
ABSTRACT
Background
The assessment of people with aphasia (PWA) should include the evaluation of specific language disorders and the impact of these disorders on their activities and participation in society. Due to the lack of assessment tools in Portugal aimed at the activity and participation levels of PWA, it was necessary to translate and adapt an existing instrument, the Communication Disability Profile (CDP), into European Portuguese (EP). The first EP version of the CDP (CDP-EP version 1, released originally in 2012) was further developed in this study.
Aims
The aim of this study was to validate the content of the CDP for Portuguese PWA using the Participatory Workshops method and to answer the following research question: Does the Portuguese version of the CDP measure the consequences of aphasia in Activity, Participation, Contextual Factors and Emotions in a Portuguese population with aphasia?
Methods & Resources
An expert panel of eleven PWA was consulted. The adopted methodology (Participatory Workshops) was chosen to foster critical thinking and discussion within the group. Sessions were video recorded and field notes taken. All data were transcribed verbatim and analysed using a topic guide divided in two sections: Form and content.
Outcomes & Results
The panel considered that the CDP-EP content (clarity, ambiguity, relevance, and extension of the instrument) was relevant and important, and the items reflected PWA’s reality, covering their needs. Though the CDP-EP was considered clear, the Activities (talking, understanding, expression, reading, and writing) and Participation (tasks that people have to do, want to do, and how things are at home; communication difficulty in a person’s daily life, i.e., going shopping, using money in a store, using public transport, getting back to work) sections were considered incomplete. Concerning form (design), the expert panel was unanimous in considering the instrument not suitable for Portuguese PWA and suggested adapting it to the Portuguese society and culture, e.g., as Portugal is primarily homogenous in ethnicity, the multiple cultural scales depicting different cultures/ ethnicities were not considered relevant.
Conclusions
Although the previous EP version of the CDP (CDP-EP version 1) was considered incomplete, the suggestions proposed by the expert panel consulted have been integrated making the new version of the CDP-EP an instrument able to measure the consequences of aphasia, in terms of Activity, Participation, Contextual Factors and Emotions of Portuguese PWA. Further studies need to be done in order to analyse the psychometric properties of this new version.
Introduction
Aphasia has been “typically” defined as an acquired neurogenic language disorder secondary to a brain injury (mostly caused by stroke, in the left hemisphere), involving varying degrees of impairment in four primary areas: Spoken language expression, spoken language comprehension, written expression and reading comprehension (ASHA, Citation2022). However, the consequences of aphasia go far beyond language impairments, with the need to integrate other consequences into its conceptualisation. Aphasia can result in social and psychological adversities which affect relationships and participation in different social life domains (Andersson & Fridlund, Citation2002; Dorze & Brassard, Citation1995; Parr, Citation2007). Even though there is no international general consensus (Berg et al., Citation2022), recent literature defines aphasia as a communication disability due to an acquired impairment of language modalities and functions that may affect the social participation and quality of life of the person with aphasia as well as of their family, carers and friends (Berg et al., Citation2022; Fotiadou et al., Citation2014; Martin et al., Citation2008; Papathanasiou et al., Citation2011).
This broader definition of aphasia was the result of many studies developed in the field over the last 20 years. In 2001, the revised World Health Organization’s (WHO) International Classification of Functioning, Disability and Health (ICF), emphasised the need for health professionals to consider the consequences of a disorder not just in the body structures and functions of the person, but also in their activity and participation in daily life (Frattali, Citation1998; Kearns, Citation1991; Worrall, Citation1992; Worrall & Frattali, Citation2011). According to this perspective, the person with aphasia has language deficits, limitations in communication activities, and restrictions in participation (Worrall et al., Citation2013). Many studies highlighted the potential consequences of stroke and aphasia such as restrictions on social life, fewer social activities, family life disruption, loss of or fewer contacts with friends, boredom and loneliness, as well as social isolation (Parr, Citation1994; Zemva, Citation1999). The impact of aphasia on family members and close relatives, third-party functioning and third-party disability, have also been studied (Grawburg et al., Citation2013).
Worrall et al. (Citation2002) suggested using the WHO classification in clinical practice of the speech and language therapists (SLTs) and that the rehabilitation of a person with aphasia should not focus exclusively on the impairment of language and communication. Therefore, SLTs should support communication according to current theories, which show us the importance of assessment and intervention of language disorders in aphasia, and also consider the social participation of people with aphasia – PWA (Dalemans et al., Citation2010).
Murray and Coppens (Citation2013) highlighted the need for the assessment of PWA to include measures that evaluate each component considered in the ICF. This means that assessment should consider not only the difficulties that PWA have associated with language and verbal expression, but also consider its impact in their ability to participate in daily activities and relationships, in their participation in society and the influence of personal and environmental factors in this process (Simmons-Mackie et al., Citation2014).
The most “traditional” instruments used to assess aphasia focused mainly on language impairments (Kagan & Simmons-Mackie, Citation2007; Simmons-Mackie et al., Citation2014), hence did not reflect PWA’s true performance in ordinary situations of their daily life (Frattali, Citation1998; Kearns, Citation1991; Worrall, Citation1992; Worrall & Frattali, Citation2011). The importance of including the perspective of PWA in developing assessments was also recognised by other authors (Byng & Duchan, Citation2005; Frattali, Citation1992; Leal, Citation2006; Parr, Citation1996; Pierce, Citation1996; Pound et al., Citation2002; Simmons‐Mackie & Kagan, Citation2007; Spreen & Risser, Citation2003; Threats, Citation2008). Learning about the consequences of aphasia from the perspective of PWA facilitates meaningful management of their rehabilitation (Garcia & Connor, Citation2011), and is the basis of an assessment for the person, about the person and with the person (Worrall & Cruice, Citation2005).
According to data from the Portuguese Stroke Society (SPAVC), three Portuguese people experience a stroke per hour. About a third (21% to 38%) of the survivors of stroke may have aphasia (Engelter et al., Citation2006; Laska et al., Citation2001). In this context, the Portuguese Institute of Aphasia (IPA) estimate that around 8000 new cases of aphasia appear every year in Portugal, that has one of the highest stroke rates in the European Union. Through statistical extrapolations, IPA estimates that the prevalence of PWA in Portugal is around 40,000.
In Portugal, the literature related to the assessment of aphasia is scarce. The existing tools used by Portuguese SLTs in their clinical practice with PWA do not allow them to assess all the ICF components. This may limit a broader intervention that integrates all of WHO’s directives (Matos, Citation2012). According to Leal et al. (Citation2014), the most popular assessment tools used by Portuguese SLTs (N=55) to assess aphasia are impairment-based, namely the Bateria de Avaliação da Afasia de Lisboa – BAAL (Damásio Citation1973; Castro-Caldas Citation1979; Ferro Citation1986), the Aachen Aphasie Test (AAT) – Portuguese version (Lauterbach 2006), the Escala de Funcionalidade para Afásicos – EFA (Leal, Citation2006), and the Provas de Avaliação da Linguagem e da Afasia em Português – PALPA-P (Castro et al., Citation2007). Leal et al. (Citation2014) have also shown that Portuguese SLTs’ practice is structured according to the rehabilitation model of intervention and focuses on the activity level, and that future developments in practice are likely to include assessment tools that supports this.
