
Abstract
Objective
To describe the rate and demographics of pain among Vietnamese people in 48 provinces and describe the impact of pain on individuals, levels of satisfaction with treatment results, and behavior of pain sufferers.
Methods
The cross-sectional study was conducted in adults presenting to outpatient clinics throughout 48 provinces in Vietnam and were randomly selected for inclusion in this study. A physician trained to administer a questionnaire in a standardized fashion interviewed each patient and collected data regarding gender, age, career, acute and chronic pain, diagnoses, treatment, and satisfaction with treatment.
Results
There were 12,136 respondents (50.65% male and 49.35% female) from 48 of the 63 provinces in Vietnam. About 86.53% of respondents reported experiencing pain that affected their daily lives, with 24.10% complaining of acute pain and 62.43% having chronic pain. About 67.71% reported pain that affected job performance. Headache was the most common complaint in 35.43% of the respondents. Fewer than half (43.35%) of all patients with pain sought help from a doctor; only a quarter (27.50%) sought help within 1 month of experiencing that pain. A majority (61.98%) of patients who did seek help were satisfied with treatment results. The median cost of treatment was between 150 and 250 USD.
Conclusion
Pain severe enough to impact patients’ daily lives is common in Vietnam. Treatment costs are a significant economic burden and may help explain why only a minority of patients seek treatment. Access to lower cost, effective treatment for pain should be improved.
Introduction
Pain is a common health care problem not only in terms of medical effects but also due to its socioeconomic impact. Many large-scale epidemiological surveys of pain have been conducted in developed countries such as Germany, the Netherlands, Canada, Japan, and other countries.Citation1–Citation5 Causes of chronic pain were different between surveys and countries, but the most common were osteoarthritis and lower back pain.Citation6–Citation9 The results in some studies have shown that the rate of chronic pain is higher in females than in males.Citation10–Citation12 Chronic pain is associated with increasing age and the elderly are the most vulnerable population to suffer from.Citation12,Citation13 In developing countries, chronic pain is of more concern as it leads to decreasing quality of life. Inadequate or undertreated chronic pain affects people’s daily activities and behavior which in turn contribute to a substantial rate of depression and anxiety. Few reports have investigated the prevalence of pain in community and reflected the real status about how chronic patients were managed.Citation14–Citation16 Currently, there is no any published epidemiological data concerning pain in Vietnam.
The objectives of this study were to 1) determine the prevalence and demographics of pain in Vietnam’s 48 provinces; 2) explore the impact of pain on daily activities including employment; and 3) gain a better understanding of the practices, cost, and satisfaction associated with treatment.
Methods
The cross-sectional study was conducted in adults presenting to outpatient clinics. Data were collected between December 2014 and May 2015. Our investigators surveyed hospitals in 48 of the 63 provinces, representing all seven economic regions of Vietnam ().
Table 1 Survey site
The Vietnamese population in 2015 was used as the standard population.
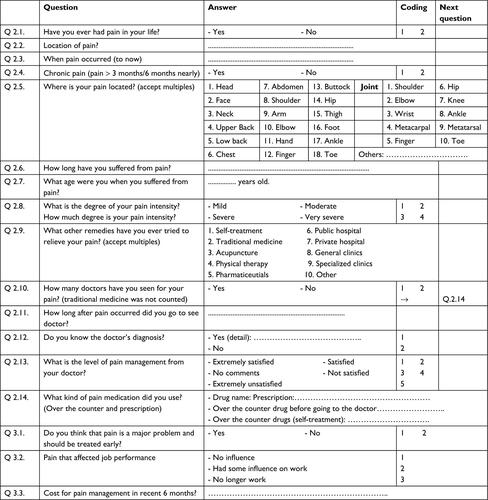
All the respondents received care in outpatient facilities at center of medicine or clinics. Respondents were excluded from the study if they were younger than 10 years. Respondents with pain who were currently involved in clinical trials were excluded to ensure that the data reflected respondents who were receiving standard treatment for their pain. Our questionnaire () was adapted from the one used by Breivik et al.Citation5 The interviews were conducted in Vietnamese. The corresponding author (Nguyen Trung Kien) translated the original questionnaire to a Vietnamese version before starting study. All patients provided written informed consent. The study was conducted in accordance with the Declaration of Helsinki.
