
Abstract
Purpose
Diabetes mellitus (DM) causes different corneal changes that are associated with the severity of diabetic retinopathy. To identify the pathophysiological reasons for this, corneal tomography and optical densitometry (COD) were combined with retinal oximetry.
Methods
Patients with DM and healthy subjects were included in this pilot study. Spatially resolved corneal thickness and COD were assessed using the Pentacam HR (Oculus). The pachymetry difference (PACDiff) was calculated as an indicator of an increase in the peripheral corneal thickness. Oxygen saturation (SO2) of the retinal vessels was measured using the Retinal Vessel Analyzer (Imedos Systems UG). Subsequently, the associations between corneal and retinal parameters were analyzed.
Results
Data from 30 patients with DM were compared with those from 30 age-matched healthy subjects. In DM, arterial (P = 0.048) and venous (P < 0.001) SO2 levels were increased, and arteriovenous SO2 difference was decreased (P < 0.001). In patients, PACDiff was higher than that in healthy subjects (P < 0.05), indicating a stronger increase in peripheral corneal thickness. The COD was reduced in DM (P = 0.004). The PACDiff of concentric rings with a diameter of 4 mm (r = −0.404; P = 0.033) to 8 mm (r = −0.522; P = 0.004) was inversely correlated with the arteriovenous SO2 difference. Furthermore, PACDiff 4 mm was negatively associated with arterial SO2 (r = −0.389; P = 0.041), and the COD of the peripheral corneal areas correlated positive with arterial SO2 (COD total 10–12 mm: r = 0.408; P = 0.025).
Conclusion
These associations might indicate a common pathogenesis of corneal and retinal changes in DM, which could be caused by reduced oxygen supply, mitochondrial dysfunction, oxidative stress, and cytokine effects.
Plain Language Summary
Retinal changes are particularly important for ophthalmologists in the management of diabetes mellitus. These are primarily consequences of diabetic vascular changes that can lead to a lack of oxygen. However, there is also evidence of significant changes in the cornea of patients with diabetes. In the present study, the associations between changes in corneal thickness profile, optical density of the cornea, and oxygen saturation of retinal vessels in diabetes mellitus were demonstrated for the first time. Therefore, this study could contribute to clarifying the possible causes of corneal changes in patients with diabetes.
Introduction
Chronic hyperglycemia induces morphological and functional changes in various organ systems of the human body. In addition to acute metabolic complications, the course of the disease is determined by the chronic vascular changes.Citation1 In the eye, the consequences of retinal microangiopathy (diabetic retinopathy (dRP) and maculopathy (dMP)) are most significant.Citation2 In addition to the damage, particularly to small blood vessels, caused by the high blood sugar level, direct hyperglycemic effects on the retinal cells probably also play a role.Citation2 Furthermore, there is increasing evidence that DM affects corneal microstructure and function.Citation3 In patients with DM, the incidence of ocular surface diseases has increased.Citation2,Citation4 Potential reasons include reduction in corneal innervation, changes in tear film composition, and epithelial cells with an accumulation of advanced glycation end-products (AGEs). Furthermore, disturbed corneal barrier function and delayed wound healing are conceivable.Citation3,Citation4 Changes in growth factor concentrations, cytokine levels, oxidative stress, changes in corneal proteoglycans and glycosaminoglycans, and inflammatory components may be associated.Citation3–5
