
Abstract
Objective
This research aimed to assess the effectiveness of manual therapy in alleviating pain among women undergoing primary dysmenorrhea (PD).
Methods
All randomized controlled trials (RCTs) regarding manual therapy for PD were searched from online databases, spanning from their inception to July 2023. The identified literature underwent a thorough screening process, and the data were meticulously extracted and analyzed using RevMan 5.3. Subsequently, the included studies underwent Cochrane’s quality assessment and meta-analysis. The evidence obtained was then assessed using the grading of recommendations, assessment, development, and evaluation (GRADE) approach.
Results
32 RCTs, involving 2566 women were finally included for analysis. The overall quality of the concluding evidence was generally rated as low or very low. Performance bias and blind bias were found to be the main risk of bias of the included studies. In comparison to no treatment, manual therapy demonstrated a significant increase in pain relief in short-term (n=191, MD=1.30, 95% CI: 0.24~2.37). The differences in the effects of manual therapy and the placebo on pain intensity may not be statistically significant (n=255, MD=0.10, 95% CI: −0.37~0.58). In contrast to NSAIDs, manual therapy exhibited superior pain alleviation (n=507, MD=3.01, 95% CI: 1.08~4.94) and a higher effective rate (n=1029, OR=4.87, 95% CI: 3.29~7.20). Importantly, no severe adverse events were reported across all studies, indicating a relatively safe profile for manual therapy.
Conclusion
Manual therapy presented promise in effectively relieving menstrual pain with minimal adverse events in short term, outperforming both no treatment and NSAIDs. However, this conclusion is tempered by the low quality of the included RCTs, highlighting the necessity for more robust trials to validate it.
Introduction
Primary dysmenorrhea (PD) is defined as painful menstruation in the absence of pelvic pathology and is characterized by recurrent, crampy, lower abdominal pain during menstruation, affecting 50–90% of women.Citation1 Among them, 15–50% of women with moderate to severe symptoms find their daily activities, including work, school, or other activities, disrupted.Citation2 The adverse effects of PD extend beyond physical discomfort, affecting performance by reducing attention and productivity.Citation3,Citation4 The guidelines recommend the use of non-steroidal anti-inflammatory drugs (NSAIDs) as the primary therapeutic approach for PD.Citation5 Nevertheless, a subset of individuals fails to relieve their pain with NSAIDs and, instead, may experience undesirable side effects such as nausea, dyspepsia, headaches, or insomnia.Citation6
The non-pharmacological and non-invasive therapies are endorsed to manage dysmenorrhea symptoms, including acupuncture, biofeedback, heat treatments, transcutaneous electrical nerve stimulation, exercises, and manual therapy.Citation7,Citation8 Manual therapy, a specialized branch of physical therapy, employing skilled hands-on techniques to assess, diagnose, and treat musculoskeletal and neuromuscular conditions. This therapeutic approach encompasses a variety of hands-on techniques, including massage, acupressure, holographic therapy, spinal manipulative therapy and more.
The utilization of manual treatment for PD remains controversial. Manual therapy, either in isolation or in combination with other treatment modalities, has demonstrated potential advantages for overall health with a low reported risk of adverse effects.Citation9 In contrast, in 2006, a Cochrane systematic review indicated inadequate evidence to substantiate the efficacy of manual therapy in alleviating pain for women with dysmenorrhea.Citation10 Given these divergent viewpoints, this research was to evaluate the efficacy and safety of manual therapy for PD, utilizing updated data and comparing its effects with no treatment, placebo or first-line treatment.
Methods
This meta-analysis adhered to the guidelines outlined in the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines (Table S1).Citation11 The study protocol was registered in the PROSPERO database (https://www.crd.york.ac.uk/PROSPERO/; registration number CRD42023443160) and fully conducted in this research.
Search Strategy
A thorough search was conducted across multiple databases, including PubMed, EMBASE, MEDLINE, Cochrane Central Register of Controlled Clinical Trials, CNKI, Wanfang, SinoMed, and VIP, covering the period from inception to July 2023. The search strategy employed a combination of medical subject headings (MeSH) terms with free words such as dysmenorrhea, menstrual pain, massage, manipulation, manual therapy, and was adjusted based on the specific requirements of each database (Table S2).
Eligibility Criteria
Types of Participants
The inclusion criteria included female patients of reproductive age who were experiencing PD. PD was defined as cyclic pelvic pain occurring during menstruation without the presence of gynecological pathologies such as endometriosis, adenomyosis, or uterine myoma. Furthermore, patients with secondary dysmenorrhea or significant medical conditions were excluded.
Types of Studies
All randomized controlled trials (RCTs) assessing pain intensity and associated outcomes were systematically included to evaluate the efficacy of manual therapy in females with PD. The treatment duration spanned a minimum of 2 menstrual cycles.
Types of Interventions
In this research, the intervention group comprised various forms of manual therapies, while combinations of manual therapy with other interventions were excluded. The control group encompassed sham or placebo treatments, no treatment, and oral NSAIDs.
Types of Outcomes
The primary outcome measures were centered on a direct assessment of pain intensity or severity, utilizing assessment tools such as the Visual Analogue Scale (VAS) or Numeric Rating Scale (NRS) and McGill Pain Questionnaire (MPQ). The secondary outcomes included the Moos Menstrual Distress (MDQ) questionnaire, adverse events, and the effective rate. The effective rate was determined by applying specific evaluation criteria, including the improvement in clinical symptoms or other measurable outcomes. Participants were classified as “cured”, “significantly improved”, “improved”, or “non-responders” following therapy. The effective rate was computed using the following formula: , where N, N1, N2, and N3 represent the total sample size and the number of patients who were cured, significantly improved, and improved, respectively.Citation12
Study Selection and Data Extraction
Two researchers (LX and WYH) independently conducted searches, integrating the results using NoteExpress software to eliminate duplicates and identify potentially eligible articles through a review of titles and abstracts. The full texts of the selected articles were subsequently assessed against predetermined inclusion and exclusion criteria. Data were extracted in a standardized manner, with any discrepancies resolved through consultation with a senior reviewer (YCH). The data collection form included recorded information such as the first author, publication year, sample size, age, course of PD, intervention regimen, treatment duration, and follow-up.
