

Abstract
Purpose
Dupilumab significantly reduced the requirement for systemic corticosteroids (SCS) in patients with severe chronic rhinosinusitis with nasal polyps (CRSwNP). Patients with CRSwNP and coexisting asthma typically have a higher disease burden and have more difficulty in managing disease. Here, we report an analysis of asthma outcomes and SCS use in patients with CRSwNP and coexisting asthma.
Patients and Methods
This was a post hoc analysis of the randomized, placebo-controlled SINUS-24 and SINUS-52 studies (NCT02912468/NCT02898454) in patients with severe CRSwNP and coexisting asthma (patient self-reported) from the pooled intention-to-treat population randomized to dupilumab 300 mg every 2 weeks or placebo. On-treatment SCS use was estimated using Kaplan–Meier analysis. Forced expiratory volume in 1 s (FEV1), percent predicted FEV1, and the 6-item Asthma Control Questionnaire (ACQ-6) were assessed at baseline and Week 24 (pooled SINUS-24/52) in patients with/without history of asthma exacerbation or prior SCS use.
Results
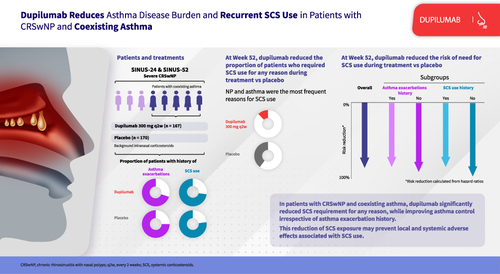
Of 337 patients with coexisting asthma, 88 (26%) required on-treatment SCS use. The requirement for on-treatment SCS use for any reason was significantly lower with dupilumab (20/167 patients; 12%) vs placebo (68/170; 40%); hazard ratio (95% confidence interval) 0.248 (0.150–0.409); p < 0.0001. The most frequent reasons for SCS use were nasal polyps (dupilumab 3% and placebo 27%) and asthma (2% and 9%, respectively). FEV1, percent predicted FEV1, and ACQ-6 were all significantly improved at Week 24 with dupilumab vs placebo irrespective of history of asthma exacerbation or prior SCS use (all p < 0.01).
Conclusion
Dupilumab significantly reduced the requirement for SCS and improved asthma outcomes irrespective of history of asthma exacerbation or prior SCS use vs placebo in patients with CRSwNP and coexisting asthma, demonstrating concomitant reduction of SCS use and asthma disease burden in these patients.
Plain Language Summary
Chronic rhinosinusitis with nasal polyps (CRSwNP) and asthma are type 2 inflammatory conditions that often coexist. Patients with both CRSwNP and asthma generally have worse symptoms that are more difficult to treat. Their standard treatment is topical (inhaled/intranasal) corticosteroids, but where this is ineffective, systemic corticosteroids, also called SCS, are used. SCS are effective at reducing nasal polyp size and improving symptoms, but this effect often does not last, and many patients experience side effects when SCS are used for a long time. Dupilumab, a drug that targets type 2 inflammation, is approved for treating both uncontrolled CRSwNP and moderate-to-severe asthma. Here, we investigate whether dupilumab changes how often patients with CRSwNP and asthma need to use SCS and its effect on their asthma. We found that dupilumab-treated patients were 75% less likely to need SCS than patients treated with placebo and also had significantly greater improvements in measures of their asthma severity, irrespective of their history of previous asthma attacks or previous SCS use. These results show that, in patients with CRSwNP and asthma, dupilumab can improve asthma symptoms and reduce the need for SCS use. Using fewer SCS may help patients avoid the side effects associated with SCS use.
Graphical Abstract
Abbreviations
ACQ-6, 6-item Asthma Control Questionnaire; CI, confidence interval; CRSwNP, chronic rhinosinusitis with nasal polyps; FEV1, forced expiratory volume in 1 s; HR, hazard ratio; IL, interleukin; NP, nasal polyps; q2w, every 2 weeks; SCS, systemic corticosteroids.
Data Sharing Statement
Qualified researchers may request access to patient-level data and related study documents including clinical study report, study protocol with any amendments, blank case report form, statistical analysis plan, and dataset specifications. Patient-level data will be anonymized, and study documents will be redacted to protect the privacy of trial participants. Further details on Sanofi’s data sharing criteria, eligible studies, and process for requesting access can be found at: https://www.vivli.org/.
Ethics Approval and Informed Consent
The SINUS-24 and SINUS-52 studies were conducted according to the Declaration of Helsinki principles and were approved by the local institutional review board or ethics committee at each study site (Supplementary Table S1). All patients provided written informed consent.
Acknowledgments
The authors thank Shahid Siddiqui, MD (formerly of Regeneron Pharmaceuticals Inc.), and Andrew Menzies-Gow, MD (Royal Brompton and Harefield Hospitals), for insights and guidance. Medical writing/editorial assistance provided by Joseph Hodgson, PhD, of Adelphi Group, Macclesfield, UK, funded by Sanofi and Regeneron Pharmaceuticals Inc. according to the Good Publication Practice guideline.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Mark Gurnell reports steering committee membership and speakers’ bureau fees for AstraZeneca, and speakers’ bureau fees for Novartis. Amr Radwan, Scott Nash, and Yamo Deniz are employees of Regeneron Pharmaceuticals Inc. and may hold stock and/or stock options in the company. Claus Bachert reports grants from Sanofi and was the principal investigator for studies for Sanofi, GlaxoSmithKline, and Novartis, during the conduct of the study. Njira Lugogo is an advisory board member and has received consultancy fees from Novartis, has received research grants from Avillion and Gossamer Bio, and is an advisory board member and has received consultancy fees and research grants from AstraZeneca, Genentech, GlaxoSmithKline, Regeneron Pharmaceuticals Inc., Sanofi, and Teva Pharmaceutical Industries Ltd. Seong H Cho has received grants from and is an advisory board member for Sanofi, and Regeneron, during the conduct of the study; received grants from the National Institute of Health, and received research grants from and is an advisory board member for Insmed, outside the submitted work. Haixin Zhang is a former employee of Regeneron Pharmaceuticals Inc. and may hold stock and/or stock options in the company. Asif H Khan, Juby A Jacob-Nara, and Paul J Rowe are employees of Sanofi and may hold stock and/or stock options in the company.