To the Editor,
A 54-year-old woman was admitted due to severe back pain. Nine years previously she underwent lumpectomy and axillary lymph node dissection due to a 2.4 cm left breast invasive ductal carcinoma grade 2, ER positive, HER 2 negative, with lymphovascular invasion and involvement of two axillary lymph nodes. The patient was treated by adjuvant chemotherapy consisting of six cycles of CAF (cyclophosphamide, doxorubicin and 5 FU) followed by adjuvant tamoxifen for five years and anastrazole for 2.5 years. Due to extensive high grade ductal carcinoma in situ adjacent to the primary tumor she subsequently underwent left mastectomy. She remained asymptomatic on routine follow-up.
A computed tomography (CT)-scan preformed upon admission revealed several lytic-sclerotic lesions in D3–D6 with soft tissue extension and a lytic lesion in the first left rib. A left lung nodule of 5 × 4 cm was seen in the lingula, suggesting metastatic disease in both bone and lung. Serum tumor marker levels were within normal range.
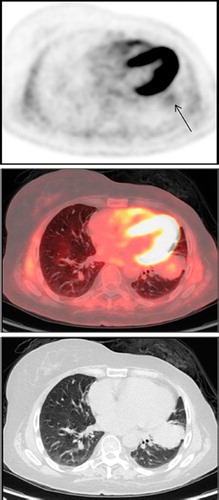
In need for a definitive tissue diagnosis before further therapeutic decisions a CT-guided biopsy of the left lung lesion was performed, revealing a synovial sarcoma. It was then unclear whether all findings represented lesions of metastatic synovial sarcoma or possibly the sarcoma was an incidental finding in a patient with skeletal metastatic breast cancer. FDG positron emission tomography (PET)/CT-scan performed for whole body assessment of the extent of disease, showed several foci of intense uptake in the thoracic spine and in the left first rib (SUVmax 4.5–6.6) (). A very low intensity FDG uptake was seen in the large left lung nodule (SUVmax 2.2) (). The discrepancy in the intensity of FDG uptake between these lesions suggested two different etiologies, leading to intensive attempts to obtain a bone biopsy. Vertebral biopsy failed but a biopsy of the first rib lesion revealed metastatic breast cancer with immunohistochemical features identical to those of the primary breast tumor.
Figure 1. FDG PET (top), PET/CT (middle) and CT (bottom) images showing a high intensity FDG uptake in a lytic-sclerotic lesion involving the body and left transverse process of T4 vertebra and the left costovertebral aspect of the adjacent 4th rib. CT, computed tomography; PET, positron emission tomography.
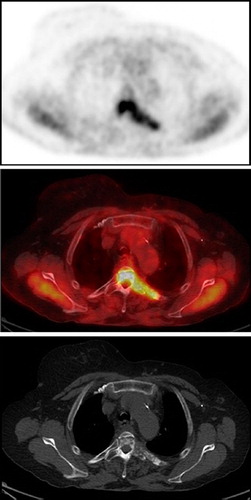
Figure 2. FDG PET (top), PET/CT (middle) and CT (bottom) images showing a very low intensity FDG uptake (arrow) in a large lung mass in the lingula. CT, computed tomography; PET, positron emission tomography.
While awaiting final diagnosis the patient was treated by irradiation of the involved vertebrae. Upon diagnosis treatment with fulvestrant was initiated and she was referred for surgery of the pulmonary sarcoma. Left upper lobectomy was performed. Histological examination of the surgical specimen revealed a monophasic synovial sarcoma. Seven hilar lymph nodes were removed and were free of tumor. The patient recovered uneventfully and is stable under hormonal therapy for metastatic breast cancer for eight months.
Discussion
Lung metastases are frequent in breast cancer and the diagnosis of a pulmonary lesion in these patients demands careful evaluation. The morphological features of pulmonary nodules in cancer patients have been described, suggesting that lesion's size greater than 10 mm can differentiate between benign and potentially malignant lesions [Citation1]. FDG PET/CT further enhances the ability to characterize lung nodules, with high intensity FDG uptake indicating the need for more aggressive diagnostic workup in suspicion for malignancy while nodules, especially large ones, with low tracer uptake are more frequently benign [Citation2]. However; in patients with metastatic disease pulmonary lesions are usually considered part of the systemic disease and are not evaluated separately.
Synovial sarcoma is a rare tumor of adolescents and young adults, located primarily adjacent to joints. The lungs are its primary metastatic site while primary pulmonary synovial sarcoma is an even rarer tumor [Citation3,Citation4]. Although FDG PET/CT imaging has a high sensitivity for various types of sarcomas, FDG uptake in synovial sarcoma is variable and has been suggested to correlate with prognosis in this rare tumor [Citation5,Citation6].
Functional imaging using FDG PET/CT is increasingly being used for the evaluation of cancer, but its use for the differentiation between various types of malignancies is not commonly described or used in clinical practice.
We describe a case of double primary tumors including a synovial sarcoma of the left lung and breast cancer metastatic to the skeleton, which were differentiated by FDG PET/CT. Biopsy of metastases in relapsed breast cancer is indicated to confirm diagnosis and determine estrogen receptor and HER 2 expression, but usually only one metastatic lesion is sampled. In this case suspicion for the existence of two different tumors arose after biopsy of the pulmonary mass unexpectedly revealed synovial sarcoma. This assumption was supported by significantly different intensity of FDG uptake in the pulmonary and bone lesions on PET/CT, supporting our intensive search for histological confirmation of bone metastatic breast cancer. This case demonstrates that in the setting of metastatic disease when there is clinical suspicion for the existence of two primary pathologies, FDG PET/CT can be useful in the diagnostic workup not only by its well documented ability to screen the whole body and detect multiple sites of the same tumor, but also by its ability to insinuate differences in metabolic-histologic properties of various malignancies in the same patient. In the case described above, the clinical presentation and the differential uptake in the lung and bone lesions led us to aggressively pursue definitive diagnostic procedures and optimal treatment plan for our patient.
References
- Lee B, Lim A, Lalvani A, Descamps MJ, Leonard R, Nallamala S, . The clinical significance of radiologically detected silent pulmonary nodules in early breast cancer. Ann Oncol 2008;19:2001–6.
- Bar Shalom R, Kanga O, Israel O, Guralnik L. Noninvasive diagnosis of solitary pulmonary lesions in cancer patients based on 2-flouro-2deoxy-D-glucose avidity on positron emission tomography/computed tomography. Cancer 2008;113: 3213–21.
- Spurrel EL, Fisher C, Thomas LM, Judson IR. Prognostic factors in advanced synovial sarcoma: An analysis of 104 patients treated at the Royal Marsden Hopsital. Ann Oncol 2005;16:437–44.
- Essary LR, Vargas SO, Fletcher CD. Primary pleuropulmonary synovial sarcoma: Reappraisal of a recently described anatomic subset. Cancer 2002;94:459–69.
- Charest M, Hickeson M, Lisbona R, Novales-Diaz JA, Derbekyan V, Turcotte RE. FDG PET/CT imaging in primary osseous and soft tissue sarcoma: A retrospective review of 212 cases. Eur J Nucl Med Mol Imaging 2009;36:1944–51.
- Lisle JW, Eary JF, O'Sullivan J, Conard JU. Risk assessment based on FDG-PET in patients with synovial sarcoma. Clin Ortho Relat Res 2009;467:1605–11.