In the last ten years, several studies have been carried out with the purpose of overcoming the lack of assessment instruments in this context (Matos et al., Citation2014). These studies were mainly focused on the translation to European Portuguese (EP) and adaptation of different assessment instruments to the Portuguese reality. Matos et al. (Citation2014) explored the aphasia assessment instruments available in Portugal, identifying 20: Ten of these instruments were impairment based; four assessed activity limitations; four assessed activity limitations and participation restrictions; one assessed barriers and facilitators; and one assessed the quality of life of PWA. However, most of the psychometric properties of these tools are still being studied, so the vast majority of instruments translated and adapted to EP are yet to be validated and are not available for a general use in clinical practice (Matos et al., Citation2014). One of those instruments is the Communication Disability Profile (CDP), originally developed by Swinburn and Byng (Citation2006), translated and adapted to EP (Matos, Citation2012).
The CDP is an instrument that allows PWA to express their views and experiences of living with aphasia, regardless of the form in which they do it, i.e., through pointing, writing, or speaking in four sections: Activities, Participation, External Influences (barriers and facilitators) and Emotions. Since the individual is at the centre of the process, the experience itself is reported in the first person. It allows professionals and PWA to explore and quantify its impact on daily living (Swinburn & Byng, Citation2006). The CDP helps professionals to understand which aims and objectives need to be achieved in the intervention process, according to the person’s needs and expectations (Swinburn & Byng, Citation2006).
Matos (Citation2012) interviewed three different groups of participants [PWA (n=14), SLTs (n=10) and Family/Friends (n=14)] in order to understand the consequences of stroke and aphasia in their daily lives and analyse if they were covered by the CDP items. ICF categories were used in order to codify the data obtained. Main results of the interviews conducted in this study indicated that with regard to the consequences of stroke and aphasia in the ICF domain of Body Functions and Structures, the three groups were unanimous in considering the category of Specific Mental Functions as being the most disturbed. However, within this framework, SLTs gave more value to Emotional Functions, PWA to Mental Language Functions and Family/Friends to both subcategories already mentioned, as well as the subcategory of Energy and drive functions.
In terms of Activities and Participation there was a consensus in the three groups regarding to: (1) the consequences on Personal Interactions and Relationships, (2) Social and Civic Community Life, and (3) Main Areas of Life. The consequences in Communication were only valued by SLTs and PWA. The categories of Mobility and Domestic Life were only valued by PWA and Family/Friends. Finally, the category of Self-Care and Autonomy, were only valued by the Family/Friends group. The Environmental and Attitudinal were mentioned as the main Barriers. They also considered the existence of Personal Factors, which in some way may hinder a more active participation (Matos, Citation2012).
An initial evaluation of this version of the CDP-EP (Matos, Citation2012) was also conducted with the three groups (10 SLTs; 4 PWA; 4 Family/Friends), exploring the relevance of its items, the instrument format, words, images, and scales used. Each group was also asked to assess the comprehension, clarity, practicability, and acceptance/approval of the instrument. The appraisal of the CDP-EP was very positive, and PWA did not suggest any modifications. However, this first version of the CDP-EP was not considered as truly reflecting the reality of Portuguese PWA, since during the interviews PWA offered few or limited critical commentary and tended to agree with what facilitators said. Researchers hypothesized that due to the type of intervention model usually followed in Portugal (medical model), PWA were not used to being consulted, and suggested that further research was needed in order to finish the content validation of the CDP-EP (Matos, Citation2012).
In order to complete CDP-EP’s first version content validation and try to obtain more information directly from PWA, we have used a different methodology: Participatory Workshops. This method consists of a series of meetings in groups with people who have lived through a specific experience (in this case, by PWA). Participatory Workshops encourage PWA to share their opinions and allow them to participate in the validation process without worrying about their status, i.e., having aphasia (Alliance, Citation2001; Galliers et al., Citation2012; Kanji & Greenwood, Citation2001; Mc Menamin et al., Citation2015).
Aim of the study
The aim of this study was to validate the content of the CDP-EP by PWA through the Participatory Workshops method, in order to answer the following research question: Does CDP-EP measure the consequences of aphasia in Activity, Participation, Contextual Factors and Emotions in a Portuguese population with aphasia?
Method
Study design
Content validity is one of the most important measurement properties of a patient-reported outcome measure (PROM) as well as sensitivity and reliability. It refers to the relevance, comprehensiveness and comprehensibility of the PROM for the construct target population, and context of use of interest (Terwee et al., Citation2018). It can be assessed by asking patients and professionals about the relevance, comprehensiveness and comprehensibility of the items, response options and instructions (de Vet et al., Citation2011; Streiner et al., Citation2015).
The constitution of a panel of experts for content validation should consider the characteristics of the instrument, training, skills and the availability of the experts, as well as their experiences (Grant & Davis, Citation1997; Terwee et al., Citation2018). A relevant factor when selecting these experts is clinical expertise (Davis, Citation1992; Grant & Davis, Citation1997; Terwee et al., Citation2018). It should include people potentially related to the population being studied (e.g., family members and patients) to ensure the accuracy and relevance of languages and terms (Alexandre & Coluci, Citation2011), since they are familiar with the caregiver burden and clinical practice. Furthermore, members of the target culture (people potentially related to the issue) can help ensure that all relevant content of the instrument is included as well as irrelevant content is excluded and mutual understanding of the construct is achieved (Leung & Arthur, Citation2000; Mohr & Tulman, Citation2000). Others studies (Grant & Davis, Citation1997; Terwee et al., Citation2018), advocate that diversity is more important than size. However, these authors argued that a minimum number of professionals (experts) may be needed (at least 7 for a very good rating).
Since the CDP was designed to determine the impact of aphasia on PWA, it was necessary to involve PWA in the present study to test the validity of CDP-EP based on their own experiences (Galliers et al., Citation2012; Mc Menamin et al., Citation2015; Pearl et al., Citation2011; Swinburn & Byng, Citation2006).
The Participatory Workshops method consists of a series of sessions/meetings in groups of people who have lived through a specific experience during a previously established period of time. Each session takes approximately two hours, due to the limitations that exist in the level of auditory comprehension and the need to explain the objectives and carry out all activities (Dalemans et al., Citation2010; Galliers et al., Citation2011, Citation2012). The approach encourages people to share information, learn from each other, and work together to solve common problems. It allows PWA to actively participate in the process, without worrying about their status (having aphasia), or their ability to communicate formally (Alliance, Citation2001). The Participatory Workshops methodology includes active approaches which encourage people to think for themselves. Facilitators help group members to develop communication skills by promoting discussion. Activities such as games (ice breakers, energisers and games to make people think), visual tools, role play and case studies are used to explore different points of view (Alliance, Citation2001).
Ethical considerations
Two independent ethics committees gave approval for this study: Unidade de Inovação e Desenvolvimento do Centro de Ensaios Clínicos do Centro Hospitalar e Universitário de Coimbra, Portugal and Unidade de Investigação em Ciências da Saúde: Enfermagem (UICISA: E) da Escola Superior de Enfermagem de Coimbra (ESEnfC), Portugal. An aphasia-friendly informed consent form, available as supplementary materials, was signed by all participants (simplified vocabulary, increase font size, little information per page and use of images, short sentences and with little information, content informative words written in lowercase letters and in bold (Rose et al., Citation2010), since it facilitates the comprehension of PWA, as suggested by Brennan et al. (Citation2005).