Degeneration of neuronal fibers with a reduction in corneal sensitivity has been reported, which correlates with the stage of dRP.Citation6 Furthermore, cellular changes, with a reduction in epithelial cell density, were present in DM.Citation7 In addition, keratocyte lossCitation8 and reduction in endothelial cellsCitation9 are associated with disease duration and HbA1C values. Different studies have reported an increase in central corneal thickness (CCT) in DM.Citation9–11 The rise in CCT is associated with the severity of peripheral neuropathy,Citation10 disease duration,Citation9 and the stage of dRP.Citation11 Furthermore, changes in the peripheral corneal thickness profile are associated with the stage of dRP and presence of dMP.Citation12 However, hyperglycemia-induced changes in the corneal stroma are hardly known.Citation3 The stroma accounts for approximately 90% of the whole corneal volumeCitation2 and mainly determines corneal biomechanical properties.Citation3,Citation4 In this context, corneal biomechanics are also altered in DMCitation5,Citation13 and these changes correlate with the stage of dRP and presence of dMP as well.Citation13 Furthermore, an increase in corneal autofluorescenceCitation14 and a reduction in corneal optical densityCitation15 were detectable, which also showed significant associations with the severity of dRP.Citation14,Citation15
These associations lead to the assumption of a common pathogenesis for corneal and retinal changes in DM. Earlier studies using retinal oximetry revealed an increase in oxygen saturation (SO2) of the retinal arterioles and venules. This increase in SO2 was associated with indicators of disease severity and the dRP.Citation16 In this context, the fundus of the eye offers an unique opportunity to directly visualize blood vessels and to measure tissue perfusion parameters. Furthermore, the arterial supply of the whole eye originates mainly from a common source: the ophthalmic artery. It is well known, that the stage of dRP is an indicator of the systemic microvascular stage and the risk of complications in DM. This may also be the case for hyperglycemia-induced corneal changes.Citation3
To test the hypothesis of a common pathogenesis of corneal and retinal changes in DM, measurements of corneal parameters and retinal oximetry were combined in the current pilot study.
Methods
This study adhered to the tenets of the Declaration of Helsinki and the local ethics committee of the University Hospital approved the study protocol. Adult patients with DM between October 2018 and April 2020 were included in this pilot study. In patients, the DM type, disease duration, antidiabetic therapy, and current HbA1c levels were assessed. The data were compared with those of age-matched healthy subjects. Only one eye randomly chosen from each participant was included in the study. Exclusion criteria were pre-existing corneal diseases, glaucoma, trauma, ocular surgery in the past (except for uncomplicated intravitreal injections), previous retinal vessel occlusion, and retinal diseases other than diabetic retinopathy or maculopathy. Data of participants with previous myocardial infarction, bypass operation, stroke, or peripheral artery occlusive disease were excluded because of their potential influence on retinal oximetry. All study participants underwent measurements using a Retinal Vessel Analyzer (RVA; Imedos Systems UG, Jena, Germany) and Pentacam (Pentacam HR, type 70,900, Oculus, Wetzlar, Germany).
The RVA consisted of a modified fundus camera (FF450; Carl Zeiss Meditec AG, Jena, Germany) equipped with a digital camera (KY-F75; JVC, Inc., Yokohama, Japan). Thirty-degree images of the fundus centered on the optic disc were taken. The SO2 of retinal vessels was evaluated using a two-wavelength technique. By introducing a dual-bandpass transmission filter in the optical path of the camera, two images of different wavelengths (548 ± 10 nm and 610 ± 10 nm) were recorded simultaneously. For image acquisition the programs Visualis version 2.61 (Imedos Systems UG, Jena, Germany) and VesselMap version 3.10 (Imedos Systems UG, Jena, Germany) were used. The optical density of each retinal vessel was determined using the grayscale values of the images. SO2 was proportional to the ratio of the optical densities of both captured images, and the saturation of each vessel was calculated accordingly.Citation16 Vessel segments within a peripapillary annulus (inner radius of 1 and outer radius of 1.5 optic disc diameters) were analyzed, and the mean values of all arterioles and venules were calculated.
