

Abstract
Purpose
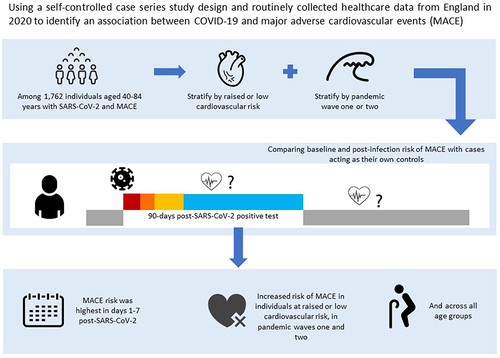
To assess the risk of incident cardiovascular outcomes after COVID-19 by level of cardiovascular risk in waves one and two of the pandemic in England in 2020.
Patients and methods
We conducted a self-controlled case-series study among adults aged 40–84 years with no pre-existing cardiovascular disease using linked data from the Clinical Practice Research Datalink. We generated season-adjusted incidence ratios (IRs) for first acute cardiovascular event after SARS-CoV-2 infection compared with baseline time before and >91 days after infection. We used composite and individual acute cardiovascular event outcomes including myocardial infarction, major ventricular arrhythmia, left ventricular heart failure, and ischemic stroke. We stratified by cardiovascular risk, using diagnosed hypertension and QRISK3 predicted risk, and by wave one and two of the pandemic.
Results
We included 1762 individuals, 76.6% had a QRISK3 score ≥10% and 59.4% had hypertension. The risk of any cardiovascular event was elevated in the 1–7 days after infection (IR 7.14 [95% CI 6.06–8.41]) and, while the effect size tapered, the risk remained for 15–28 days after infection (1.74 [1.33–2.26]). Risks were similar for individual event type, differing by level of cardiovascular risk, and in wave one and two of the pandemic.
Conclusion
SARS-CoV-2 infection is associated with early elevations in the risk of first acute cardiovascular event, across cardiovascular risk levels and in both wave one and two of the pandemic. Prevention of COVID-19 is important to avert cardiovascular complications.
Graphical Abstract
Data Sharing Statement
The data used for this study were obtained from the CPRD. All CPRD data are available via an application to the Independent Scientific Advisory Committee (see https://www.cprd.com/Data-access). Data acquisition is associated with a fee and data protection requirements. This study is supported by code lists used to define each health condition, which have been made openly available at https://doi.org/10.17037/DATA.00002763. Our data management and analysis computer code is available via GitHub at https://github.com/jenAdavidson/cvrisk_covid_sccs. All code is shared without investigator support.
Acknowledgments
This work was supported by the BMA Foundation for Medical Research/Rosetrees Trust COVID-19 grant (M958). CWG is funded by a Wellcome Career Development Award (225868/Z/22/Z). JAD was funded by a British Heart Foundation Non-Clinical PhD Studentship (FS/18/71/33938). EH is funded by a National Institute for Health Research (NIHR) post-doctoral fellowship (PDF-2016-09-029). HS is funded by the NIHR through an Advanced Fellowship (NIHR301730). The views expressed in this publication are those of the author(s) and not necessarily those of the NIHR, NHS or the UK Department of Health and Social Care. This work uses data provided by patients and collected by the NHS as part of their care and support. We thank Dr Harriet Forbes for helpful discussions on study design.
Disclosure
JB reports consulting fees from ARCbio, HVivo and GSK and participation in a data safety and monitoring board for the COM Cov trial, Oxford, now ended. AB reports grants from NIHR, AstraZeneca and the British Medical Association and leadership roles as Vice-President, Digital, Marketing, Communications for the British Cardiovascular Society and Senior Advisor to the Emerging Leaders Programme of the World Heart Federation. The authors report no other conflicts of interest in this work.