Participants
In order to recruit the sample necessary to carry out our study, two health services providers were contacted: The Portuguese Institute of Aphasia (Instituto Português da Afasia – IPA) in Matosinhos, north of Portugal and the Coimbra University Hospital (Centro Hospitalar e Universitário de Coimbra – CHUC), in Coimbra, centre of Portugal. Participants were recruited by the local SLTs, according to the following inclusion criteria: people of both sexes; over 18 years of age; native speakers of EP; at least 3 months post onset following a stroke; living at home; have an aphasia diagnosis according to the Lisbon Aphasia Assessment Battery/Bateria de Avaliação da Afasia de Lisboa – BAAL (Caldas, Citation1979; Damásio, Citation1973; Ferro, Citation1986); a reliable yes/no response (no less than 7 on the BAAL yes/no questions, with a total score of 8 points); no hearing problems that would interfere in the communication process, as reported by PWA; no presumed cognitive disorder according to the Language-Modified Mini-Mental State Examination (LMMMSE) – European Portuguese (Matos & Jesus, Citation2011) (no less than 22 in a total of 30) and also according to the information in the clinical history of the person; not pre-morbidly illiterate.
The participants were contacted by the first author of this paper. Two meetings were subsequently held, one meeting for the IPA Group and another for the CHUC Group. In these meetings, the aims of the study were explained. After having agreed to participate in the study, the participants were assessed according to previously established inclusion criteria by an experienced SLT (last author of this paper).
Eleven PWA (7 men; 4 women) participated in the study, with a mean age of 57 years (range 37-68 years; SD=8.4 years), and a mean of 11 years of schooling (range 4-20 years; SD=6.7 years), shown in . Participants were on average 5 years post-stroke (range 1-13 years; SD=4.0 years). All participants scored within the normal range for cognitive functioning (mean LMMSE score=27.4; SD=1.6; range 25-30).
Table 1. Demographic, aphasia and cognitive status of participants with aphasia of the CHUC Group (n=5).
Table 2. Demographic, aphasia, and cognitive status of participants with aphasia of the IPA Group (n= 6).
The Communication Disability Profile (CDP)
The CDP includes four sections: Activities, Participation, External Influences (barriers and facilitators) and Emotions. Each section contains a series of questions that explore different aspects of what living with aphasia means to the respondent. The Activities section consists of twenty items that explore communication activities of everyday life (speaking, communicating, understanding, reading, and writing). The Participation section is composed of fifteen questions that seek to understand the perception of each individual regarding how aphasia affects daily tasks (e.g., go shopping, money, health, transport and job). The External Influences section consists of three items, and assesses what helps and hinders Social Participation, identifying Barriers and Facilitators for each person. The final section, Emotions, consists of seventeen items. It explores the emotional state of PWA, in relation to mood, self-image and levels of satisfaction with their present and future life.
All scores are generated using a pictorial scale. There are different representative scales which vary in relation to ethnicity, age, and sex. PWA choose the one that they most closely identify with. The results obtained from the scales, are converted into a numeric value, which allows the calculation of a score in each section (Swinburn & Byng, Citation2006).
It should be noted that the CDP was originally developed under the guidance of a group of PWA. This has contributed to ensuring that the content, text, design, images and the administration of the CDP were accessible and acceptable to PWA (Swinburn & Byng, Citation2006).
Procedures
We explored the perspective of eleven PWA about the form (design) and content (clarity, ambiguity, relevance and extension) of CDP-EP. For logistical reasons and to ensure the comfort of PWA, the panel of experts was divided into two geographically disparate groups (the IPA Group in North Portugal and the CHUC Group in the centre of Portugal). The first group to be consulted was the IPA Group. The meetings took place at the IPA headquarters and were conducted by two SLTs, co-authors of this study (A.S. & M.M.). The CHUC Group met at the Centro Hospitalar e Universitário de Coimbra, with the assistance of the last author of this paper (M.M.).
Two types of sessions were arranged: Group meetings and individual meetings. The aim of group meetings was to present the CDP-EP version 1 and perform its validation, as well as the validation of the new versions obtained during the different phases of the study, through the adoption of the Participatory Workshops method. Each group session took approximately two hours.
The purpose of individual meetings was to provide a direct contact of PWA with the initial version (version 1) of CDP-EP. This allowed PWA to better understand the performance of the instrument, assess what should be included and thus evaluate the weaknesses, strengths, and potential omissions of the existing CDP-EP. Each individual meeting lasted approximately one hour.
Galliers et al. (Citation2011, Citation2012) recomended a maximum of two to three elements per meeting, to avoid fatigue of the participants, ensuring that all previously planned topics were discussed in each session. Attention was paid to clearly explain the objectives and all activities and ensuring everyone present had understood what was required.
Group discussions were supported by a slide presentation prepared specifically for the purpose. This technique was previously used in other studies with PWA (Pearl et al., Citation2011). It can help guide the meeting, by giving support to what is being said during the discussion, by providing language samples, thus making communication more effective (Pearl et al., Citation2011).
The sessions were guided by two SLTs with experience in aphasia (A.S. & M.M.) and total communication strategies were used (Pearl et al., Citation2011) in order to obtain as many suggestions as possible from PWA, especially people that were most affected in terms of expression and understanding skills. This technique provides written and illustrated material to support conversation and make changes in its pace/speed, quality and linguistic content (Pearl et al., Citation2011). Non-verbal communication was encouraged, both to stimulate and to shape the discussions. The Supported Conversation for Adults with Aphasia (SCA) method (Kagan et al., Citation2001), which promotes the use of communication ramps to allow access to the conversation, was also implemented. In this study the participants cooperated with each other in order to help those participants with more difficulties in auditory comprehension and verbal expression. The participants were motivated and therefore contributed actively to group discussions.
Data collection took place in five distinct phases:
Phase 0 – Assessment: Contact with the participants and assessment with BAAL and LMMSE to ensure they fulfilled the inclusion criteria.
Phase 1 – Group sessions (CDP-EP version 1): Presentation of CDP-EP version 1; validation study regarding its form (design) and content (clarity, ambiguity, relevance, and extension of the instrument) in group meetings (see supplementary materials), according to the Participatory Workshops method.
Phase 2 – Individual meetings (CDP-EP version 1): Content Validation of the CDP-EP version 1; all participants reviewed and evaluated the instrument and added individual suggestions/changes to those proposed in phase 1.
Phase 3 – Group sessions (CDP-EP version 2): Presentation and analysis of CDP-EP version 2 in each group (IPA Group and CHUC Group) using the Participatory Workshops method.
Phase 4 – Data analysis and production of CDP-EP version 3.
Data analysis
All sessions were video recorded, field notes were taken, and all data was transcribed verbatim. It should be noted that for data transcription, all types of communication used by the panel members were accepted: verbal and non-verbal communication.
The form and content of CDP-EP was evaluated using a topic guide (see supplementary materials), which was divided into two sections: form and content. The first section (form) focused on the validation of the visual presentation of the instrument – words (font, size, bold), images (colours or black and white) and scales (number of scales). Overall, the proposal was to validate the design of the CDP-EP. Regarding content (second section), we aimed to validate the clarity of the instructions (accessibility of the answers); the clarity of items (ease of understanding, necessity to remove/replace information); the relevance of items (according to Portuguese PWA); the ambiguity of the instrument (the purpose of it); and the clarity of the images (if they are adequate to the written information, accessible and help to understand the purpose of the items).
Results
The results will be presented according to the phases previously described in the Method section. First, the feedback obtained from PWA regarding Form (Design) and Content (Ambiguity, Clarity, Relevance and Extent of the Instrument) issues (Phases 1 and 2) will be presented. Finally, the suggestions/changes proposed for each issue were incorporated in a new version of the instrument and were presented once more to the group of PWA (phases 3 and 4).