Pentacam uses a rotating Scheimpflug camera to generate two-dimensional optical sections through the cornea and the structures lying behind, and the software reconstructs three-dimensional anterior and posterior surface tomography of the cornea. Spatially resolved corneal thickness was measured as the distance between the anterior and posterior border of the cornea.Citation17 In the current study, peripheral thickness change was calculated as the difference between the thinnest corneal thickness (TCT) and the peripheral thickness value of concentric rings around the TCT. Rings with a diameter of 2–10 mm were used to calculate the PACDiff.Citation12
Furthermore, Pentacam measured the corneal backscattered light and calculated the corneal optical density (COD) over a 12-mm-diameter area centered at the apex. The examined area was further divided into four annular zones (0–2 mm, 2–6 mm, 6–10 mm, and 10–12 mm in diameter), and for each zone, COD was given in three separate layers (anterior 120 μm, central layer, and posterior 60 μm).Citation18
Data were analyzed using the SPSS software (Version 28, IBM Statistics, New York, USA). The Kolmogorov–Smirnov test was used to check for a normal distribution of the results. Because some parameters were not normally distributed, group comparisons were performed using the Mann–Whitney U-test. Associations among SO2 values, corneal thickness parameters, and COD values were examined using Spearman correlation analysis. Statistical significance was set at p ≤ 0.05.
Results
Thirty eyes of patients with DM type 2 were included in this pilot study. Mean age was 69.6 ± 11.5 years (range 47–94 years) and mean intraocular pressure amounted to 15.2 ± 4.3 mmHg. The mean disease duration was 21.1 ± 13.2 %, and the mean HbA1C value was 6.9 ± 1.4 %. Nine of the investigated eyes showed a dRP (one mild non-proliferative, four moderate non-proliferative, three non-proliferative, and one proliferative), eight patients showed a dMP with edema, and two patients had been treated by pan-retinal laser coagulation in the past. Furthermore, 13 patients had diabetic neuropathy, five had diabetic nephropathy, and seven had diabetic foot syndrome. Fourteen patients received oral antidiabetic therapy, nine were treated with insulin and seven patients received combination therapy.
SO2 of retinal arterioles (100.7 ± 6.5 % vs 97.4 ± 4.9 %, P = 0.048) and venules (69.8 ± 9.5 % vs 59 ± 6.7 %, P < 0.001) was higher in DM patients than in healthy subjects. Furthermore, the arteriovenous SO2 difference was significantly reduced in the DM (30.9 ± 7.5 % vs 38.5 ± 5.5 %, P < 0.001, ).
Table 1 Baseline Data and Oxygen Saturation Values of Retinal Vessels in Diabetes Mellitus Patients and Healthy Subjects
The analysis of spatially resolved pachymetry readings showed higher differences between peripheral corneal thickness values and TCT in patients with DM than in the controls (P < 0.05, ). This observation indicates a greater increase in the peripheral corneal thickness in patients with DM. In agreement, absolute pachymetry values of the concentric rings with a diameter of 8 mm (699.6 ± 37.9 µm vs 672.9 ± 42.6 µm, P = 0.031) and 10 mm (788.8 ± 47.6 µm vs 738.5 ± 58.1 µm, P = 0.003) were higher in patients than in healthy subjects (). Furthermore, in DM, COD was lower in most of the analyzed corneal areas and layers (total COD: 21.8 ± 6.6 GSU vs 27.3 ± 5.3 GSU, P = 0.004, ).
Table 2 Results of Pentacam Measurements in Diabetes Mellitus Patients and Healthy Subjects
In patients with DM, correlation analysis between SO2 of the retinal vessels and corneal thickness measurements revealed an inverse association between arteriovenous saturation difference and the thickness difference between the TCT and peripheral concentric rings with a diameter of 4–8 mm (PACDiff 4 mm: r = −0.404, P = 0.033; ; PACDiff 5 mm: r = −0.441, P = 0.019; PACDiff 6 mm: r = −0.474, P = 0.011; PACDiff 7 mm: r = −0.452, P = 0.016; PACDiff 8 mm: r = −0.522, P = 0.004). Furthermore, arterial SO2 inversely correlated with the difference between the TCT and peripheral ring with a diameter of 4 mm (r = −0.389, P = 0.041, ).
Figure 1 Association between oxygen saturation of retinal arterioles (in %), retinal arteriovenous saturation difference (in %), and difference between central thinnest corneal thickness and peripheral thickness of the cornea measured at a concentric ring with a diameter of 4 mm (PAC Diff 4 mm, in µm) in diabetes mellitus.