Quality Assessment
Two reviewers (LX and SYN) employed Cochrane Handbook of Systematic Reviews to assess the potential for bias in each included RCT.Citation13 This assessment encompassed seven items categorized by the risk of bias, with each item being assigned to one of three risk categories: low risk, unknown risk, and high risk. The evidence quality was then rated as good, moderate, low, and very low using the grading of recommended assessment development and evaluation tool (GRADEpro GDT).Citation14 If any of the following conditions were met: 1) risk of bias; 2) inconsistency; 3) indirectness; 4) imprecision; and 5) publication bias, the GRADE grading downgraded quality of each study from excellent.
Interpretation of Treatment Effects
To gauge the clinical significance of each treatment effect, a comparison was made with the minimum clinically important difference (MCID): 1.3 points for pain intensity on NRS,Citation15 10 points for MDQ,Citation16 and a 19.9% improvement for the effect rate.Citation12
Data Synthesis
The outcomes were classified into short-term (2–3 months), intermediate (3–12 months), and long-term (>12 months). In cases where multiple time frames fell within the same category, data closest to 3 months (short-term), 6 months (intermediate), and 12 months (long-term) were considered.
Meta-analysis was performed using the RevMan 5.3. Heterogeneity was assessed through I-square (I2) statistics and Cochrane Q test.Citation17 I2 < 50% statistics or P-value > 0.01 indicated a low heterogeneity. When possible, a random-effects model was adopted for meta-analysis. In cases where substantial heterogeneity was observed, sources of heterogeneity were explored through subgroup or sensitivity analysis. For dichotomous variables, odds ratios (ORs) with 95% confidence intervals (CIs) were utilized, and other binary data were converted into OR values. Continuous variables were analyzed using the Hedges’ g method and expressed as standardized mean difference (SMD) or mean difference (MD) with 95% CIs.
The findings were descriptively synthesized if there was only one relevant study or when the data were inappropriate for quantitative synthesis. To assess publication bias, a funnel plot was employed when more than ten papers were available for pooling.
Results
Study Selection
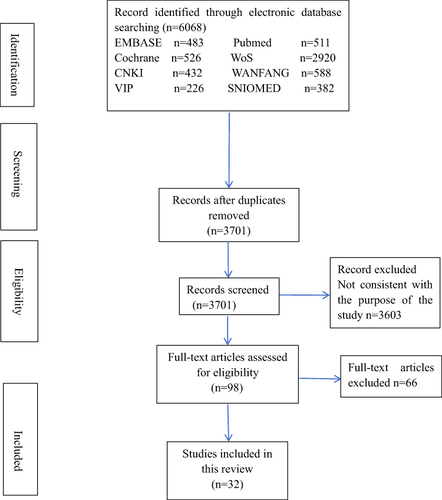
A total of 6068 citations were retrieved initially. After excluding 2367 duplicate studies, a further 3603 studies were excluded based on the screening of titles and abstracts, as they did not align with the study purpose. Subsequently, the full texts of 98 studies were carefully reviewed, and 65 were found not to meet the inclusion criteria. Finally, 32 RCTs that met the specified criteria were included in the analysis. All studies were published between January 1999 and 2019, with 18 studies published in ChineseCitation18–35 and 14 in English.Citation36–49 The PRISMA flowchart of the screening process is shown in .
Figure 1 PRISMA flowchart. Adapted from Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. J Clin Epidemiol. 2021;134:178–189. Creative Commons.Citation11
Study Characteristics
The study population comprised a total of 2566 participants who were randomly assigned to one of the 32 comparator groups. Among these, 18 studies were conducted in the Chinese mainland,Citation18–35 5 in Iran,Citation36,Citation37,Citation39,Citation40,Citation47 2 in Germany,Citation45,Citation46 3 in Taiwan,Citation41–43 and 1 each in HongKong,Citation48 America,Citation44 Italy,Citation38 and Turkey.Citation49 The age of participants ranged from 14 to 41 years, and the duration of symptoms varied from a mean of 3 months to 17 years. Across the 32 studies, manual therapy consisted various techniques, with 15 studies focusing on massage, 10 on acupressure, 2 on foot reflexology, 2 on holographic therapy, 2 on spinal manipulative therapy, and 1 on neuromuscular therapy. In the control group, 8 studies employed no treatment, 3 used sham therapy, and 21 involved oral medications. Details are presented in .
Table 1 Summary of Included Trials Basic Information
In terms of outcome reporting, the VAS was the most frequently utilized, with 15 studiesCitation18,Citation24,Citation28,Citation30,Citation33,Citation36–38,Citation41–44,Citation47–49 providing relevant data. Following closely, 14 studiesCitation19,Citation20,Citation22–24,Citation26,Citation27,Citation29–35 reported effect rates, all originating from China. Additionally, 4 studies,Citation22,Citation25,Citation26,Citation30 reported pain scores, 4Citation41–43,Citation48 reported outcomes using the MDQ, 3Citation21,Citation45,Citation46 mentioned outcomes using the NRS, and 2Citation40,Citation47 demonstrated outcomes using the MPQ. Adverse events were documented in two studies.Citation28,Citation45 The duration of most treatments lasted 2 to 4 menstrual cycles, with 6 studies having follow-ups of up to 6 months and one study extending to 12 months. Details are presented in .