PHASE 1 | PHASE 2
The results obtained from phases 1 and 2 are presented together, since the main purpose of the two phases was the validation of the CDP-EP version 1. It should be noted that in phase 1 the results were obtained through group meetings whereas in phase 2 through individual meetings. The implications of the implementation of the different types of meetings are described further on PHASE 3 in the subsection “Implications and consequences of the adoption of participatory workshops methodology on suggestions/changes from phases 1, 2 and 3”.
FORM – Design
The results presented in are related to the design of the scales: Its text and images; the type and size of the font, line spacing, pictures (colour or black and white); the number and type of scales used.
Table 3. Suggestions about Design.
All participants agreed that the design of the instrument was not adequate: “It is the colour that is missing, otherwise it is well understood” (in M.P.’s own words). M.P. also referred that “this one is better”, pointing to the image with an increased line spacing, just like J.C. and J.F. did. Overall, most of suggestions were related to making the design more aphasia-friendly as suggested by Brennan et al. (Citation2005) and Worrall et al. (Citation2002).
Content
Clarity
All participants agreed the instrument’s items and images were clear (CHUC Group n=5; IPA Group n=6). It is worth mentioning that the images are part of the form (in colour or black and white) and content (if they are adequate to the written information, accessible and help to understand the purpose of the items), as referred in the methodology. However, some participants classified the instrument as incomplete and recommended some adjustments. B.M. mentioned that the expression “Done it” should be translated to Portuguese. “Write text messages on the phone (…) add money (…) add tax (in B.M.’s own words) (see ).
Table 4. Suggestions made by both groups about the category Clarity in Phases 1 and 2.
Table 5. Suggestions made by both groups about the category Clarity in Phases 1 and 2.
Table 6. Suggestions made by both groups about the category Clarity in Phases 1 and 2.
Participants reported positive aspects such as the: Participation section; accessible language; CDP-EP version 1 is “suitable” and demonstrates PWA’s “problems”. As for the negative aspects of the CDP-EP version 1, one participant with global aphasia highlighted its application duration (“too long” in H.A.’s own words).
Relevance
When the facilitator queried the participants about the relevance of the CDP-EP, all participants considered the instrument content relevant to their needs. Indeed, all participants said “Yes” and C.C., L.C., J.F. and V.C. pointed to the card with the word “Yes” written on it. The items cover the needs felt, with most items considered by the panel as “important” questions since they allow PWA to “(…) speak (…) about everything!” (J.C.). One of the positive aspects mentioned by the panel was that the CDP-EP version 1 used “words, sentences (…)” (J.O.) with an accessible language. (“It is suitable … OK … it demonstrates my problem” V.C.).
Ambiguity
None of the panel members considered the CDP-EP an ambiguous instrument regarding the items and images used. This meant, the panel concluded that items of the CDP-EP version 1 were accessible, the images were suitable and met their intended purpose.
Extent of the instrument
Four PWA considered the CDP-EP version 1 very long (CHUC Group n=2; IPA Group n=2) and seven PWA considered the instrument to have “reasonable” length (CHUC Group n=3; IPA Group n=4).
PHASE 3
Two PWA from the IPA Group dropped out at the beginning of Phase 3 due to personal reasons and health conditions. It should also be noted that the data explored at this stage is related to the changes proposed by PWA in phases 1 and 2, as mentioned in the Methods section. In other words, it was intended to verify/confirm that the changes made by each group to the CDP-EP version 1 were in line with what had been proposed in phases 1 and 2 by our panel of experts. Group sessions consisted of: presentation and analysis of CDP-EP version 2 in each group (IPA Group and CHUC Group) using, once more, the Participatory Workshops method. In phase 3, we intended to show PWA the CDP-EP version 2 that resulted from phase 1 and phase 2, in order to make sure this version was in accordance to PWA suggestions. In practice, we verified and analysed the suggestions given in phase 1 and phase 2.
FORM – Design
The two expert panels (IPA and CHUC groups, totalling 9 PWA) analysed and discussed the changes that were proposed during phases 1 and 2, concluding that their implementation brought some improvements to the instrument (B.M. “it’s better”).
CONTENT – Clarity
The panel confirmed the suggestions concerning the clarity of the CDP-EP version 1 proposed in phases 1 and 2. They considered the new version (version 2) of the CDP-EP to be clearer and less ambiguous. However, CHUC Group members still mentioned the need to increase the size of images (n=3), suggested the introduction of a new topic “speak using the computer” (n=5), and changed some words in order to reflect more the Portuguese society and facilitate the understanding of the topics (e.g., change original word “sentence” to “title”; change de original name of the story book to Anita’s story (n=4).
CONTENT – Relevance
The panel stated that the suggestions concerning the relevance of the CDP-EP version 1 proposed in phases 1 and 2, contributed towards the fact that the CDP-EP version 2 was more appropriate and relevant to Portuguese PWA.
CONTENT – Ambiguity
The panel accepted the suggestions regarding the ambiguity of the CDP-EP version 1 proposed in phases 1 and 2, claiming that the modified instrument (CDP-EP version 2) was now less ambiguous, although in a first phase of this work, the panel found the instrument items accessible (their purpose was understood).
Implications and consequences of the adoption of Participatory Workshops methodology on suggestions/changes from phases 1, 2 and 3
Most of the suggestions (98%) were collected during the Participatory Workshops. Very few suggestions (2%) came out of individual meetings with PWA. It is important to mention that PWA proposed eighty percent (80%) of the suggestions and only twenty percent (20%) were proposed by the first author of this paper.
PHASE 4
In this final phase, both groups were informed of the suggestions made to the CDP-EP version 2 (the suggestions of the CHUC Group were presented to the IPA Group and vice-versa). The aim was for each group to validate the suggestions that best represented the different contexts and situations in which aphasia can interfere, according to their views. In this phase, three of the IPA Group participants dropped out, again for personal and health reasons.
present the suggestions proposed by both groups and confirmed during this final stage of the validation process of the CDP-EP version 2. The suggestions refer to the pages of the CDP-EP version 1 that were amended. identifies the indicators most used by the panel of experts to validate the suggestions proposed in the tables aforementioned. shows that 54% of suggestions were to add small elements (44%) such as inserting words in the scales, and also adding new topics (10%) for example “Speak on the mobile phone”. Thirty nine percent (39%) of the comments were related to modification of the instrument (e.g., change the word “stroke” to “thrombosis”, a term used by the Portuguese population to generalise stroke, ischemic or haemorrhagic). Finally, 7% of suggestions had to do with the elimination of some items that were considered not to be representative of the Portuguese population (e.g., eliminate the scales which represent other cultures around the world; eliminate pages of the CDP that do not make sense to the Portuguese population (example from the , in the line that identifies page 71 – “use a single picture” (originally, there were 3 pictures for the same subject).
Figure 1. Indicators used to validate suggestions for the final version of the CDP for the Portuguese population with aphasia.
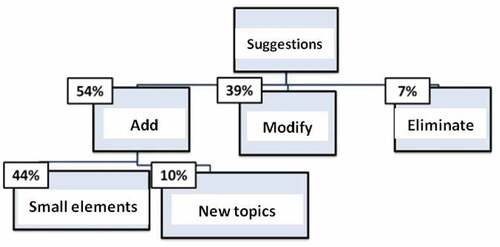
Table 7. Validated suggestions for the final version of CDP-EP.
Table 8. Validated suggestions for the final version of CDP - EP.
Table 9. Validated suggestions for final version of CDP-EP.