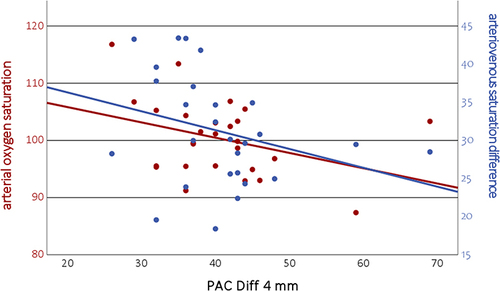
In healthy subjects, no significant association between corneal thickness and arterial or venous SO2 was detected (for example arterial SO2 and PACDiff 2 mm: r = 0.168, P = 0.376, PACDiff 4 mm: r = 0.152, P = 0.424, PACDiff 6 mm: r = 0.084, P = 0.661; venous SO2 and PACDiff 2 mm: r = −0.171, P = 0.366, PACDiff 4 mm: r = −0.155, P = 0.414, PACDiff 6 mm: r = −0.138, P = 0.469). However, the arteriovenous saturation difference weakly correlated with PACDiff 2 mm (r = 0.374, P = 0.041), PACDiff 4 mm (r = 0.408, P = 0.025) and PACDiff 6 mm (r = 0.368, p = 0.045).
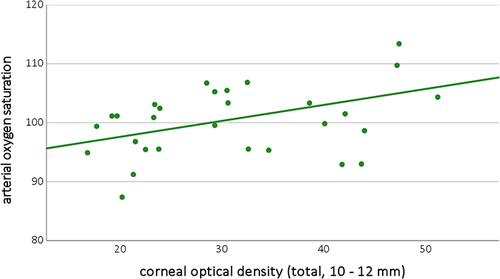
Furthermore, in DM, the COD of the peripheral corneal zones was associated with arterial SO2: COD in the 10–12 mm area of the anterior layer (r = 0.422, P = 0.02), central layer (r = 0.4, P = 0.028), and total COD of the 10–12 mm zone (r = 0.408, P = 0.025, ) correlated with arterial SO2. However, no association between COD values and venous SO2 (total COD of the 10–12 mm zone: r = 0.031, P = 0.869) or arteriovenous saturation differences (total COD of the 10–12 mm zone: r = 0.339, P = 0.067) was detected in DM. Similarly, in healthy subjects, no significant correlations were detected between COD and oxygen saturation values (total COD of the 10–12 mm zone and arterial SO2: r = 0.223, P = 0.236; venous SO2: r = 0.094, P = 0.62; arteriovenous SO2 difference: r = −0.014, P = 0.943).
Figure 2 Correlation between retinal arterial oxygen saturation (in %) and peripheral corneal optical density (of all layers at 10 to 12 mm diameter, in µm) in diabetes mellitus patients.
Discussion
Corneal Thickness Profile
In the past, not only a hyperglycemia-induced increase in CCTCitation9,Citation10 but also changes in the corneal thickness profileCitation12 were detected in DM. The observation of a stronger peripheral thickness increase in the cornea in the DMCitation12 group was confirmed in the current study. Potential reasons for the diabetic CCT increase include alterations in corneal ground substances with the accumulation of advanced glycation end products, glycosylation of proteoglycans and glycosaminoglycans, increased crosslinking of collagen fibrils,Citation5 and thickening of basal membranes.Citation19 In addition, these changes may induce an increase in the peripheral corneal thickness. Furthermore, changes in corneal hydration may be a causative factor. In addition to central endothelial changes,Citation9,Citation10 alterations in the peripheral corneal endothelium have been reported,Citation20 which may result in corneal swelling. Moreover, a healthy cornea is free of blood vessels and limbal capillaries supply only a small peripheral proportion.Citation2 Therefore, systemic hyperglycemia may influence the corneal periphery. Furthermore, the distribution pattern of proteoglycans within the cornea may also be causative.Citation21 The properties of proteoglycans depend on their glycosaminoglycan (GAG) side chains and their proportions vary within the cornea.Citation2,Citation21,Citation22 Different water-binding properties of GAGs influence corneal hydrationCitation22,Citation23 and the spatial orientation of collagen fibrils. Therefore, GAGs act as spacers between collagen fibrils and affect their orientation,Citation21 which may influence the corneal thickness profile.
