admissions for chronic obstructive pulmonary disease in Hong KongThorax200762978078517311838
- ZanobettiASchwartzJDockeryDWAirborne particles are a risk factor for hospital admissions for heart and lung diseaseEnvironmental Health Perspectives200010811107111102299
- MorganGCorbettSWlodarczykJAir pollution and hospital admissions in Sydney, Australia, 1990 to 1994American Journal of Public Health19988812176117669842371
- AndersonHSpixCMedinaSAir pollution and daily admissions for chronic obstructive pulmonary disease in 6 European cities: results from the APHEA projectEuropean Respiratory Journal1997105106410719163648
- ChenYYangQKrewskiDShiYBurnettRTMcGrailKInfluence of relatively low level of particulate air pollution on hospitalization for COPD in elderly peopleInhalation Toxicology2004161212514744661
- WongTTamWYuTWongAAssociations between daily mortalities from respiratory and cardiovascular diseases and air pollution in Hong Kong, ChinaOccupational and Environmental Medicine2002591303511836466
- TeniasJMBallesterFPerez-HoyosSRiveraMLAir pollution and hospital emergency room admissions for chronic obstructive pulmonary disease in Valencia, SpainArchives of Environmental Health2002571414712071359
- QiuHYuIT-sTianLEffects of coarse particulate matter on emergency hospital admissions for respiratory diseases: a time-series analysis in Hong KongEnvironmental Health Perspectives2012120457222266709
- StiebDMSzyszkowiczMRoweBHLeechJAAir pollution and emergency department visits for cardiac and respiratory conditions: a multi-city time-series analysisEnviron Health2009825101186
- WongTWLauTSYuTSAir pollution and hospital admissions for respiratory and cardiovascular diseases in Hong KongOccupational and Environmental Medicine1999561067968310658547
- SchoutenJVonkJDe GraafAShort term effects of air pollution on emergency hospital admissions for respiratory disease: results of the APHEA project in two major cities in The Netherlands, 1977–89Journal of Epidemiology and Community Health199650Suppl 1s22s298758220
- SauerzapfVJonesAPCrossJEnvironmental factors and hospitalisation for chronic obstructive pulmonary disease in a rural county of EnglandJournal of Epidemiology and Community Health200963432432819208692
- Medina-RamonMZanobettiASchwartzJThe effect of ozone and PM10 on hospital admissions for pneumonia and chronic obstructive pulmonary disease: A national multicity studyAmerican Journal of Epidemiology2006163657958816443803
- JanssenNFischerPMarraMAmelingCCasseeFShort-term effects of PM 2.5, PM 10 and PM 2.5–10 on daily mortality in the NetherlandsScience of the Total Environment2013463202623787105
- LinYChangSLinCChenYWangYComparing ozone metrics on associations with outpatient visits for respiratory diseases in Taipei Metropolitan areaEnvironmental Pollution201317717718423333210
- BatesonTFSchwartzJWho is sensitive to the effects of particulate air pollution on mortality? A case-crossover analysis of effect modifiersEpidemiology200415214314915127905
- SunyerJSchwartzJTobiasAMacfarlaneDGarciaJAntoJMPatients with chronic obstructive pulmonary disease are at increased risk of death associated with urban particle air pollution: A case-crossover analysisAmerican Journal of Epidemiology20001511505610625173
- KanHChenBAir Pollution and Daily Mortality in Shanghai: A Time-Series StudyArchives of Environmental Health200358636036714992311
- BragaALFZanobettiASchwartzJThe lag structure between particulate air pollution and respiratory and cardiovascular deaths in 10 US citiesJournal of Occupational and Environmental Medicine2001431192793311725331
- SchwartzJDockeryDWIncreased mortality in Philadelphia associated with daily air pollution concentrationsAmerican Review of Respiratory Disease199214536006041546841
- FischerPHoekGBrunekreefBVerhoeffAVan WijnenJAir pollution and mortality in the Netherlands: are the elderly more at risk?European Respiratory Journal20032140 suppl34s38s
- WongPMLeesANLouwJEmphysema in young adult survivors of moderate-to-severe bronchopulmonary dysplasiaEuropean Respiratory Journal200832232132818385172
- JanssenNAHSchwartzJZanobettiASuhHHAir conditioning and source-specific particles as modifiers of the effect of PM10 on hospital admissions for heart and lung diseaseEnvironmental Health Perspectives200211014349
- DominiciFPengRDBellMLFine particulate air pollution and hospital admission for cardiovascular and respiratory diseasesJAMA2006295101127113416522832
- YangCYChenCJAir pollution and hospital admissions for chronic obstructive pulmonary disease in a subtropical city: Taipei, TaiwanJournal of Toxicology and Environmental Health Part A: Current Issues2007701412141219
- SchwartzJPM10, ozone, and hospital admissions for the elderly in Minneapolis-St. Paul, MinnesotaArchives of Environmental Health19944953663747944569
- SchwartzJAir pollution and hospital admissions for the elderly in Birmingham, AlabamaAmerican Journal of Epidemiology199413965895988172170
- SunyerJSaezMMurilloCCastellsagueJMartinezFAntoJMAir pollution and emergency room admissions for chronic obstructive pulmonary disease: A 5-year studyAmerican Journal of Epidemiology199313777017058484361
- LippmannMItoKNadasABurnettRAssociation of particulate matter components with daily mortality and morbidity in urban populationsResearch Report (Health Effects Institute)200095572 discussion 73–82
- DabWMedinaSQuenelPShort term respiratory health effects of ambient air pollution: results of the APHEA project in ParisJournal of Epidemiology and Community Health199650Suppl 1s42s468758223
- LeitteAMPetrescuCFranckURespiratory health, effects of ambient air pollution and its modification by air humidity in Drobeta-Turnu Severin, RomaniaScience of the Total Environment2009407134004401119375151
- PandeJBhattaNBiswasDOutdoor air pollution and emergency room visits at a hospital in DelhiIndian Journal of Chest Diseases and Allied Sciences2002441132011845928
- CireraLGarcía-MarcosLGiménezJDaily effects of air pollutants and pollen types on asthma and COPD hospital emergency visits in the industrial and Mediterranean Spanish city of CartagenaAllergologia et Immunopathologia201240423123721890258
- YangC-YChenC-JAir pollution and hospital admissions for chronic obstructive pulmonary disease in a subtropical city: Taipei, TaiwanJournal of Toxicology and Environmental Health, Part A200770141214121917573635
- LeeI-MTsaiS-SChangC-CHoC-KYangC-YAir pollution and hospital admissions for chronic obstructive pulmonary disease in a tropical city: Kaohsiung, TaiwanInhalation Toxicology200719539339817365044
- PeacockJLAndersonHRBremnerSAOutdoor air pollution and respiratory health in patients with COPDThorax2011 thx.2010.155358
- ZhangZWangJChenLImpact of haze and air pollution-related hazards on hospital admissions in Guangzhou, ChinaEnvironmental Science and Pollution Research20142164236424424306726
- ChoJChoiYJSuhMAir pollution as a risk factor for depressive episode in patients with cardiovascular disease, diabetes mellitus, or asthmaJournal of Affective Disorders2014157455124581827
- TianLHoKFWangTAmbient carbon monoxide and the risk of hospitalization due to chronic obstructive pulmonary diseaseAmerican Journal of Epidemiology11591801211591167
- ToTFeldmanLSimatovicJHealth risk of air pollution on people living with major chronic diseases: a Canadian population-based studyBMJ Open201559e009075
- CaiJChenRWangWXuXHaSKanHDoes ambient CO have protective effect for COPD patient?Environ Res2015136212625460616