The initial questionnaire was a screening interview to assess the rate of pain within each province, age and gender of respondents, the duration of pain, time when pain occurred, location of pain. The respondents were considered to suffer from chronic pain if they have 1) pain persisting for ≥3 months, 2) pain felt within the preceding 1 month, and 3) frequency of pain feeling ≥2 times/week. Respondents who fulfilled these screening criteria of the initial screening questionnaire were then interviewed in depth. Questions in the in-depth interview assessed: 1) demographics; 2) frequency, duration, and intensity of pain; 3) the impact of pain on respondents’ work and quality of life; 4) attitude of respondents toward their pain and its treatment; 5) respondents’ interaction with health care professionals, including how many doctors respondents had visited, how often they had seen them, and how long they had been seeing them; and 6) treatments, including prescription and non-prescription medicines and non-medication strategies.
Doctors working at general hospitals and medical centers in the provinces were selected to interview patients, and were trained to administer the questionnaire in a standardized fashion. The survey data were collected and analyzed in one center. Data were analyzed by SPSS software version 20.1.
This study was performed after obtaining approval from the ethics committee of Military Hospital 103.
Results
Of the 12,136 respondents screened, 10,501 (86.53%) had experienced significant pain at some time during their lives, with 7,576 (62.43%) reporting pain that was chronic in nature. A total of 3,247 (26.76%) respondents had experienced pain for at least 12 months. In total, 10,501 respondents reported suffering from pain and their interviews yielded the following data.
Demographics
Patients who reported pain were evenly distributed between the two genders (50.65% female, 49.35% male). Those under 40 years of age appeared to suffer less, whereas the 41–70 years age group appeared to more likely suffer from pain than others ().
Table 2 Age of respondents
Pain characteristics
The duration of pain was often prolonged. A majority of respondents suffered from chronic pain, as mentioned previously (62.43%; ).
Table 3 Duration of pain
presents the most commonly reported body locations and causes of pain. Headache and neck/back pain were most common.
Table 4 Body locations of pain
The intensity of reported pain is presented in .
Table 5 Intensity of pain
Impact of pain
Impact of pain on daily activities
To gauge the impact of pain on respondents’ lives, the interviewers read a list of activities and asked respondents if their daily activities or employment activities were limited by pain. About 86.53% of the respondents reported that pain affected their daily lives and 67.71% reported that pain affected their jobs.
Treatment practice
Respondent’s attitudes
The interviewers read a list of statements to respondents to determine their attitudes and beliefs about their pain. About 81.46% of respondents considered their pain to be a part of their medical condition.
Pain management
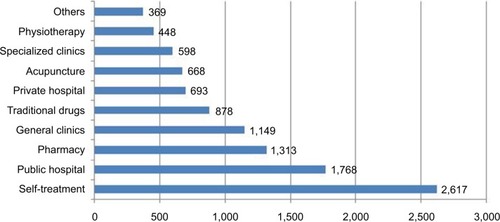
The services patients sought for treatment are shown in . The most common method was self-treatment.
Figure 1 Pain management.
Visits to doctors
About 43.35% of respondents (4,553) had visited doctors; 63.42% of them had seen their doctor in the first month, while only 2.55% had seen their doctor after 1 year. About 56.65% of respondents had not seen their doctor at all ().
Table 6 Visits to doctor
Satisfaction with treatment for pain
About 42.89% of respondents were satisfied with the treatment they received for their pain, while 19.99% were unsatisfied and 3.23% had nothing to disclose ().
Table 7 Treatment satisfaction
Cost of pain treatment
According to the 7,537 respondents who answered to the question regarding the cost of treatment, the median cost of treatment was between 150 and 250 USD. Only a small number of persons (0.20%) paid more than 1,000 USD for treatment ().
Table 8 The cost of treatment for 6 months
Discussion
It is clear from this large-scale survey of 12,136 respondents that pain is very common in Vietnam. Data were collected from 48 of the 63 provinces, which included all seven major economic areas in Vietnam. Doctors involved in conducting the survey were trained in social communication and administering the questionnaire. Thus, we are confident that the specific prevalence data for pain are valid for the documented provinces.