Corneal Optical Density
COD was used to obtain further information on the microstructural changes in the corneal tissue. To quantify the clarity of the cornea, the backscattering of incident light during tissue passage can be measured.Citation24 Light scattering is a complex process that depends on different factors, such as the refractive indices of collagen and interfibrillar matrix, structure of collagen fibrils, and hydration of the cornea.Citation23 As previously mentioned, hydration and collagen structure are mainly determined by proteoglycans.Citation23 Therefore, changes in the proteoglycan distribution can cause deviations in COD. In the current study, COD was reduced in DM.
The stroma accounts for approximately 90% of total corneal volume.Citation2 Using in vivo confocal microscopy, Hillenaar et al showed that keratocyte nuclei are the main source of stromal backscattering of light.Citation25 Additionally, a reduction in corneal keratocytes has been reported in DM, which is associated with the disease duration and HbA1c level.Citation8 Therefore, the loss of corneal keratocytes introduced by chronic hyperglycemia may be the cause of COD reduction. Keratocytes play an essential role in the balance between proteoglycans and the degradation of metabolic products.Citation26 In cases of reduced keratocyte function, the accumulation of metabolites might introduce corneal thickening and changes in the thickness profile.
Retinal Oximetry
In DM, arterial and venous SO2 were increased and arteriovenous differences were reduced. In agreement with this, earlier studies showed an increase in SO2 of retinal vessels, which was correlated with the severity of dRP,Citation16 and vascular changes of the retina were considered indicators of systemic diabetic complications. On the one hand, a reduced oxygen delivery to the tissue may be reasonable. This could be caused by blood shunting, capillary non-perfusion, increased oxygen affinity of hemoglobin, thickening of capillary basement membranes, shortened arteriovenous passage time, and dysfunction of the vascular endothelium.Citation16 On the other hand, mitochondrial dysfunction or tissue degeneration may reduce the metabolic oxygen demand.Citation16
Association Between Corneal and Retinal Changes
Following the hypothesis of reduced oxygen release into the tissue, the retinal arteriovenous SO2 difference was reduced in DM. With increasing HbA1c levels, the oxygen affinity of hemoglobin risesCitation27 and the oxygen supply declines. This stronger oxygen affinity of hemoglobin exists not only in the retina but also in all tissues of the body. As mentioned above, the peripheral portion of the cornea is supplied by the limbal capillaries.Citation2 In addition, oxygen delivery may be suboptimal in DM. The reduced availability of oxygen might cause a reduction in the number of corneal cells as a result of apoptosis. The consequence could be keratocyte loss, leading to a reduced COD in patients with DM. In addition, few or inactive cells cannot maintain the optimal corneal condition, and changes in proteoglycan and water distribution occur. This result may be due to the changes in the corneal thickness profile. In agreement with this, in the current study, a reduction in the arteriovenous SO2 difference (indicating reduced oxygen extraction) was associated with a stronger peripheral thickness increase in DM. Furthermore, retinal arterial SO2 was positively correlated with the COD of the peripheral corneal areas in DM. A possible explanation could be that, unlike the central cornea, the peripheral tissue is mainly supplied by limbal capillaries.Citation2 As mentioned above, loss of corneal keratocytes may be the cause of COD reduction in DM.Citation8,Citation25 Therefore, assuming a systemically similar perfusion situation, on might speculate that a sufficient supply of high arterial SO2 may prevent keratocyte loss in peripheral corneal regions. However, further studies are needed to clarify whether the intake of oxygen in the corneal tissue may be diminished in diabetes or whether other causes lead to keratocyte loss.