Table 2 Summary of Included Trials’ Outcome Measures and Follow-Up Period
Risk of Bias
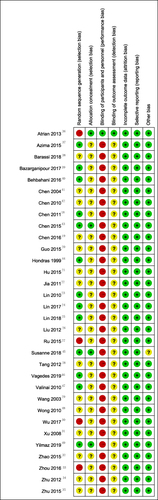
and illustrated the risk of bias observed in the included studies. Notably, in 4 studies,Citation27,Citation30,Citation33,Citation36 the randomization methods were considered to pose a high risk of bias, whereas the randomization methods were deemed appropriate in 13 studies.Citation18,Citation23–25,Citation37,Citation39,Citation40,Citation43–47,Citation49 Additionally, 15 studiesCitation19–22,Citation26,Citation28,Citation29,Citation31,Citation32,Citation34,Citation35,Citation38,Citation41,Citation42,Citation48 did not provide specific details regarding the generation of random sequences. Allocation concealment was implemented in 4 studies.Citation36,Citation43,Citation45,Citation49 Except for 1 studyCitation36 reporting blinding of participants, the remaining studiesCitation18–20,Citation22–27,Citation31,Citation33–35,Citation44–46,Citation21,Citation28–30,Citation32,Citation37–43,Citation48,Citation49,Citation47 did not furnish information on blinding. Notably, details of missing data were not reported in any of the enrolled studies, suggesting an absence of selective reporting bias. With the exception of 1 studyCitation28 with uncertainty, all other studiesCitation18–27,Citation31,Citation33–46,Citation29,Citation30,Citation32,Citation47–49 did not exhibit any other biases.
Figure 2 Risk of bias graph: review of the authors’ judgments regarding each risk of bias item presented as percentages across all included studies.
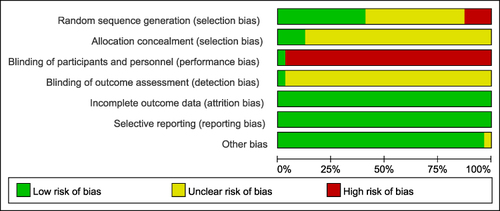
Figure 3 Risk of bias summary: review of the authors’ judgments regarding each risk of bias item in each included study.
Data Synthesis
Manual Therapy versus No Treatment
Pain Intensity
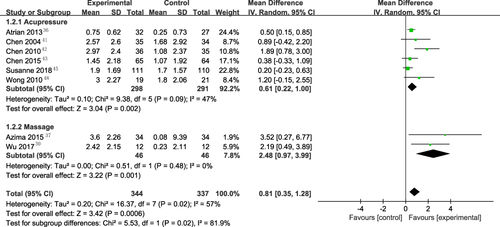
To synthesize pain scores, a meta-analysis was conducted, incorporating 8 studies.Citation30,Citation36,Citation37,Citation41–43,Citation45,Citation48 The pooled data exhibited significant heterogeneity (I2=57%), as depicted in . In the short term (n=191, MD=1.30, 95% CI: 0.24~2.37), manual therapy was preferred over no treatment by subgroup analysis; however, this effect was not seen in the intermediate term (n=361, MD=0.91, 95% CI: −0.18~1.99) or long term (n=129, MD=0.33, 95% CI: −0.33~1.09). Another subgroup analyses revealed that both acupressure (n=589, MD=0.61, 95% CI: 0.22~1.00) and massage (n=92, MD=2.48, 95% CI: 0.92~3.99) were superior to no treatment group, as depicted in .
Figure 4 Overall and different follow-up times subgroup forest plot of weighted mean difference (95% CI) for pain intensity for manual therapy versus no treatment.
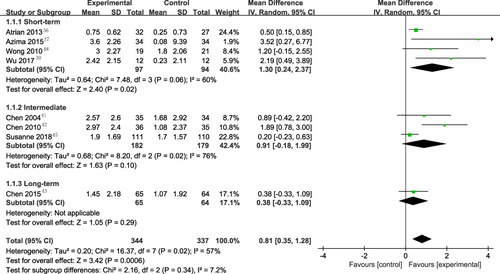
Figure 5 Overall and various manual therapies subgroup forest plot of weighted mean difference (95% CI) for pain intensity for manual therapy versus no treatment.
Effective Rate
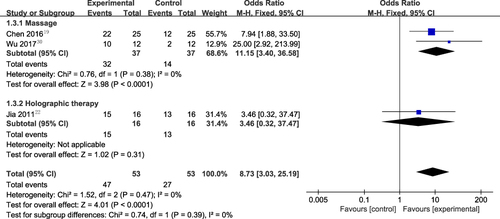
3 studiesCitation19,Citation22,Citation30 reported that the short-term effective rate in the manual therapy group was significantly higher than that in the no treatment control group (n=106, OR=8.73, 95% CI: 3.03~25.19), with no observed heterogeneity (I2=0), as illustrated in . A subgroup analysis showed that, in terms of improving effective rate, massage was superior to no treatment (n=74, OR=11.15, 95% CI: 3.40~36.58), but holographic therapy was not as beneficial (n=32, OR=3.46, 95% CI: 0.32~37.47).
Figure 6 Overall and various manual therapies subgroup forest plot of weighted OR (95% CI) for effective rate for manual therapy versus no treatment.
MDQ
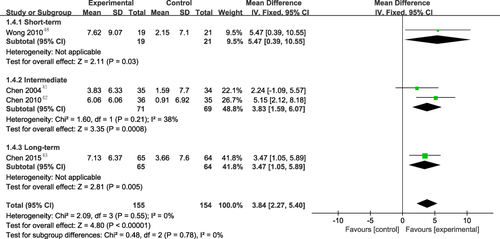
Additionally, 4 studiesCitation41–43,Citation48 reported MDQ scores. The results indicated that acupressure can lead to a greater reduction in MDQ scores compared to no treatment (n=309, MD=3.84, 95% CI: 2.27~5.40), as depicted in . The subgroup analysis demonstrated that the benefit might extend from short-term, intermediate to long- term.
Figure 7 Overall and different follow-up times subgroup forest plot of weighted mean difference (95% CI) for MDQ for manual therapy versus no treatment.
