Figures & data
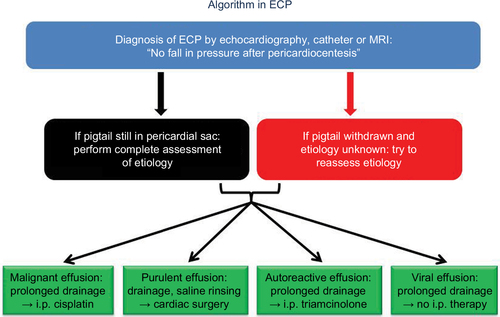
Figure 1 Cross-section of the pericardial and myocardial layers.
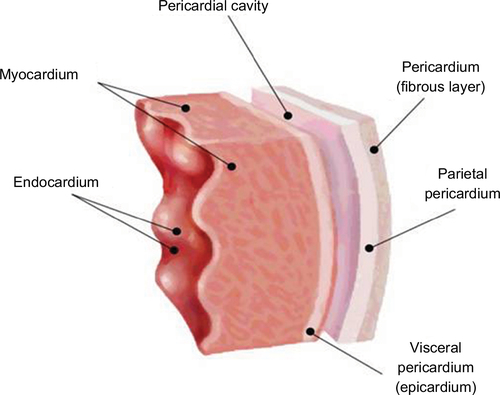
Figure 2 Dip-and-plateau phenomenon in the left and right ventricles of a patient with persisting signs of tamponade after pericardiocentesis. The persistance of an elevated end-diastolic pressure with the classic square-root sign of tamponade is diagnostic, although tamponade is no longer present. This is one of the characteristic hemodynamic features of ECP.
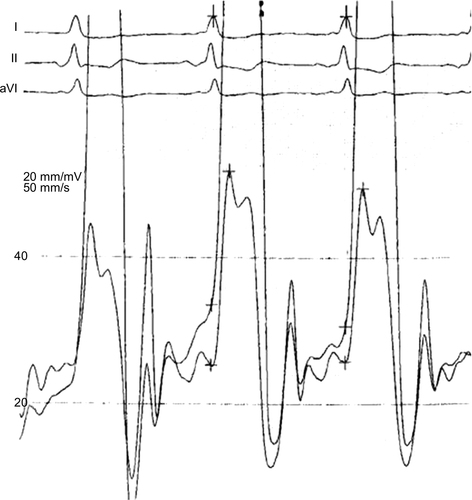
Figure 3 Epicardial inflammatory and fibrinous tissue on the epicardial side of the right ventricle (red arrow) in a 49-year-old patient with recurrence of a loculated pericardial effusion (green arrow). Most of the loculated effusion could be removed by pericardiocentesis, but signs of tamponade persisted due to epicarditis. The epicardial biopsy of this mass revealed fibrous tissue, fibrinogen and fat cells only. Neither microbial DNA or RNA by PCR nor malignancy could be detected.
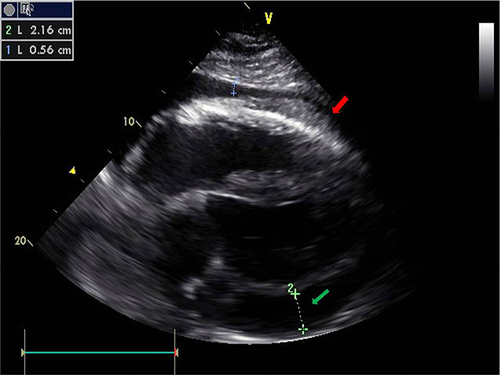
Figure 4 Cardiac MRI of a 34-year-old female half-marathon runner with recurrent pericarditis at the time of admission to our hospital.
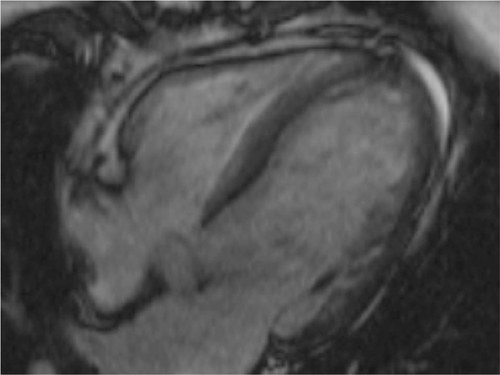
Figure 5 (A) Pericardioscopy: thickening of parietal and visceral pericardium with interspersed adhesions and some residual fluid (white light mode). (B) The interlinking adhesions (white strands) can be appreciated best in the blue light mode. The dark spots are areas of inflammation. They are the primary targets of epicardial biopsies to assess the underlying inflammation. (C) Epicarditis with small patchy fibrinous lesions. The biopsy was PCR negative for microbial DNA and RNA. Red arrow: inflamed visceral pericardium (epicardium), green arrow: parietal pericardium also with fibrinous lesions and yellow arrow: bioptome. (D) Epicarditis with a large red colored inflammatory lesion (red arrow) and an adhesive fibrous white area (green arrow). (A and B) Reprinted by permission from Springer Nature: Heart Fail Rev, Pericardioscopy and epi- and pericardial biopsy – a new window to the heart improving etiological diagnoses and permitting targeted intrapericardial therapy, Maisch B, Rupp H, Ristic A, Pankuweit S, 2013.Citation15
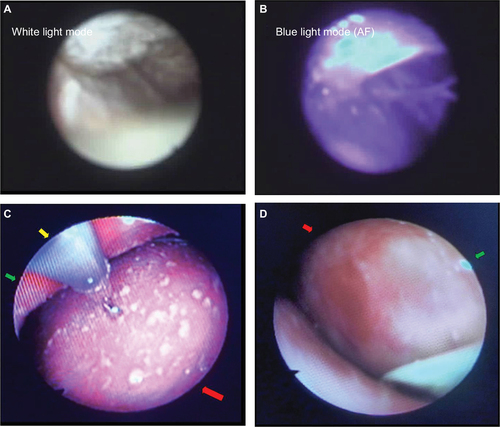
Table 1 Etiologies of pericardial effusion with ECP in a German tertiary referral center
Figure 6 Diagnostic and therapeutic algorithm in ECP.