However, there is another possible explanation for mitochondrial dysfunction. In systemic DM pathogenesis, the formation of reactive oxygen species (ROS) by dysfunctional mitochondria appears to be the primary event.Citation1,Citation28 Therefore, ROS can induce proinflammatory cytokines,Citation29 and chronic inflammation is a part of the diabetic complications.Citation1 Furthermore, AGE formation during hyperglycemia is accompanied by ROS release.Citation1 Thus, an increase in oxidative stress and ROS accumulation may be important for the development of dRP.Citation30
In addition, corneal mitochondria are affected by DM. Earlier studies have shown impaired function and altered morphology of the mitochondria of endothelial cells.Citation31 The increase in corneal autofluorescence correlated with the severity of dRP.Citation14 It may show changes in the metabolism of mitochondrial flavoproteins, which are influenced by the glucose level, oxygen supply, and respiratory state of corneal mitochondrias.Citation14
As mentioned above, ROS not only have direct damaging effects on cells and molecules, but are also able to induce proinflammatory cytokines.Citation29 Accordingly, in DM, a significant association between SO2 in retinal vessels and the concentration of proangiogenic and proinflammatory cytokines in aqueous fluid has been found.Citation32 CytokineCitation33 and AGE-induced ROS productionCitation34 can induce apoptosis in corneal cells. Therefore, it is conceivable that mitochondrial dysfunction, oxidative stress, and an increase in proinflammatory cytokines lead to malfunction and death of corneal keratocytes.Citation8 This, in turn, could lead to changes in COD and corneal thickness profile. These and similar changes probably occur not only in the cornea but also in other organs. Therefore, retinal oximetry may be an indicator of the systemic oxygen supply. This assumption is in line with previous hypotheses of systemic mitochondrial dysfunction in patients with chronic hyperglycemiaCitation1 and the common pathogenesis of corneal and retinal alterations in DM.
Limitations
This study has some limitations. It was an observational cross-sectional pilot study that showed differences and connections, but could not provide proof of causality. It is therefore just speculation about possible connections. For this reason, a longitudinal evaluation may be beneficial for identifying pathogenetic associations. Moreover, the necessary group matching reduced the number of participants, and all the patients were Caucasian. Since this was an exploratory study with limited number of cases, the p-values were not adjusted.Citation35 Consequently, the results should be cautiously interpreted. Furthermore, the study could gain from confocal microscopy. In addition, direct oximetry of limbal corneal capillaries would be desirable and could potentially be performed in a future study. However, the strength of the current study lies in the combination of the different measurement procedures in patients with DM.
Conclusion
In conclusion, in this pilot study, earlier results of changes in SO2 of retinal vessels, reduction in COD, and alterations in corneal thickness profile in DM were confirmed. The significant association between retinal SO2 values and corneal parameters may indicate the common pathogenesis of hyperglycemia-induced corneal and retinal changes. The possible mechanisms include reduced oxygen supply, mitochondrial dysfunction, oxidative stress, and cytokine effects in DM.
Data Sharing Statement
The dataset analyzed in this study is available from the corresponding author upon reasonable request.
Statement of Ethics
This study adhered to the tenets of the Declaration of Helsinki. The study protocol was approved by the Ethics Committee of the University Hospital Carl Gustav Carus, Dresden, TU Dresden, Germany (EK 424102016 and EK 91032013). Before enrolment, all participants were informed of the study purpose, methods, and data analysis, and informed consent was obtained from all participants.
Disclosure
The authors declare no conflicts of interest in this work.
References
- Forbes JM, Cooper ME. Mechanisms of diabetic complications. Physiol Rev. 2013;93(1):137–188. doi:10.1152/physrev.00045.2011
- Bowling B. Kanski`s Clinical Ophthalmology: A Systematic Approach. 8th ed. Elsevier; 2017.