Manual Therapy versus Placebo
Pain Intensity
3 studiesCitation39,Citation44,Citation49 comparing manual therapy to a placebo reported outcomes related to pain, suggested that the differences in the effects of manual therapy and the placebo on pain may not be statistically significant in short term (n=255, MD=0.01, 95% CI: −0.37~0.58), as depicted in . The interventions in these three studies were acupressure, spinal manipulative therapy, and foot reflexology. The meta-analysis results are consistent with the findings of the original studies but lack clinical significance.
Figure 8 Forest plot of weighted mean difference (95% CI) for pain intensity for manual therapy versus place control.

Manual Therapy versus NSAIDs
Pain Intensity
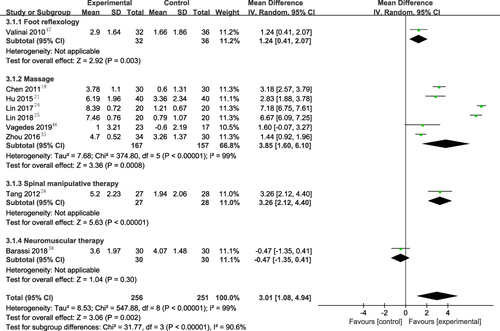
A total of 9 studiesCitation18,Citation21,Citation24,Citation25,Citation28,Citation33,Citation38,Citation46,Citation47 were subjected to meta-analysis to synthesize pain intensity findings between manual therapy and NSAIDs. Due to substantial heterogeneity (I2=99%), subgroup analyses were performed based on different types of manual therapy. As illustrated in , 1 studyCitation47 suggested that foot reflexology might yield greater pain relief than NSAIDs (n=68, MD=1.24, 95% CI: 0.41~2.07), although the difference did not attain statistical significance. 6 studiesCitation18,Citation21,Citation24,Citation25,Citation33,Citation46 indicated that massage therapy proved more effective in alleviating pain compared to NSAIDs (n=324, MD=3.85, 95% CI: 1.60~6.10). Furthermore, 1 studyCitation28 reported that the spinal manipulative therapy could potentially offer superior pain relief compared to NSAIDs (n=55, MD=3.26, 95% CI: 2.21~4.40). Conversely, another studyCitation38 found that Neuromuscular therapy demonstrated no remarkable difference in pain relief in comparison to NSAIDs (n=60, MD=−0.47, 95% CI: −1.35~0.41).
Figure 9 Overall and various manual therapies subgroup forest plot of weighted mean difference (95% CI) for pain intensity for manual therapy versus NSAIDs.
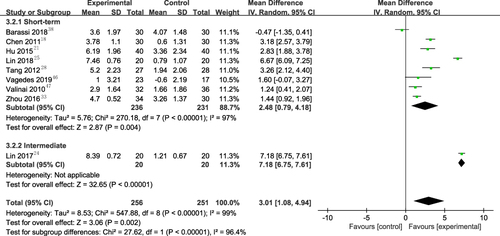
Subgroup analysis based on different follow-up durations reveals that manual therapy, in both short-term (n=467, MD=2.48, 95% CI: 0.79~4.18) and intermediate-term (n=40, MD=7.18, 95% CI: 6.75~7.61), may provide more pain relief compared to the NSAIDs group, as depicted in .
Figure 10 Overall and different follow-up times subgroup forest plot of weighted mean difference (95% CI) for pain intensity for manual therapy versus versus NSAIDs.
Effective Rate
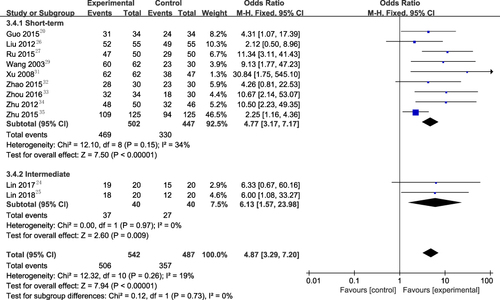
11 studiesCitation20,Citation23,Citation24,Citation26,Citation27,Citation29,Citation31,Citation33–35,Citation49 reported that the manual therapy group exhibited a significantly higher effective rate to the NSAIDs (n=1029, OR=4.87, 95% CI: 3.29~7.20), showing no heterogeneity (I2=19%). When compared to NSAIDs, the subgroup analysis revealed that acupressure, massage, and a holographic treatment are more beneficial in increasing effective rate. These findings were summarized in . Subgroup analysis based on different follow-up durations indicates that manual therapy has an advantage over NSAIDs in improving effective rate, particularly in the short-term (n=949, OR=4.77, 95% CI: 3.17~7.17) and intermediate (n=80, OR=6.13, 95% CI: 1.57~23.98), as depicted in .
Figure 11 Overall and various manual therapies subgroup forest plot of weighted OR (95% CI) for effective rate for manual therapy versus NSAIDs.
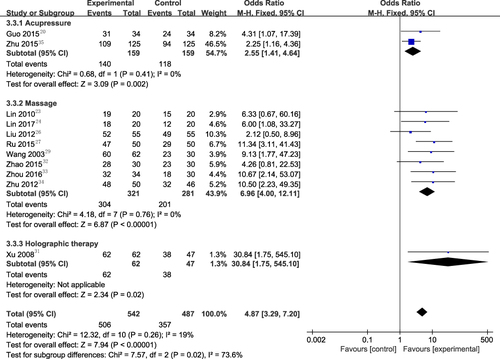
Figure 12 Overall and different follow-up times subgroup forest plot of weighted OR (95% CI) for effective rate for manual therapy versus NSAIDs.
MPQ
The reported results from the single studyCitation40 indicated a greater reduction in pain for acupressure compared to NSAIDs in short-term (n=80, MD=−6.92, 95% CI: −10.90~-2.94), which was proven by MPQ scores.