Geographically, respondents included in this study were located throughout Vietnam. Twenty-six provinces had over 100 respondents and two large cities (Hanoi and Ho Chi Minh City) accounted for more than 1,000 respondents each.
Our result showed that nearly all respondents suffered from significant pain at some point in their lives, and that chronic pain impacting daily activities and employment was very common. One reason that the prevalence of pain was high in this study may be that we surveyed persons who had presented to an outpatient clinic with some complaint, as opposed to a random survey of the population at large. Therefore, our pre-test probability was likely elevated. Interestingly, this result is similar to the study of Boerlageand et al, which found that the prevalence of chronic pain was 69% in three Dutch residential homes.Citation2 In postal surveys, the prevalence was 39.3% in Japan and 35.5% in Ireland.Citation4,Citation16 With telephone interviewing, with or without the assistance of computer, the prevalence of chronic pain was found to vary from 13% to 45.9%.Citation3,Citation5,Citation7,Citation9,Citation14
Our investigation excluded children below the age of 10 years (16.4% of Vietnam’s population per 2015 census data), because the etiology, assessment, treatment, and natural course of pain in children are substantially different from adults. Pain in children is beyond the scope of this study.
The prevalence of pain was high in elderly persons,Citation18,Citation19 and management in this population was more complicated.Citation18,Citation20,Citation21 The most frequent location of pain was joints, and the rate was found to be higher in females than in males.Citation10–Citation12 The results of our study also indicated that the prevalence of pain was higher in females (53.0%) than in males. Similar findings have been noted in LibyaCitation11 and in other countries, particularly in older females.Citation9,Citation10,Citation17
Pain is one of the most common reasons for seeking medical attention. People seek health care for pain, not only to improve their physical health but also because pain interferes with psychological and social health. Pain has deleterious effects on mental health, employment status, sleep, and personal relationships.Citation22,Citation23 Psychosocial factors, including individual attitudes about pain and learned coping mechanisms, have particularly strong effects upon daily activities and quality of life, in some cases exceeding the influence of simple pain intensity.Citation24 Functional limitations vary with the type of pain, with low back and multiple pain localizations correlating with the most functional limitations.Citation24 This survey demonstrated that pain has a negative impact on daily activities (88.16% unpleasant, 67.71% work-related).
However, the most common choice patients made regarding pain management was self-treatment. Apart from inadequate relief, this may result in delayed diagnosis of related medical problems and a poor prognosis of otherwise treatable ailments. The next most common choices were seeking help at public hospitals, pharmacies, and general clinics. This reluctance to seek professional attention may be rooted in a Vietnamese cultural preference to treat diseases at home rather than in hospital. This might be due to the fact that the professional medical establishment in Vietnam has not paid enough attention to pain management, and that there is room to improve appreciation for diagnosis and treatment of both acute and chronic pain.
Inadequate or undertreated pain significantly reduces the ability of many patients to participate in daily activities and work. An understanding of individual needs is essential in pain management.Citation25 In our study, 24.92% of respondents opted for self-treatment at home. For moderate to severe pain, treatment at home is often suboptimal;Citation26 in many cases, optimal management may require a short course of opioids,Citation27 which may be unavailable to those who choose self-treatment. Dureja et al showed that the majority (68%) of their respondents were treated for pain with over-the-counter (OTC) drugs, and most were taking nonsteroidal drug (95%).Citation14 In Müller-Schwefe’s study, 35% of the respondents took pain medication that was not prescribed by their doctor,Citation28 presenting potential safety and legal issues. Breivik’s survey of chronic pain in Europe showed that even among patients who sought help from a doctor, very few were managed by pain specialists and 40% received inadequate pain management.Citation5
The current review of literature revealed many factors that limited the possibility of achieving effective pain management by health care systems, medical staff, and patients.Citation29 Health care system is the first fundamental barrier that is related to poor pain management. According to statistics, patients are likely to not receive analgesic medication when required and treatment is likely to be delayed or ineffective.Citation30,Citation31 Vietnam has very limited resources and few pain specialists to care for patients with pain, and medical staff in pain management are not professional as well because there is no any training course in medical universities. Furthermore, other big hindrance is that patients usually buy analgesic agents by themselves from pharmacy store without prescription from doctors (). All of these factors led to inadequate pain management among Vietnamese adults.