- Del Buey MA, Casas P, Caramello C, et al. An update on corneal biomechanics and architecture in diabetes. J Ophthalmol. 2019;2019:7645352. doi:10.1155/2019/7645352
- Shih KC, Lam KSL, Tong L. A systematic review on the impact of diabetes mellitus on the ocular surface. Nutr Diabetes. 2017;7(3):e251. doi:10.1038/nutd.2017.4
- Scheler A, Spoerl E, Boehm AG. Effect of diabetes mellitus on corneal biomechanics and measurement of intraocular pressure. Acta Ophthalmol. 2012;90(6):e447–451. doi:10.1111/j.1755-3768.2012.02437.x
- Česká Burdová M, Kulich M, Dotřelová D, Mahelková G. Effect of diabetes mellitus type 1 diagnosis on the corneal cell densities and nerve fibers. Physiol Res. 2018;67(6):963–974. doi:10.33549/physiolres.933899
- Qu JH, Li L, Tian L, Zhang XY, Thomas R, Sun XG. Epithelial changes with corneal punctate epitheliopathy in type 2 diabetes mellitus and their correlation with time to healing. BMC Ophthalmol. 2018;18(1):1. doi:10.1186/s12886-017-0645-6
- Kalteniece A, Ferdousi M, Azmi S, Marshall A, Soran H, Malik RA. Keratocyte density is reduced and related to corneal nerve damage in diabetic neuropathy. Invest Ophthalmol Vis Sci. 2018;59(8):3584–3590. doi:10.1167/iovs.18-23889
- Calvo-Maroto AM, Cerviño A, Perez-Cambrodí RJ, García-Lázaro S, Sanchis-Gimeno JA. Quantitative corneal anatomy: evaluation of the effect of diabetes duration on the endothelial cell density and corneal thickness. Ophthalmic Physiol Opt J Br Coll Ophthalmic Opt Optom. 2015;35(3):293–298. doi:10.1111/opo.12191
- Kumar N, Pop-Busui R, Musch DC, et al. Central corneal thickness increase due to stromal thickening with diabetic peripheral neuropathy severity. Cornea. 2018;37(9):1138–1142. doi:10.1097/ICO.0000000000001668
- Jha A, Verma A, Alagorie AR. Association of severity of diabetic retinopathy with corneal endothelial and thickness changes in patients with diabetes mellitus. Eye Lond Engl. 2021. doi:10.1038/s41433-021-01606-x
- Ramm L, Spoerl E, Pillunat LE, Terai N. Is the corneal thickness profile altered in diabetes mellitus? Curr Eye Res. 2020;45(10):1228–1234. doi:10.1080/02713683.2020.1741009
- Ramm L, Herber R, Spoerl E, Pillunat LE, Terai N. Factors influencing corneal biomechanics in diabetes mellitus. Cornea. 2020;39(5):552–557. doi:10.1097/ICO.0000000000002275
- Stolwijk TR, van Best JA, Oosterhuis JA, Swart W. Corneal autofluorescence: an indicator of diabetic retinopathy. Invest Ophthalmol Vis Sci. 1992;33(1):92–97.
- Ramm L, Spoerl E, Pillunat LE, Terai N. Corneal densitometry in diabetes mellitus. Cornea. 2020;39(8):968–974. doi:10.1097/ICO.0000000000002310
- Hammer M, Vilser W, Riemer T, et al. Diabetic patients with retinopathy show increased retinal venous oxygen saturation. Graefes Arch Clin Exp Ophthalmol Albrecht Von Graefes Arch Klin Exp Ophthalmol. 2009;247(8):1025–1030. doi:10.1007/s00417-009-1078-6
- Oliveira CM, Ribeiro C, Franco S. Corneal imaging with slit-scanning and Scheimpflug imaging techniques. Clin Exp Optom. 2011;94(1):33–42. doi:10.1111/j.1444-0938.2010.00509.x
- Cankaya AB, Tekin K, Kiziltoprak H, Karahan S, Yilmazbas P. Assessment of corneal backward light scattering in the healthy cornea and factors affecting corneal transparency. Jpn J Ophthalmol. 2018;62(3):335–341. doi:10.1007/s10384-018-0584-7
- Hashemi H, Asgari S, Mehravaran S, Emamian MH, Fotouhi A. Five-year changes of anterior corneal indices in diabetics versus non-diabetics: the shahroud eye cohort study. Curr Eye Res. 2019;44(1):30–33. doi:10.1080/02713683.2018.1521977
- McNamara NA, Brand RJ, Polse KA, Bourne WM. Corneal function during normal and high serum glucose levels in diabetes. Invest Ophthalmol Vis Sci. 1998;39(1):3–17.