Adverse Events
Among the 32 studies analyzed, adverse events associated with the interventions were documented in only 2 studies. 1 studyCitation45 highlighted soreness in the lower back region associated with spinal manipulative therapy. In contrast, another studyCitation28 reported adverse events linked to self-acupressure, including bruises, deterioration, hand pain, pressure pain, menstrual cycle shifts, dizziness, nausea, leg pain, and finger tingling. The majority of these adverse events were considered minor, as they either resolved spontaneously or were treated effectively.
Quality of Evidence
To assess quality, GRADEpro GDT was employed, incorporating outcomes from the enrolled studies. The evidence was generally appraised as being of low or very low quality based on GRADE criteria, attributable to the elevated risk of bias and pronounced heterogeneity. Notably, self-rating scales employed as a primary outcome for pain assessment were considered low-quality evidence. The summarized findings of interventions are presented in .
Table 3 Summery of Finding
Sensitivity Analysis
Sensitivity analyses demonstrated robustness by excluding those with a sample size less than 30, or those with unclear randomization procedures (Table S3).
Publication Bias
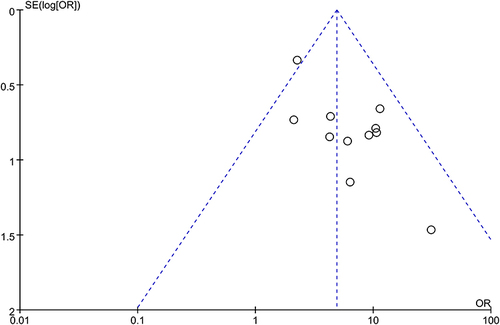
As depicted in , the likelihood of publishing bias appeared to be minimal, as indicated by the study of the funnel plot, which did not reveal any significant asymmetry. However, it is essential to approach the interpretation of funnel plot results with caution, considering inherent heterogeneity in the meta-analysis and acknowledging other potential sources of bias.
Figure 13 Funnel plot of effective rate for manual therapy versus NSAIDs.
Discussion
Summary of Main Results
We methodically examined and compiled the data from a diverse array of studies investigating manual therapy for PD in this meta-analysis. 32 studies included covered a wide variety of manual therapeutic techniques, such as massage, acupressure, foot reflexology, holographic therapy, spinal manipulative therapy, and neuromuscular therapy. By amalgamating data from these RCTs, our analysis provided a thorough overview of the effectiveness of manual therapy in addressing PD. Notably, the adverse events reported across the studies were predominantly minor in nature, with many resolving spontaneously or responding well to effective treatment.
The evidence, rated as low to very low, indicates that manual therapy for dysmenorrhea may demonstrate superior efficacy compared to both no treatment and oral NSAIDs, resulting in a more substantial alleviation of pain. These results endorse the preference for manual treatment over no treatment in patients with PD. The treatment impact estimates exceed the MCID threshold of 20%, with an effect rate of 39.1%. Nonetheless, our meta-analyses revealed that the treatment impact estimates for quality of life (MDQ, 3.84 points on a 30-to-150-point scale) and pain (NRS, 0.81 points on a 0-to-10-point scale) were marginally below thresholds of MCID thresholds among patients with PD. These results bolstered the case for utilizing manual treatment rather than oral medication in PD patients. The decrease in pain intensity by 3.01 points (95% CI: 1.08~4.94) surpassed the MCID of 2 points, while the improvement in effective rate by 19.7% (16.7~21.9) is close the MCID of 19.9%.
In studies comparing manual therapy with a placebo control (n=255, MD=0.10, 95% CI: −0.37~0.58), the results suggest that manual therapy did not exhibit superiority. Concerning this outcome, considerations arise on two fronts. Firstly, there is contemplation of the limited number of included studies and an insufficient sample size. Secondly, attention is drawn to the potential influence of the placebo effect. The placebo effect is defined as a genuine positive psychological or physiological response solely attributed to the knowledge of receiving a substance or undergoing a procedure, rather than the inherent efficacy of that substance or procedure.Citation50 This improvement is not initiated by the treatment itself but rather by the patient’s beliefs and expectations. Previous research underscores the significance of acknowledging the placebo effect in the context of physical therapy, especially when compared with placebos associated with pharmaceuticals or other intervention measures.Citation51–53
Subgroup analyses were conducted following significant heterogeneity in outcomes related to pain. In a subset characterized by a small sample size and a limited number of studies, conflicting results were observed. It is crucial to approach the interpretation of this specific subset with caution, considering its restricted representation and smaller study population, which could contribute to the observed discrepancies.
We discerned a prevalent trend of subpar research quality in the scrutinized papers, as evidenced by our comprehensive analysis of bias risk and evidence quality. The primary factor contributing to this observation is the lack of transparent data in most studies regarding the generation of random sequences and participant assignment. Furthermore, the application of blinding procedures proves challenging due to the distinctive nature of manual therapy interventions; nevertheless, a body of researchCitation36 has demonstrated the feasibility of blinding in this context. These methodological deficiencies underscore the imperative for enhanced reporting guidelines and innovative approaches to address the challenges associated with blinding and randomization in studies focusing on manual therapy interventions.
Advantages of Manual Therapy for PD
Manual therapy provides a non-pharmacological option for addressing PD, catering to individuals who prefer non-drug interventions or seek complementary approaches alongside conventional medical treatments. The personalized nature of manual therapy allows for tailored interventions with therapists adjusting techniques based on pain severity, preferences, and overall health.