Discussion
The aim of this study was to validate the content of the CDP-EP in order to answer the following research question: Does CDP-EP measure the consequences of aphasia in Activity, Participation, Contextual Factors and Emotions in a Portuguese population with aphasia? Thus, the validation of the CDP-EP was carried out by a panel of experts constituted by PWA in order to guarantee the integrity of its validation, through a Participatory Workshop’s method (Alliance, Citation2001; Galliers et al., Citation2012; Kanji & Greenwood, Citation2001; Mc Menamin et al., Citation2015).
PWA as consultants
The original CDP (Swinburn & Byng, Citation2006) was designed under the guidance of a group of PWA in the UK, and the current version of CDP-EP has taken the same approach. This ensured that the content, text, design, images and administration of the CDP were accessible and acceptable to PWA, and addressed their needs and difficulties (Swinburn & Byng, Citation2006). It has been shown by other authors (Simmons‐Mackie & Kagan, Citation2007; Threats, Citation2008) that learning about the consequences of aphasia from the perspective of PWA facilitates the management of their rehabilitation (Garcia & Connor, Citation2011), and this can be the basis of an assessment for the person, about the person and with the person (Worrall & Cruice, Citation2005).
Participatory Workshops
The method we used (Participatory Workshops) allowed the majority of suggestions to be given by PWA and not by the authors. This was a key contribution since in previous studies (Leal et al., Citation2014; Matos, Citation2012) the participation of PWA was not substantial, possibly due the type of intervention model usually followed in Portugal (medical model) or the methodology adopted – individual consultation (Matos et al., Citation2010). Matos (Citation2012) also stated that PWA had not been consulted and that further research was needed in order to finish the content validation of the CDP-EP. The use of the Participatory Workshops method in this study encouraged people to share information, learn from each other, and work together to solve a common problem. It allowed PWA to actively participate in the process, without worrying about their aphasia or their ability to communicate formally. It allowed (1) the integration of PWA, creating a less formal environment and enabling them to feel more comfortable, and (2) a hierarchy of equality towards those who interview them. The involvement of PWA, due to their difficulties in auditory comprehension and/or expression, is not something that facilitates data collection. However, strategies to overcome these communication barriers, such as the adoption of aphasia-friendly material, the use of a slide presentation with what is being said during the discussion and the use of simple language were valuable tools for facilitating the process. The implementation of the strategies proposed by the SCA framework was a facilitator that we also used for data collection.
Design
Regarding the Form (Design of the CDP-EP version 1), the panel of experts was unanimous in saying that it was not adequately formatted for Portuguese PWA. Most of the suggestions provided were related to the text (line spacing, highlighting parts of the text, key words) and image formatting (colour was missing; make design more aphasia-friendly). These changes are in line with what is described in the literature (Brennan et al., Citation2005; Reis et al., Citation2006). According to Rose et al. (Citation2011), PWA prefer spaced out information, bold text, black text, key information highlighted and the use of colour images. There is a general agreement, in the literature, that well organised information can assist understanding (Rose et al., Citation2011). In the literature it is also mentioned that some PWA emphasized the need to include objective graphics/images to assisting reading and captivate potential readers (Rose et al., Citation2011).
Other suggestions were specifically to the Portuguese society and culture. An example of this, is the fact that the panel proposed the reduction of the number of scales (the panel choose only scale A1) and pictures used in the domain of Participation. In the development of the original instrument, Swinburn and Byng (Citation2006) felt that it would be beneficial to use 8 different scales, due to the cultural diversity of their country (UK). This is not applicable in Portugal, so both groups suggested reducing the number of scales (to A1) and images in CDP-EP version 3. Also, as Portugal is primarily homogenous in ethnicity, the multiple cultural scales depicting different cultures/ ethnicities were not considered relevant. The most recent data (PORDATA, Citation2020) indicated that only 6% of the Portuguese population were foreigners with legal resident status. The majority were from Europe (38%), followed by America (31%), Africa (16%) and Asia (15%). However, it should be noted that, if foreigners were included in the sample, the results would most likely be different. In this way, future research should be carried out in order to follow the cultural evolution of the country to ensure that CDP is accessible to the entire current population.
Content
The original CDP was developed for use in the UK and its culture and society (Swinburn & Byng, Citation2006) which are quite different from the Portuguese one, so some aspects needed to be changed and adapted. The Participation section was designed to understand the perception of each individual regarding how aphasia affects daily tasks (e.g., going shopping, using money in a store, having a health-related conversation with a General Practitioner, using public transport and getting back to work). Suggestions were made in order to complete and adapt the CDP-EP version 1 to the current reality of Portuguese PWA, introducing some items that are more in line with Portuguese culture and reality, such as going fishing, cycling or playing cards, and also playing traditional Portuguese games like jogo da malha. Another adaptation was related to the development of new technologies that appeared since the original CDP was written. The added topics were suggested in order to complete all the areas and contexts encountered by individuals.
The panel considered the CDP-EP version 1 as an incomplete instrument, specifically in the sections related to Activities and Participation. Originally (Swinburn & Byng, Citation2006), the Activities section explored communication activities of everyday life like speaking, communicating, understanding, reading and writing, without any use of technology (computer, smartphones or any other media).
The widespread use of technology in societies is a worldwide phenomenon causing profound changes in all dimensions. Therefore, the way people communicate has evolved since the CDP was originally designed and since then, technology has reshaped our interactions. An example of this, are the social networks that have changed and continue changing the way people engage with each other (Lamey, Citation2018). This new form of communication helps people to be closer to each other when they would have otherwise lost contact (Lamey, Citation2018). The pandemic situation caused by COVID-19 reinforced the use of such technologies and the need to consider them in assessment tools like the CDP. Portuguese PWA also observed this, so new topics such as “communicate using a computer” and “speak on the mobile phone”, were added. It should be noted that it was the CHUC Group with the highest level of education and with higher professional positions and responsibilities that suggested such topics. The time post stroke was similar in both groups as well as their age.
The remaining suggestions/changes made related to the clarity of the images. The experts were focused more on changing (e.g., change the word “stroke” to “thrombosis”) and on adding (e.g., add words to the scales, add new topic “speak on the phone” and “speak trough the computer” in order to make a video call) some details in order to improve the image clarity (e.g., increase images size, modify some details in the images like changing the expression of some of the people that were portrayed from happy to sad, and deleting unnecessary information that introduce visual noise). This is in agreement with what is described in the literature that well organised information can assist understanding (Rose et al., Citation2011). Regarding the type of text/words, there were only a few suggestions such as line spacing, font size and font type, and a phrase on a single line. These suggestions have been previously emphasized in the literature (Brennan et al., Citation2005), when referring to the importance of accessible information for PWA – aphasia friendly information (Rose et al., Citation2010; Rose et al., Citation2011). It is important to mention that the PWA who suggested most of these changes were people with worse language comprehension. Rose et al. (Citation2003) found that 12 people with mild to moderately severe aphasia were able to comprehend significantly more health information when the information was modified using simple words and short sentences, large font size (size 18), standard font (Times New Roman), ample white spacing, and pictures (Microsoft ClipArt). Regarding line spacing, in the study carried out by Rose et al. (Citation2010), a small number of participants did not consider white space helpful. These participants tended to have more severe reading difficulties, indicating that white space may not be enough to assist when reading difficulties are severe. In our study, all participants of IPA Group suggested this but, only one person (H.A.) of the CHUC Group mentioned it. The main difference between both groups was their AQ (IPA average AQ = 63.3; CHUC average AQ = 55.46), which suggests that the CHUC Group tended to have more difficulties, compared with the IPA Group. Some studies (Rose et al., Citation2003) indicate no clear relationship between aphasia-friendly effectiveness and aphasia severity, but a scatterplot comparing AQ and aphasia-friendly effectiveness has shown that participants with moderate to mild aphasia (participants’ AQ values ranging between 75 and 92) benefited the most from aphasia-friendly brochures (Rose et al., Citation2003).
