
Abstract
Objective
The current study aims to improve understanding of events leading to lapses of dietary restraint, and to identify pathways to perseverance or abandonment of weight loss efforts in response to lapses. In addition, Behaviour Sequence Analysis (BSA) was also evaluated as an analytical tool in dietary behaviour.
Design
A sample of 176 adults who were engaging in self-imposed dietary restraint for weight loss were recruited to participate.
Main outcome measures
Participants were instructed to provide a detailed written timeline of an episode where they lapsed in their dietary restraint plan. They were instructed to report their preceding behaviours and internal states, and social and environmental contexts, leading up to and after their lapse in dietary restraint.
Results
Lapses in dietary restraint were precipitated by negative internal states in the presence of cues for highly palatable foods. In addition, abandonment of weight loss efforts after lapsing was preceded by dichotomous thinking, whereas perseverance was preceded by a more neutral, flexible interpretation of the lapse in self-control.
Conclusion
BSA has identified that neutral evaluation of inevitable lapses in dietary restraint are predictive of continuation with weight loss efforts, highlighting the importance of individual tolerance of lapses in self-regulation.
1 Introduction
1.1. Background
Rising levels of obesity in Western societies pose a significant burden to public health (Wang et al., 2011). The link between obesity and negative somatic health outcomes have been repeatedly demonstrated (Tanamas et al., Citation2016). Furthermore, a growing body of research has also identified a strong inverse relationship between obesity and mental health (Magallares & Pais-Ribeiro, Citation2014). As a result, for many reducing body mass can often be regarded as a secondary objective, with some individuals being primarily motivated to lose body mass as a means of increasing positive self-regard and reducing body dissatisfaction (Cooper & Fairburn, Citation2001). Given the increasing prevalence of obesity, and the accompanying physical and mental costs, the creation and development of interventions that support individual weight loss and weight-management is a public health priority (Gardner et al., Citation2021).
The principal approach to reducing body mass is engagement of dietary restraint, with an estimated 20% to 50% of females and 5% to 25% of males employing dietary restraint techniques (Slof-Op ‘t Landt et al., 2017). Dietary restraint refers to the conscious decision to restrict food intake and/or restrict consumption of specific food types (Herman & Polivy, Citation1984), which is typically implemented with self-imposed verbal rules that enable an individual to vigilantly observe and maintain a pattern of eating that will lead to weight loss (Ward & Mann, Citation2000). In this context, verbal rules refer to the specification of contingency that is based on language rather than experienced contingency, i.e. reality, and therefore may be arbitrarily determined. For example, an individual attempting to lose body mass may impose a verbal rule such as: “To successfully lose weight I must not consume more than 1500 calories per day.” The verbal rule is considered arbitrary and not definitive because an individual can successfully lose body mass via a multitude of alternative behavioural responses, e.g. consuming 1700 calories on alternate days.
Although such self-imposed verbal rules are not definitively true, often they can be pragmatically true in their application, and may lead to successful outcomes. In a vast majority of cases, such a reduction in energy intake will result in a reduced body mass (Applebaum, Citation2008), particularly when there is a consistent deficit in the number of calories consumed in relation to the individual’s energy expenditure.
However, the effectiveness of self-imposed dietary restraint to reduce body mass is contested in the literature. Although it may seem counter-intuitive prima facie, existing evidence has pointed towards dietary restraint being ineffective for long-term weight loss maintenance (Mann et al., Citation2007). Indeed, Wing and Phelan (Citation2005) conservatively estimate that only 20% of dieters maintain their weight loss results for an extended period. A large body of research has consistently demonstrated that most dieters regain the lost weight in a relatively short time span following dietary restraint (Buchanan et al., Citation2019; Green et al., Citation2009; Hartmann-Boyce et al., Citation2014; Parretti et al., Citation2016). Therefore, if the physical and psychological health benefits of dietary restraint are to be achieved, attention must be focused on understanding why weight loss outcomes are not maintained over the long term (Cooper & Fairburn, Citation2001).
1.2. Maintenance of strict dietary restraint
Although eating behaviour is not an unconscious reflex, behavioural control in eating remains greatly influenced by context, meaning that verbal, social and environmental cues are important in determining lapses in dietary restraint (Gardner et al., Citation2021; Herman & Polivy, 2004). Because of lifestyle restraints and commitments, most adults cannot modulate eating based solely on hunger and satiety cues (Herman & Polivy, 2004). In other words, for many, it is not feasible to stop daily activities to prepare and consume food whenever hunger arises. Therefore, to a large extent eating behaviour must be regulated by verbal rules. It is argued that severely restrictive verbal rules during periods of dietary restraint, requiring substantial vigilance and suppression of impulses, will eventually be abandoned in the context of cues that momentarily deplete self-control (Buchanan et al., Citation2019; Gardner et al., Citation2020, Citation2021). Internal cues that are widely acknowledged to deplete self-control include experiencing negative affect, stress and physical fatigue (Goldstein et al., Citation2018).