The specific mechanisms underlying the efficacy of manual therapy in addressing PD are not fully understood. However, a study by Chen et alCitation54 revealed that massage therapy was beneficial for PD. Because it may relieve pain by enhancing uterine blood flow and regulating aberrant levels of prostaglandin F2a (PGF2a) and prostaglandin E2 (PGE2). Farzaneh et alCitation55 suggested that acupressure at the Sanyinjiao point (SP6) can be an effective, feasible, and cost-effective intervention for mitigating PD. The SP6 acupoint serves as the junction point of the liver, spleen, and kidney meridians. According to the traditional Chinese medicine, this intervention can strengthen the spleen function, resolve and expel dampness, and restore balance to Yin and blood, liver, and kidneys.Citation56 Furthermore, some individuals believe that manual therapy for dysmenorrhea is closely associated with reflex points. For instance, Mur et alCitation57,Citation58 reported increased intestinal blood flow during stimulation of corresponding reflex points compared to subjects intervened with reflex stimulation on unrelated points. Similarly, Sudmeier et alCitation59 demonstrated increased renal blood flow, measured with Doppler sonography, with reflexology on foot points related to the kidney compared with individuals given placebo reflexology at points not associated with the kidney.
Strengths and Limitations
Prior to this research, a systematic reviewCitation60 evaluated the effect of manual therapy for PD, incorporating four studies published in 2017. In contrast to this earlier review, our study involved a more comprehensive search strategy, encompassing a greater number of studies meeting the criteria. Meanwhile, different analytical methods were employed herein. Our research aimed to extensively explore various manual therapy modalities and considered the cyclical nature of dysmenorrhea. Additionally, we defined a minimum treatment duration of at least two months, acknowledging the periodicity of menstrual pain. The control group exclusively comprised placebos and NSAIDs. This design, with a placebo control, facilitates the evaluation of the specific effects of manual therapy. Additionally, the comparison of manual therapy with NSAIDs offers insights into the relative effectiveness and potential advantages of manual therapy over standard pharmacological interventions.
This research was subjected to several limitations. Firstly, the included studies were of low quality, restricting the availability of high-quality evidence supporting the efficacy of manual therapy in treating dysmenorrhea. Secondly, various manual therapy modalities were not classified and quantified when assessing the overall effectiveness due to their diverse range. Lastly, despite conducting subgroup analyses to address significant heterogeneity observed in the meta-analysis, the issue persisted without resolution.
Implications for Clinical Practice and Research
In clinical practice, the findings underscored the potential efficacy of manual therapy in alleviating menstrual pain. Healthcare practitioners may contemplate incorporating manual therapy into their treatment protocols for individuals experiencing PD. From a research perspective, this research highlights the necessity for further investigating distinct manual therapy modalities and their comparative efficacy. Future research endeavors should strive to enhance the quality of evidence based on high-quality studies with rigorous methodologies. Additionally, exploring the mechanisms behind the effects of manual therapy on dysmenorrhea could contribute valuable insights to the field.
Conclusion
The results in this work suggested that manual therapy might alleviate menstrual pain in short-term, surpassing both no treatment and NSAIDs. However, it is impossible to rule off an effective placebo effect during manual therapy. Manual therapy demonstrated only mild adverse events, indicating a relatively safe profile. It’s important to note that our study recommendations are constrained by limitations stemming from the low quality of the included RCTs. More rigorously designed trials are imperative to validate and confirm our findings.
Abbreviations
RCTs, randomized controlled trials; PD, primary dysmenorrhea; GRADE, grading of recommendations, assessment, development, and evaluation; NSAIDs, non-steroidal anti-inflammatory drugs; PRISMA, Preferred Reporting Items for Systematic Review and Meta-Analyses; MeSH, medical subject headings; VAS, Visual Analogue Scale; NRS, Numeric Rating Scale; MPQ, McGill Pain Questionnaire; MDQ, Moos Menstrual Distress questionnaire; MCID, minimum clinically important difference; ORs, odds ratios; CIs, confidence intervals; SMD, standardized mean difference; MD, mean difference.
Ethics Approval
This article does not contain any studies with human or animal subjects performed by any of the authors.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
Additional information
Funding
References
- Kho KA, Shields JK. Diagnosis and management of primary dysmenorrhea. JAMA. 2020;323(3):268. doi:10.1001/jama.2019.16921
- Ju H, Jones M, Mishra G. The prevalence and risk factors of dysmenorrhea. Epidemiol Rev. 2014;36(1):104–113. doi:10.1093/epirev/mxt009
- Schoep ME, Adang EMM, Maas JWM, De Bie B, Aarts JWM, Nieboer TE. Productivity loss due to menstruation-related symptoms: a nationwide cross-sectional survey among 32 748 women. BMJ Open. 2019;9(6):e026186. doi:10.1136/bmjopen-2018-026186
- MacGregor B, Allaire C, Bedaiwy MA, Yong PJ, Bougie O. Disease burden of dysmenorrhea: impact on life course potential. Int J Womens Health. 2023;15:499–509. doi:10.2147/IJWH.S380006
- Ferries-Rowe E, Corey E, Archer JS. Primary dysmenorrhea: diagnosis and therapy. Obstetrics Gynecol. 2020;136(5):1047–1058. doi:10.1097/AOG.0000000000004096
- Marjoribanks J, Ayeleke RO, Farquhar C, Proctor M; Cochrane Gynaecology and Fertility Group. Nonsteroidal anti-inflammatory drugs for dysmenorrhoea. Cochrane Database Syst Rev. 2015. doi:10.1002/14651858.CD001751.pub3
- Nesrin Y, Nesrin Y, Orcin TA, Tuba CA, Ozlem KC. Long-term follow-up result of connective tissue manipulation in young women with primary dysmenorrhea: different intervention durations. Reprod Sci. 2023;30(7). doi:10.1007/s43032-023-01172-5
- Fernández-Martínez E, Onieva-Zafra MD, Parra-Fernández ML. The impact of dysmenorrhea on quality of life among Spanish Female University students. Int J Environ Res Public Health. 2019;16(5):713. doi:10.3390/ijerph16050713
- López-Liria R, Torres-álamo L, Vega-Ramírez FA, et al. Efficacy of physiotherapy treatment in primary dysmenorrhea: a systematic review and meta-analysis. Int J Environ Res Public Health. 2021;18(15):7832. doi:10.3390/ijerph18157832
- Proctor ML, Hing W, Johnson TC, Murphy PA. Spinal manipulation for primary and secondary dysmenorrhoea. Cochrane Database Syst Rev. 2006;2006(3):CD002119. doi:10.1002/14651858.CD002119.pub3
- Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. J Clin Epidemiol. 2021;134:178–189. doi:10.1016/j.jclinepi.2021.03.001
- Xu Y, Zhao W, Li T, et al. Effects of acupoint-stimulation for the treatment of primary dysmenorrhoea compared with NSAIDs: a systematic review and meta-analysis of 19 RCTs. BMC Complement Altern Med. 2017;17:436. doi:10.1186/s12906-017-1924-8
- Cochrane handbook for systematic reviews of interventions. Available from: https://training.cochrane.org/handbook/current. Accessed December 26, 2023.
- Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924–926. doi:10.1136/bmj.39489.470347.AD
- Gallagher EJ, Liebman M, Bijur PE. Prospective validation of clinically important changes in pain severity measured on a visual analog scale. Ann Emerg Med. 2001;38(6):633–638. doi:10.1067/mem.2001.118863
- Moos RH. The development of a menstrual distress questionnaire. Psychosom Med. 1968;30(6):853–867. doi:10.1097/00006842-196811000-00006
- Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–560. doi:10.1136/bmj.327.7414.557
- Chen Y, Shang GD, Fu GB, et al. Effects of massage on uterine artery hemodynamic parameters and serum prostaglandins in patients with primary dysmenorrhea. Chi J Integrat Trad Chin Western Med. 2011;31(10):1355–1358.
- Chen XY, Ma YT, Li P, et al. Clinical observation on the effect of Wentong manipulation combined with acupoint massage on primary dysmenorrhea. Health Today. 2016;15(7):327–328.
- Guo DM. Observation and nursing of acupoint massage in relieving primary dysmenorrhea. J Ration Use Drugs Clin Pract. 2015;8(11):135–136.
- Hu L. Clinical observation on 40 cases of dysmenorrhea treated by massage. Chin Natl Folk Med. 2015;24(6):74.
- Jia Q. Application of Second Metacarpal Side Holotherapy in the Treatment of Dysmenorrhea in Female College Students [ Dissertation]. China: Shandong Sport University; 2011.
- Lin HQ. Clinical observation of treatment of primary dysmenorrhea with massage. Massage Rehabilitat Med. 2010;1:37–38.
- Lin XH, Yu L, Zhou J, et al. Study on the therapeutic effect of massage on sports dysmenorrhea in college entrance examination girls. J Anhui Normal Univ. 2017;40(04):404–408.
- Lin XH. Study on the Effect of Massage Therapy on Female College Students with Primary Dysmenorrhea [ Dissertation]. China: Anhui Normal University; 2018.
- Liu Y. Clinical observation of manual treatment of primary dysmenorrhea. China TCM Emergency. 2012;21(01):137–138.
- Ru YJ, Zheng XY. Clinical effect of massage in the treatment of primary dysmenorrhea. Prim Med China. 2015;12:1890–1891.
- Tang N. Clinical Observation of Immediate Analgesic Effect of Chiropractic Therapy on Patients with Blood Stasis Type Primary Dysmenorrhea [ Dissertation]. China: Shandong University of Traditional Chinese Medicine; 2012.
- Wang HL, Feng YH. Treatment of 62 cases of primary dysmenorrhea with tuina. Shanghai J TCM. 2003;04:34–35.
- Wu DY. Effect of “Dysmenorrhea Regulating Manipulation” on Female College Students with Primary Dysmenorrhea [ Dissertation]. Beijing Sport University; 2017.
- Xu YQ, Qiao GS. Holographic therapy for primary dysmenorrhea. Chin Commun Phys Med Spec. 2008;10(23):156.
- Zhao J, Wang JH. Thirty cases of primary dysmenorrhea were treated by syndrome differentiation and tuina. Chin J Exter Treat TCM. 2015;2015:288–291.
- Zhou Y, Dong SQ. To observe the effect of Chinese medicine manipulation in the treatment of 64 patients with dysmenorrhea. Mater Child Health China. 2016;31(24):5511–5512.
- Zhu JL. The experience of massage combined with ibuprofen in the treatment of primary dysmenorrhea in female vocational school. Med Innovat China. 2012;9(2):105–106.
- Zhu ZQ. Effect of point massage combined with nursing intervention on primary dysmenorrhea. Med Inf. 2015;10:89–90.