Length of the CDP-EP version 2
In this study, participants mentioned the length of the instrument as being reasonable. However, there were some PWA (participants’ AQ ranging between 29.7 and 66.1; H.A., D.G., J.F. and B.M.) that found the CDP-EP version 2 to be too long and one of them (AQ – 66.1; B.M.) mentioned that the administration of the CDP-EP should be done in two sessions. These findings do not seem to be in accordance with the literature (Matos et al., Citation2010), which found that the length of CDP-EP version 1 was not criticised by PWA but was considered too long by a family member. This method of administration (over more than one session) was used in another study (Chue et al., Citation2010) due to the participant’s fatigue.
According to Chue et al. (Citation2010), the CDP’s duration of administration may be important as timing can affect a person’s mood and a person’s perception of the impact of aphasia on their Activities and Participation status. Note that in the same study (Chue et al., Citation2010), there was no significant correlation between severity or comprehension abilities and the absolute difference scores between trials, showing that severity and comprehension abilities did not impact on the overall reliability of the participants’ response. This reinforces the need to provide preliminary support for the reliable use of the CDP by people with severe aphasia. Nevertheless, it was mentioned by the authors that the CDP may be an unviable instrument for some people with extremely serious communication difficulties. In the present study, PWA who reported that the CDP was too long had an AQ between 29.7 (H.A.) and 77.6 (L.A.).
Personal factors influencing PWA’s opinions
Most suggestions/changes obtained in phases 1, 2 and 3 were proposed by PWA who had more years of schooling, had professions/occupations that required more responsibility and important positions as well as the younger population and also those who had a longer time post onset. Some of these factors are referred to in the ICF as Personal Factors (WHO, Citation2001).
Suggestions: General
As mentioned in the Method and the Results sections, the first author moderated the meetings, encouraged suggestions and discussions within the group and also provided some suggestions supported by other studies (Matos, Citation2012). However, in the light of the results obtained, it was perceived that the groups that constituted the panel were not influenced by her opinions, as they accepted and rejected her ideas and made their own suggestions, without hesitation. Looking at the sample characteristics of the CHUC Group, it was noted that its participants had the highest education level and highest professional positions and responsibilities, which might lead to a greater interaction with technology. This observation may justify the large number of changes and suggestions given by this group concerning the technological component.
Suggestions: Personal and contextual factors
From the data collected in phase 0 and the interaction between the participants and the first author over the meetings, it is clear that the participants with more communicative situations in their daily lives offered more criticisms of the CDP. These results agree with those described by Dalemans et al. (Citation2010), who mentioned that the more communication situations PWA have in their daily lives, the more their communication skills are encouraged and the more they are predisposed to social participation. Although there were participants who had lived with aphasia longer (M.P., L.A. and J.C.), their level of education and professional responsibilities were lower, a fact that may have contributed to fewer suggestions. Moreover, our previous and concurrent social interaction make us who we are and how we react at the moment (Simmons-Mackie & Damico, Citation2007). Another aspect to consider is that these participants live in a large city, with a vast number of distractions and ambient noise. Regarding the environmental factors reported in the literature (Dalemans et al., Citation2010), it is known that with this type of environmental barriers, the predisposition of PWA to communicate decreases. Living in big cities with overwhelming city noise and social distractions makes it more difficult to interact with people. Usually, people did not know each other and lived therefore more individually, making contact more difficult (Dalemans et al., Citation2010).
Strengths and Limitations of this study
The main strength of the study was the inclusion of PWA in the entire process, resulting in a new version of the CDP-EP more suitable for this population. It was clear from the literature (Ghidella et al., Citation2005; Matos, Citation2012) that the opinion (needs, aims and desires) of the PWA is different from that of their families and health professionals. If the perspectives of PWA as service users are taken into consideration, in all phases of research, new findings will be generated, the translation to real-world clinical practice will be accelerated and functional interventions and strategies for living successfully with aphasia will be promoted (Charalambous et al., Citation2020). The use of Participatory Workshops produced novel results from those reported before in studies that involved PWA with other methodologies (Matos, Citation2012). This study also demonstrated the importance of exploring cultural relevance when adapting assessment tools. By engaging PWA who lived in Portugal and spoke Portuguese, the team were able to make the adaption of the original CDP culturally relevant and appropriate for its intended end users. The therapeutic intervention plan for PWA is likely to be enriched since it can then consider goals that meet their needs, in a variety of contexts.
The results obtained in this study may be a beginning for clinical practice in Portugal to be more appropriate and directed to the needs of PWA. However, the sample of the present study was insufficient for the findings to be more consistent. The sample should include a larger number of participants, as evidenced in other studies mentioned in Charalambous et al. (Citation2020).
Future work
Further research is necessary to determine if the CDP-EP version 3 is suitable for the Portuguese population of PWA. Given the subjectivity of the method used in this study, including sharing experiences and discussion between participants, the sample size should be increased and be more representative of all types of aphasia.
Conclusions
Research has shown that the involvement of PWA is important in the development of assessment tools and in clinical practice but the medical model is still used in Portugal. The use of a panel of experts constituted by PWA, in order to guarantee the integrity of the CDP-EP version 1 in this study, established an adequate and realistic validation that reflects the aims and objectives that need to be considered in the intervention process with PWA. This was achieved not only with the choice of panel of experts, but also and mainly, by adopting the Participatory Workshops method. Hence, this study found that the first version of the CDP-EP is incomplete in the sections of Activity and Participation. Therefore, the proposed suggestions complement the gaps of CDP-EP, aiming to obtain a more final (complete) version of this instrument (version 3). Analysing the characteristics of the sample of this study, and according to the suggestions obtained, it is thought that the level of schooling/ education, life experience, profession (responsibility and social position) and age, influenced critical and analytical thinking.
APH-PA_22-079-File002.docx
Download MS Word (1 MB)Acknowledgments
Support was also received from Portuguese National Funds through the FCT, in the context of the projects UIDB/00127/2020and RISE-LA/P/0053/2020.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Supplemental Material
Supplemental data for this article can be accessed online at https://doi.org/10.1080/02687038.2022.2136483
Notes
1. According to the results of the formal test Bateria de Avaliação de Afasia de Lisboa – BAAL (Caldas, Citation1979; Damásio, Citation1973; Ferro, Citation1986).
References
- Alexandre, N. M. C., & Coluci, M. Z. O. (2011). Validade de conteúdo nos processos de construção e adaptação de instrumentos de medidas. Ciência & Saúde Coletiva, 16(7), 3061–3068. https://doi.org/10.1590/S1413-81232011000800006
- Alliance. (2001). A Facilitators’ Guide to Participatory Workshops with NGOs/CBOs Responding to HIV/AIDS. 1038860, 1–10.
- Andersson, S., & Fridlund, B. (2002). The aphasic person’s views of the encounter with other people: a grounded theory analysis. Journal of Psychiatric and Mental Health Nursing, 9(3), 285–292. https://doi.org/10.1046/j.1365-2850.2002.00480.x
- ASHA. (2022). Clinical Topics: Aphasia. https://www.asha.org/practice-portal/clinical-topics/aphasia/
- Berg, K., Isaksen, J., Wallace, S. J., Cruice, M., Simmons-Mackie, N., & Worrall, L. (2022). Establishing consensus on a definition of aphasia: an e-Delphi study of international aphasia researchers. Aphasiology, 36(4), 385–400. https://doi.org/10.1080/02687038.2020.1852003
- Brennan, A., Worrall, L., & McKenna, K. (2005). The relationship between specific features of aphasia-friendly written material and comprehension of written material for people with aphasia: An exploratory study. Aphasiology, 19(8), 693–711. https://doi.org/10.1080/02687030444000958
- Byng, S., & Duchan, J. F. (2005). Social model philosophies and principles: Their applications to therapies for aphasia. Aphasiology, 19(10–11), 906–922. https://doi.org/10.1080/02687030544000128
- Caldas, A. C. (1979). Diagnóstico e evolução das afasias de causa vascular. Universidade de Lisboa.