Other reason is financial problems. The economic burden to the patient is substantial in a developing country. In our survey, the average cost was 200 USD/person. In Vietnam, the poverty threshold is less than 600 USD/year. The cost of pain management represents a significant burden for affected people. Vietnam is a developing country and we must consider how the economic situation of its people affects the prevalence and treatment of pain. In the survey conducted by Tsang et al, there was no obvious association between the prevalence of chronic pain and economic situation.Citation17
Satisfaction with treatment is an increasingly popular outcome measure in pain management. In our survey, 58.97% of respondents were either satisfied or extremely satisfied with their pain control. These results are in line with those reported by McCracken et al.Citation32 Importantly, 37.8% of respondents were either dissatisfied or extremely dissatisfied. We suspect that a combination of inadequate treatment, high cost of treatment, relatively high pain intensity (23.7% of our respondents rated their pain as severe), and limitation in health care system are largely responsible for this dissatisfaction. Nursing homes involved in pain management in the Netherlands showed that the satisfaction rate was 60%,Citation33 suggesting that poor pain control may be a worldwide issue. Awareness and knowledge about pain assessment and treatment need to be raised not only for medical staff but also for all residents.
Conclusion
Pain is common in Vietnam, with headache and neck/back pain accounting for the majority of ailments. Many individuals with chronic pain suffer limitations in their daily activities, including employment. Treatment is often limited by the economic situation of patients and their reluctance to seek professional assistance. There are many opportunities to improve the accessibility and quality of pain management in Vietnam.
Acknowledgments
The authors thank Mr Gaurav Kumar for his comments on an earlier draft. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplementary material
Figure S1 Pain survey questionnaire
Notes: Adapted with permission from Breivik H, Collett B, Ventafridda V, Cohen R, Gallacher D. Survey of chronic pain in Europe: prevalence, impact on daily life, and treatment. Eur J Pain. 2006;10(4):287–333. © 2005 European Federation of Chapters of the International Association for the Study of Pain. Published by Elsevier Ltd. All rights reserved.Citation1 The interviews were conducted in Vietnamese. The corresponding author (Nguyen Trung Kien) translated the original questionnaire to a Vietnamese version before starting study.
Reference
- BreivikHCollettBVentafriddaVCohenRGallacherDSurvey of chronic pain in Europe: prevalence, impact on daily life, and treatmentEur J Pain200610428733316095934
Disclosure
The authors report no conflicts of interest in this work.
References
- HenslerSHeinemannDBeckerMTChronic pain in German general practicePain Med20091081408141520021600
- BoerlageAAvan DijkMStronksDLde WitRvan der RijtCCPain prevalence and characteristics in three Dutch residential homesEur J Pain200812791091618267371
- MoulinDEClarkAJSpeechleyMMorley-ForsterPKChronic pain in Canada – prevalence, treatment, impact and the role of opioid analgesiaPain Res Manag20027417918412518174
- InoueSKobayashiFNishiharaMChronic pain in the Japanese community – prevalence, characteristics and impact on quality of lifePLoS One2015106e012926226076135
- BreivikHCollettBVentafriddaVCohenRGallacherDSurvey of chronic pain in Europe: prevalence, impact on daily life, and treatmentEur J Pain200610428733316095934
- HendersonJVHarrisonCMBrittHCBayramCFMillerGCPrevalence, causes, severity, impact, and management of chronic pain in Australian general practice patientsPain Med20131491346136123855874
- ChungJWWongTKPrevalence of pain in a community populationPain Med20078323524217371410
- WatkinsEAWollanPCMeltonLJYawnBPA population in pain: report from the Olmsted County health studyPain Med20089216617418298699