- Atrian MK, Abbaszadeh F, Sarvieh M, Sarafraz N, Jafarabadi MA. Investigating the effect of pressure on third liver point on primary dysmenorrhea: a randomized controlled clinical trial. Iranian Red Crescent Med J. 2013;15(9):848–853. doi:10.5812/ircmj.12719
- Azima S, Bakhshayesh HR, Kaviani M, Abbasnia K, Sayadi M. Comparison of the effect of massage therapy and isometric exercises on primary dysmenorrhea: a randomized controlled clinical trial. J Pediatr Adolesc Gynecol. 2015;28(6):486–491. doi:10.1016/j.jpag.2015.02.003
- Barassi G, Bellomo RG, Porreca A, Di Felice PA, Prosperi L, Saggini R. Somato-visceral effects in the treatment of dysmenorrhea: neuromuscular manual therapy and standard pharmacological treatment. J Alternat Complement Med. 2018;24(3):291–299. doi:10.1089/acm.2017.0182
- Bazarganipour F, Taghavi SA, Allan H, et al. A randomized controlled clinical trial evaluating quality of life when using a simple acupressure protocol in women with primary dysmenorrhea. Complementary Ther Med. 2017;34:10–15. doi:10.1016/j.ctim.2017.07.004
- Behbahani BM, Ansaripour L, Akbarzadeh M, Zare N, Hadianfard MJ. Comparison of the effects of acupressure and self-care behaviors training on the intensity of primary dysmenorrhea based on McGill pain questionnaire among Shiraz University students. J Res Med Sci. 2016;21. doi:10.4103/1735-1995.193176
- Chen HM, Chen CH. Effects of acupressure at the Sanyinjiao point on primary dysmenorrhoea. J Adv Nurs. 2004;48(4):380–387. doi:10.1111/j.1365-2648.2004.03236.x
- Chen HM, Chen CH. Effects of acupressure on menstrual distress in adolescent girls: a comparison between Hegu-Sanyinjiao matched points and Hegu, Zusanli single point. J Clin Nurs. 2010;19(7–8):998–1007. doi:10.1111/j.1365-2702.2009.02872.x
- Chen HM, Wang HH, Chiu MH, Hu HM. Effects of acupressure on menstrual distress and low back pain in dysmenorrheic young adult women: an experimental study. Pain Manag Nurs. 2015;16(3):188–197. doi:10.1016/j.pmn.2014.06.002
- Hondras MA, Long CR, Brennan PC. Spinal manipulative therapy versus a low force mimic maneuver for women with primary dysmenorrhea: a randomized, observer-blinded, clinical trial. Pain. 1999;81(1–2):105–114. doi:10.1016/S0304-3959(99)00004-4
- Blödt S, Pach D, Eisenhart-Rothe SV, et al. Effectiveness of app-based self-acupressure for women with menstrual pain compared to usual care: a randomized pragmatic trial. Am J Clin Exp Obstet Gynecol. 2018;218(2):227.e1–227.e9. doi:10.1016/j.ajog.2017.11.570
- Vagedes J, Fazeli A, Boening A, Helmert E, Berger B, Martin D. Efficacy of rhythmical massage in comparison to heart rate variability biofeedback in patients with dysmenorrhea—A randomized, controlled trial. Complementary Ther Med. 2019;42:438–444. doi:10.1016/j.ctim.2018.11.009
- Valiani M, Babaei E, Heshmat R, Zare Z. Comparing the effects of reflexology methods and Ibuprofen administration on dysmenorrhea in female students of Isfahan University of Medical Sciences. Iran J Nurs Midwifery Res. 2010;15(Suppl 1):371–378.
- Wong CL, Lai KY, Tse HM. Effects of SP6 acupressure on pain and menstrual distress in young women with dysmenorrhea. Complement Ther Clin Pract. 2010;16(2):64–69. doi:10.1016/j.ctcp.2009.10.002
- Yilmaz FA, Baser M. Effects of foot reflexology on dysmenorrhea: a randomized controlled trial. Cukurova Med J. 2019;44:54–60. doi:10.17826/cumj.550663
- Stewart-Williams S, Podd J. The placebo effect: dissolving the expectancy versus conditioning debate. Psychol Bull. 2004;130(2):324–340. doi:10.1037/0033-2909.130.2.324
- Linde K, Niemann K, Meissner K. Are sham acupuncture interventions more effective than (other) placebos? A re-analysis of data from the Cochrane review on placebo effects. Forsch Komplementmed. 2010;17(5):259–264. doi:10.1159/000320374
- Sun CY, Xiong ZY, Sun CY, et al. Placebo response of sham acupuncture in patients with primary dysmenorrhea: a meta-analysis. J Integr Med. 2023;21(5):455–463. doi:10.1016/j.joim.2023.08.005
- Molina-Álvarez M, Arribas-Romano A, Rodríguez-Rivera C, et al. Manual therapy effect in placebo-controlled trials: a systematic review and meta-analysis. Int J Environ Res Public Health. 2022;19(21). doi:10.3390/ijerph192114021
- Chen Y, Shang G-D, Fu G-B. 推拿对原发性痛经患者子宫动脉血流动力学参数及血清前列腺素的影响 [Effect of massage on hemodynamics parameters of uterine artery and serum prostaglandin in treating patients with primary dysmenorrhea]. Chinese Journal of Integrative Medicine. 2011;31(10):1355–1358. Chinese.
- Kashefi F, Ziyadlou S, Khajehei M, Ashraf AR, Reza Fadaee A, Jafari P. Effect of acupressure at the Sanyinjiao point on primary dysmenorrhea: a randomized controlled trial. Complement Therap Clin Pract. 2010;16(4):198–202. doi:10.1016/j.ctcp.2010.04.003
- Abaraogu UO, Igwe SE, Tabansi-Ochiogu CS. Effectiveness of SP6 (Sanyinjiao) acupressure for relief of primary dysmenorrhea symptoms: a systematic review with meta- and sensitivity analyses. Complement Therap Clin Pract. 2016;25:92–105. doi:10.1016/j.ctcp.2016.09.003
- Mur E, et al. Influence of reflex zone therapy of the feet on intestinal blood flow measured by color doppler sonography. Forsch Komplementarmed Klass Naturheilkd. 2001;8:86–89.
- Demirtürk F, Yilar Erkek Z, Alparslan Ö, Demirtürk F, Demir O, Inanir A. Comparison of reflexology and connective tissue manipulation in participants with primary dysmenorrhea. J Altern Complementary Med. 2016;22(1):38–44. doi:10.1089/acm.2015.0050
- Sudmeier I, Bodner G, Egger I, Mur E, Ulmer H, Herold M. Ønderung der Nierendurchblutung durch organ assoziierte Reflexzonentherapie am Fuss ge messen mit farbkodierter Doppler-Sonograp [Changes of renal blood flow during organ-associated foot reflexology measured by color Doppler sonography]. Forsch Komplementarmed. 1999;6(3):129–134. German. doi:10.1159/000021238
- Abaraogu UO, Igwe SE, Tabansi-Ochiogu CS, Duru DO. A systematic review and meta-analysis of the efficacy of manipulative therapy in women with primary dysmenorrhea. Explore. 2017;13(6):386–392. doi:10.1016/j.explore.2017.08.001