- Castro, S., Gomes, I., & Caló, S. (2007). PALPA-P – Provas de Avaliação da Linguagem e da Afasia em Português. CEGOC.
- Charalambous, M., Kambanaros, M., & Annoni, J. M. (2020). Are people with aphasia (PWA) involved in the creation of quality of life and aphasia impact-related questionnaires? A scoping review. Brain Sciences, 10(10), 1–23. https://doi.org/10.3390/brainsci10100688
- Chue, W. L., Rose, M. L., & Swinburn, K. (2010). The reliability of the Communication Disability Profile: A patient-reported outcome measure for aphasia. Aphasiology, 24(6–8), 940–956. https://doi.org/10.1080/02687030903490541
- Dalemans, R. J. P., Witte, L., Wade, D., & Heuvel, W. (2010). Social participation through the eyes of people with aphasia. International Journal of Language & Communication Disorders/Royal College of Speech & Language Therapists, 45(5), 537–550. https://doi.org/10.3109/13682820903223633
- Damásio, A. (1973). Neurologia da Linguagem. Universidade de Lisboa.
- Davis, L. L. (1992). Instrument review: Getting the most from a panel of experts. Applied Nursing Research, 5(4), 194–197. https://doi.org/10.1016/S0897-1897(05)80008-4
- de Vet, H. C. W., Terwee, C. B., Mokkink, L. B., & Knol, D. L. (2011). Measurement in Medicine. Cambridge University Press. https://doi.org/10.1017/CBO9780511996214
- Dorze, G. le, & Brassard, C. (1995). A description of the consequences of aphasia on aphasic persons and their relatives and friends, based on the WHO model of chronic diseases. Aphasiology, 9(3), 239–255. https://doi.org/10.1080/02687039508248198
- Engelter, S. T., Gostynski, M., Papa, S., Frei, M., Born, C., Ajdacic-Gross, V., Gutzwiller, F., & Lyrer, P. A. (2006). Epidemiology of aphasia attributable to first ischemic stroke: Incidence, severity, fluency, etiology, and thrombolysis. Stroke, 37(6), 1379–1384. https://doi.org/10.1161/01.STR.0000221815.64093.8c
- Ferro, J. (1986). Neurologia do comportamento. Estudo da correlação com a tomografia axial computorizada. Universidade de Lisboa.
- Fotiadou, D., Northcott, S., Chatzidaki, A., & Hilari, K. (2014). Aphasia blog talk: How does stroke and aphasia affect a person’s social relationships? Aphasiology, 28(11), 1281–1300. https://doi.org/10.1080/02687038.2014.928664
- Frattali, C. M. (1992). Functional assessment of communication: Merging public policy with clinical views. Aphasiology, 6(1), 63–83. https://doi.org/10.1080/02687039208248577
- Frattali, C. M. (1998). Measuring Outcomes in Speech-language Pathology. Thieme.
- Galliers, J., Wilson, S., Muscroft, S., Marshall, J., Roper, A., Cocks, N., & Pring, T. (2011). Accessibility of 3D Game Environments for People with Aphasia: An Exploratory Study. The Proceedings of the 13th International ACM SIGACCESS Conference on Computers and Accessibility, 139–146. https://doi.org/10.1145/2049536.2049562
- Galliers, J., Wilson, S., Roper, A., Cocks, N., Marshall, J., Muscroft, S., & Pring, T. (2012). Words are not enough. Proceedings of the 12th Participatory Design Conference on Research Papers: Volume 1 - PDC ’12, 51. https://doi.org/10.1145/2347635.2347643
- Garcia, E., & Connor, L. T. (2011). Understanding Barriers and Facilitators to Participation in People with Aphasia a Qualitative Approach. Center for Social Development, Washington University, St. Louis, USA.
- Ghidella, C., Murray, S., Smart, M., McKenna, K., & Worrall, L. (2005). Aphasia websites: An examination of their quality and communicative accessibility. Aphasiology, 19(12), 1134–1146. https://doi.org/10.1080/02687030500337871
- Grant, J. S., & Davis, L. L. (1997). Focus on Quantitative Methods Selection and Use of Content Experts for Instrument Development. Research in Nursing and Health, 20, 269–274.
- Grawburg, M., Howe, T., Worrall, L., & Scarinci, N. (2013). A qualitative investigation into third-party functioning and third-party disability in aphasia: Positive and negative experiences of family members of people with aphasia. Aphasiology, 27(7), 828–848. https://doi.org/10.1080/02687038.2013.768330
- Kagan, A., Black, S. E., Duchan, F. J., SimmonsJ., SimmonsMackie, N., & Square, P. (2001). Training volunteers as conversation partners using “Supported Conversation for Adults with Aphasia” (SCA): a controlled trial. Journal of Speech, Language, and Hearing Research : JSLHR, 44(3), 624638.624638.
- Kagan, A., & Simmons-Mackie, N. (2007). Beginning With the End outcome-Driven Assessment and Intervention With Life Participation in Mind. Topics in Language Disorders, 27(4), 309–317.
- Kanji, N., & Greenwood, L. (2001). Participatory approaches to research and development in IIED: Learning from experience. IED Bookshop, London, UK.
- Kearns, K. P. (1991). Functional Outcome: Methodological Considerations. Proceedings of the Clinical Aphasiology Conference, Destin, FL.
- Lamey, D. (2018). The Evolution of Technology: Past, Present and Future | DiscoverTec. https://www.discovertec.com/blog/evolution-of-technology
- Laska, A. C., Hellblom, A., Murray, V., Kahan, T., & Von Arbin, M. (2001). Aphasia in acute stroke and relation to outcome. Journal of Internal Medicine, 249(5), 413–422. https://doi.org/10.1046/j.1365-2796.2001.00812.x
- Leal, A., Jesus, L. M. T., Gomes, A., Couto, P., & Matos, M. (2014). Aphasia Assessment by the Portuguese Speech and Language Therapists. Revista de Saúde Pública, 48, 291.
- Leal, G. (2006). Avaliação funcional da pessoa com afasia: construção de uma escala. Re(Habilitar), 3, 7–24.
- Leung, S. F., & Arthur, D. (2000). The alcohol use disorders identification test (AUDIT): validation of an instrument for enhancing nursing practice in Hong Kong. International Journal of Nursing Studies, 37(1), 57–64. https://doi.org/10.1016/S0020-7489(99)00052-8
- Martin, N., Thompson, K. C., & Worrall, L. (2008). Aphasia Rehabilitation - The Impairment and its Consequences (2008th ed.). Plural Publishing Group.
- Matos, M. (2012). Níveis de Actividade e Participação das Pessoas com Afasia: Desenvolvimento de Instrumentos de Avaliação Portugueses [Activity and Participation Levels of People With Aphasia: Development of Portuguese Assessment Tools] [ Ph.D. Thesis]. University of Aveiro.