- SchopflocherDTaenzerPJoveyRThe prevalence of chronic pain in CanadaPain Res Manag201116644545022184555
- MiróJParedesSRullMPain in older adults: a prevalence study in the mediterranean region of cataloniaEur J Pain2007111839216487733
- ElzahafRAJohnsonMITashaniOAThe epidemiology of chronic pain in Libya: a cross-sectional telephone surveyBMC Public Health201616177627514513
- ChrubasikSJunckHZappeHAStutzkeOA survey on pain complaints and health care utilization in a German population sampleEur J Anaesthesiol19981543974089699096
- Rapo-PylkköSHaanpääMLiiraHChronic pain among community-dwelling elderly: a population-based clinical studyScand J Prim Health Care201634215916427065337
- DurejaGPJainPNShettyNPrevalence of chronic pain, impact on daily life, and treatment practices in IndiaPain Practice2014142E51E6224304963
- SakakibaraTWangZPaholpakPKosuwonWOoMKasaiYA comparison of chronic pain prevalence in Japan, Thailand, and myanmarPain Physician201316660360824284845
- RafteryMNSarmaKMurphyAWDe La HarpeDNormandCMcGuireBEChronic pain in the Republic of Ireland – community prevalence, psychosocial profile and predictors of pain-related disability: results from the Prevalence, Impact and Cost of Chronic Pain (PRIME) study, part 1Pain201115251096110321450402
- TsangAVon KorffMLeeSCommon chronic pain conditions in developed and developing countries: gender and age differences and comorbidity with depression-anxiety disordersJ Pain200891088389118602869
- DziechciażMBalicka-AdamikLFilipRThe problem of pain in old ageAnn Agric Environ Med201313538
- GunzelmannTSchumacherJBrählerEThe prevalence of pain in the elderly German population: results of population-based studies with the Giessen Subjective Complaints List (Giessener Beschwerdebogen GBB)Schmerz2002164249254 German12192433
- TseMLeungRHoSPain and psychological well-being of older persons living in nursing homes: an exploratory study in planning patient-centred interventionJ Adv Nurs201268231232121679226
- TseMMPunSPBenzieIFPain relief strategies used by older people with chronic pain: an exploratory survey for planning patient-centred interventionJ Clin Nurs200514331532015707441
- McCarbergBHNicholsonBDToddKHPalmerTPenlesLThe impact of pain on quality of life and the unmet needs of pain management: results from pain sufferers and physicians participating in an Internet surveyAm J Ther200815431232018645331
- SmithBHElliottAMChambersWASmithWCHannafordPCPennyKThe impact of chronic pain in the communityFam Pract200118329229911356737
- LaméIEPetersMLVlaeyenJWKleefMPatijnJQuality of life in chronic pain is more associated with beliefs about pain, than with pain intensityEur J Pain200591152415629870
- CherubinoPSarzi-PuttiniPZuccaroSMLabiancaRThe management of chronic pain in important patient subgroupsClin Drug Investig201232Suppl 13544
- DukeMBottiMHunterSEffectiveness of pain management in hospital in the home programsClin J Pain201228318719421904201
- MoskovitzBLBensonCJPatelAAAnalgesic treatment for moderate-to-severe acute pain in the United States: patients’ perspectives in the Physicians Partnering Against Pain (P3) surveyJ Opioid Manag20117427728621957827
- Müller-SchwefeGHEuropean survey of chronic pain patients: results for GermanyCurr Med Res Opin201127112099210621933101
- Mędrzycka-DąbrowskaWDąbrowskiSBasińskiAProblems and barriers in ensuring effective acute and post-operative pain management–an international perspectiveAdv Clin Exp Med201524590591026768644
- MotovSMKhanANProblems and barriers of pain management in the emergency department: are we ever going to get better?J Pain Res2008251121197290
- TaylorALGostinLOPagonisKAEnsuring effective pain treatment: a national and global perspectiveJAMA20082991899118167410
- McCrackenLMEvonDKarapasETSatisfaction with treatment for chronic pain in a specialty service: preliminary prospective resultsEur J Pain20026538739312160513
- van HerkRBoerlageAAvan DijkMBaarFPTibboelDde WitRPain management in Dutch nursing homes leaves much to be desiredPain Manag Nurs2009101323919264281