- Ho LTY, Harris AM, Tanioka H, et al. A comparison of glycosaminoglycan distributions, keratan sulphate sulphation patterns and collagen fibril architecture from central to peripheral regions of the bovine cornea. Matrix Biol J Int Soc Matrix Biol. 2014;38:59–68. doi:10.1016/j.matbio.2014.06.004
- Castoro JA, Bettelheim AA, Bettelheim FA. Water gradients across bovine cornea. Invest Ophthalmol Vis Sci. 1988;29(6):963–968.
- Meek KM, Leonard DW, Connon CJ, Dennis S, Khan S. Transparency, swelling and scarring in the corneal stroma. Eye Lond Engl. 2003;17(8):927–936. doi:10.1038/sj.eye.6700574
- Özyol P, Özyol E. Assessment of corneal backward light scattering in diabetic patients. Eye Contact Lens. 2018;44(Suppl 1):S92–S96. doi:10.1097/ICL.0000000000000331
- Hillenaar T, Cals RHH, Eilers PHC, Wubbels RJ, van Cleynenbreugel H, Remeijer L. Normative database for corneal backscatter analysis by in vivo confocal microscopy. Invest Ophthalmol Vis Sci. 2011;52(10):7274–7281. doi:10.1167/iovs.11-7747
- Yam GHF, Riau AK, Funderburgh ML, Mehta JS, Jhanji V. Keratocyte biology. Exp Eye Res. 2020;196:108062. doi:10.1016/j.exer.2020.108062
- Schweitzer D, Lasch A, van der Vorst S, et al. Change of retinal oxygen saturation in healthy subjects and in early stages of diabetic retinopathy during breathing of 100% oxygen. Klin Monatsbl Augenheilkd. 2007;224(5):402–410. doi:10.1055/s-2007-963156
- Nishikawa T, Edelstein D, Du XL, et al. Normalizing mitochondrial superoxide production blocks three pathways of hyperglycaemic damage. Nature. 2000;404(6779):787–790. doi:10.1038/35008121
- Cejka C, Cejkova J. Oxidative stress to the cornea, changes in corneal optical properties, and advances in treatment of corneal oxidative injuries. Oxid Med Cell Longev. 2015;2015:591530. doi:10.1155/2015/591530
- Barot M, Gokulgandhi MR, Mitra AK. Mitochondrial dysfunction in retinal diseases. Curr Eye Res. 2011;36(12):1069–1077. doi:10.3109/02713683.2011.607536
- Aldrich BT, Schlötzer-Schrehardt U, Skeie JM, et al. Mitochondrial and morphologic alterations in native human corneal endothelial cells associated with diabetes mellitus. Invest Ophthalmol Vis Sci. 2017;58(4):2130–2138. doi:10.1167/iovs.16-21094
- Tayyari F, Khuu LA, Sivak JM, et al. Retinal blood oxygen saturation and aqueous humour biomarkers in early diabetic retinopathy. Acta Ophthalmol. 2019;97(5):e673–e679. doi:10.1111/aos.14016
- Sagoo P, Chan G, Larkin DFP, George AJT. Inflammatory cytokines induce apoptosis of corneal endothelium through nitric oxide. Invest Ophthalmol Vis Sci. 2004;45(11):3964–3973. doi:10.1167/iovs.04-0439
- Shi L, Yu X, Yang H, Wu X. Advanced glycation end products induce human corneal epithelial cells apoptosis through generation of reactive oxygen species and activation of JNK and p38 MAPK pathways. PLoS One. 2013;8(6):e66781. doi:10.1371/journal.pone.0066781
- Cipriani V, Quartilho A, Bunce C, Freemantle N, Doré CJ. Ophthalmic statistics note 7: multiple hypothesis testing—to adjust or not to adjust. Br J Ophthalmol. 2015;99(9). doi:10.1136/bjophthalmol-2015-306784