- Matos, M., & Jesus, L. M. T. (2011). Mini-Mental State Modificado (MMSM)(Processo INPI 483183 com despacho de concessão em 3/8/2011, inserido no Boletim da Propriedade Industrial Número 2011/08/08 (150/ 2011); Deferimento pela IGAC em 4/07/2011 – No 3303/2011).
- Matos, M., Jesus, L. M. T., & Cruice, M. (2014). Assessment of aphasia in Portugal: Past, present and future. Stem-, Spraak- En Taalpathologie, 19, 78–83.
- Matos, M., Jesus, L. M. T., Cruice, M., & Gomes, A. A. (2010). Portuguese translation and adaptation of the Communication Disability Profile (CDP) and the Participation Objective, Participation Subjective (POPS) Tools. 28th World Congress of the International Association of Logopedics and Phoniatrics (IALP 2010), July 2014, 60–63.
- Mc Menamin, R., Tierney, E., & mac Farlane, A. (2015). “Who decides what criteria are important to consider in exploring the outcomes of conversation approaches? A participatory health research study.” Aphasiology, 29(8), 914–938. https://doi.org/10.1080/02687038.2015.1006564
- Mohr, W. K., & Tulman, L. J. (2000). Children Exposed to Violence: Measurement Considerations within an Ecological Framework. Advances in Nursing Science, 23(1), 59–68. https://doi.org/10.1097/00012272-200009000-00009
- Murray, L., & Coppens, P. (2013). Formal and Informal Assessment of Aphasia. In Papathanasiou, Ilias, Coppens, Patrick Potagas, Constantin. Aphasia and Related Neurogenic Communication Disorders. Jones &Bartlett Learning.
- Papathanasiou, I., Coppens, P., & Potagas, C. (2011). Aphasia and Related Neurogenic Communication Disorders (Vol. 3). David D. Cella.
- Parr, S. (1994). Coping with aphasia: Conversations with 20 aphasic people. In Aphasiology (Vol. 8). https://doi.org/10.1080/02687039408248670
- Parr, S. (1996). Everyday literacy in aphasia: Radical approaches to functional assessment and therapy. Aphasiology, 10(5), 469–479. https://doi.org/10.1080/02687039608248426
- Parr, S. (2007). Living with severe aphasia: Tracking social exclusion. Aphasiology, 21(1), 98–123. https://doi.org/10.1080/02687030600798337
- Pearl, G., Sage, K., & Young, A. (2011). Involvement in volunteering: an exploration of the personal experience of people with aphasia. Disability and Rehabilitation, 33(19–20), 1805–1821. https://doi.org/10.3109/09638288.2010.549285
- Pierce, R. (1996). Read and write what you want to: What’s so radical? Aphasiology, 10(5), 480–483. https://doi.org/10.1080/02687039608248427
- PORDATA. (2020). pordata. https://www.pordata.pt/Portugal/População+estrangeira+com+estatuto+legal+de+residente+total+e+por+algumas+nacionalidades-24
- Pound, C., Parr, S., Lindsay, J., & Woolf, C. (2002). Beyond aphasia. Therapies for living with communication disability (Oxon UK). Speechmark Publishing Ltd.
- Reis, A., Faísca, L., Ingvar, M., & Petersson, K. M. (2006). Color makes a difference: Two-dimensional object naming in literate and illiterate subjects. Brain and Cognition, 60(1), 49–54. https://doi.org/10.1016/j.bandc.2005.09.012
- Rose, T. A., Worrall, L. E., Hickson, L. M., & Hoffmann, T. C. (2011). Aphasia friendly written health information: content and design characteristics. International Journal of Speech-Language Pathology, 13(4), 335–347. https://doi.org/10.3109/17549507.2011.560396
- Rose, T. A., Worrall, L. E., & McKenna, K. T. (2003). The effectiveness of aphasia-friendly principles for printed health education materials for people with aphasia following stroke. Aphasiology, 17(10), 947–963. https://doi.org/10.1080/02687030344000319
- Rose, T., Worral, L., & McKenna, K. (2003). The effectiveness of aphasia‐friendly principles for printed health education materials for people with aphasia following stroke. Aphasiology, 17(10), 947–963.
- Rose, T., Worrall, L., Hickson, L., & Hoffmann, T. (2010). Do People With Aphasia Want Written Stroke and Aphasia Information? A Verbal Survey Exploring Preferences for When and How to Provide Stroke and Aphasia Information. Topics in Stroke Rehabilitation, 17(2), 79–98. https://doi.org/10.1310/tsr1702-79
- Simmons-Mackie, N., & Damico, J. S. (2007). Access and social inclusion in aphasia: Interactional principles and applications. Aphasiology, 21(1), 81–97. https://doi.org/10.1080/02687030600798311
- Simmons‐Mackie, N., & Kagan, A. (2007). Application of the ICF in Aphasia. Semin Speech Lang, 28(4), 244–253. https://doi.org/10.1055/s-2007-986521
- Simmons-Mackie, N., Kagan, A., Charles Victor, J., Rowland, A. C., Mok, A., Hoch, J. S., Huijbregts, M., & Streiner, D. L. (2014). The assessment for living with aphasia: reliability and construct validity. International Journal of Speech-Language Pathology.
- Spreen, O., & Risser, A. (2003). Assessment of aphasia. Oxford University Press.
- Streiner, D. L., Norman, G. R., & Cairney, J. (2015). Health Measurement Scales (Vol. 1). Oxford University Press. https://doi.org/10.1093/med/9780199685219.001.0001
- Swinburn, K., & Byng, S. (2006). The Communication Disability Profile. Connect - the communication disability network.
- Terwee, C. B., Prinsen, C. A. C., Chiarotto, A., Westerman, M. J., Patrick, D. L., Alonso, J., Bouter, L. M., de Vet, H. C. W., & Mokkink, L. B. (2018). COSMIN methodology for evaluating the content validity of patient-reported outcome measures: a Delphi study. Quality of Life Research, 27(5), 1159–1170. https://doi.org/10.1007/s11136-018-1829-0
- Threats, T. (2008). Use of the ICF for clinical practice in speech-language pathology. International Journal of Speech-Language Pathology, 10(1–2), 50–60. https://doi.org/10.1080/14417040701768693
- WHO. (2001). International Classification of Functioning, Disability and Health (ICF). Geneve: World Health Organization (WHO).
- Worrall, L. (1992). Functional communication assessment: An australian perspective. Aphasiology, 6(1), 105–110. https://doi.org/10.1080/02687039208248581
- Worrall, L., & Cruice, M. (2005). Why the WHO ICF and QOL constructs do not lend themselves to programmatic appraisal for planning therapy for aphasia. A commentary on Ross and Wertz, “Advacing appraisal: Aphasia and the WHO.” Aphasiology, 19, 885–893.
- Worrall, L., & Frattali, C. M. (2011). Neurogenic Communication Disorders: A Functional Approach.
- Worrall, L., McCooey, R., Davidson, B., Larkins, B., & Hickson, L. (2002). The Validity of Functional Assessments of Communication and the Activity/Participation Components of the ICIDH-2: Do They Reflect What Really Happens in Real-Life?. Journal of Communication Disorders, 35(2), 107–137.
- Worrall, L., Papathanasiou, I., & Sherratt, S. (2013). “Therapy approaches to Aphasia.” In I. Papathanasiou, P. Coppens, & C. Potagas (Eds.), Aphasia and Related Neurogenic Communication Disorders (pp. 95–112). Jones & Bartlett Learning.
- Zemva, N. (1999). Aphasic patients and their families: wishes and limits. Aphasiology, 13(3), 219–224. https://doi.org/10.1080/026870399402190