Furthermore, evidence consistently shows that creating verbal rules regarding dietary restraint can paradoxically have the effect of increasing the value and desirability of the omitted food (Buchanan et al., Citation2019; Polivy & Herman, Citation2002; Rodgers et al., Citation2018). If vigilance and effort are required to inhibit drives to consume larger amounts of food, or specific food types, then by necessity there will be a learned association between eating forbidden foods (or quantities of food) and relaxation of effort (Gardner et al., Citation2021). Green et al. (Citation2009) have identified that for dieters, so-called junk food consumption is often framed as an opportunity for reward and respite, whereas rigid dietary restraint is framed as an aversive and exhausting internal battle. As a result, when individuals are exposed to contextual cues that momentarily deplete self-control, they are more likely to lapse in their dietary restraint. In sum, the increased drive to consume restricted foods when experiencing inevitable periods of negative affect, will be especially difficult to resist in the context of an obesogenic environment where abundant amounts of highly caloric and palatable foods are available (Larsen, Citation2007). Therefore, arguably, it may be unrealistic to presume that an individual will be able to adhere consistently to a rigid and restrictive eating pattern without occasional lapses (Goldstein et al., Citation2018).
1.3. Implications of lapses in dietary restraint
Given the expectation of occasional lapses in dietary restraint, attention should focus on the relationship between lapses and dietary restraint perseverance and long-term weight loss maintenance. Existing research indicates that repeated lapses in dietary restraint leads to individuals abandoning efforts to lose weight or maintain weight loss (Carels et al., Citation2004; Forman et al., Citation2017), further emphasising the importance of understanding the sequence of events before and following the lapse in dietary restraint. Abandonment of weight loss intentions and behaviours in response to a lapse could be interpreted as excessive and illogical when placed in the context of the preceding successes in diet adherence (Herman & Polivy, 2004). Polivy and Herman (Citation2002) account for this abandonment as a response to the dysphoria and negative affect that individuals experience after lapsing, and the uncomfortable experiences of guilt and negative self-regard that emerge. It is proposed that the negative affect and demoralisation stemming from a lapse is a result of the realisation that one is not meeting self-imposed expectations and intentions, and therefore negatively affecting one’s self concept (Neal & Carey, Citation2004).
Furthermore, evidence shows that an excessive reaction to a lapse in dietary restraint, often referred to as All or Nothing or Dichotomous Thinking, is a robust predictor of abandonment of weight loss efforts (Buchanan et al., Citation2019; Byrne et al., Citation2004; Rodgers, et al., Citation2018). As previously discussed, weight loss is often not the primary goal of dietary restraint but rather a mechanism to improve attractiveness and self-worth (Cooper & Fairburn, Citation2001). Higher levels of body dissatisfaction are reliably associated with more rigid levels of dietary restraint, which in turn increase the probability, if not the inevitability, of relapse (Putterman & Linden, Citation2004; Stice & Shaw, Citation2002). For these individuals, a lapse in dietary restraint may not just be a temporary halt in weight loss progress but perhaps an indicator of their lack of discipline and that they are moving away from their ideal self, and as a result increasing the negative affect experienced (Cooper & Fairburn, Citation2001). Clearly, there is a link between dietary restraint attempts, lapses and abandoning efforts to lose weight. Temporal research into the transition between dietary lapses and post-lapse behaviour is required to clarify the complex processes.
1.4. Application of behaviour sequence analysis
From the above, it is evident that dietary restraint is unlikely to be strictly adhered to over the long-term, and equally, that temporary lapses in dietary restraint are probable, if not inevitable, for most individuals. Given that frequent, temporary lapses in dietary restraint are predictive of abandonment of weight loss intentions, it is important to identify points of significance in the behavioural sequence leading up to dietary lapses. In addition, it is important to identify what behaviours in response to lapses in dietary restraint are predictive of either persevering with, or abandoning, dietary restraint in response. The development of effective interventions for both short-term lapses in dietary restraint, and subsequent complete abandonment of efforts, will be largely dependent on understanding the sequence of internal and external events that precede both.
Behaviour Sequence Analysis (BSA; Clarke & Crossland, Citation1985; Keatley, Citation2018, Citation2020) allows researchers to track the progression of events and behavioursFootnote1 over time. While the method has been used repeatedly in the Social and Forensic Psychology areas, it has not been applied as widely in relation to Health Psychology, with notable exceptions from Townsend and colleagues who have studied self-harm and suicide ideation (Townsend et al., Citation2016). A lot of health-related research focuses on predicting individual outcome behaviours, through multiple factors or predictors; BSA instead highlights the sequential chains that precede and follow certain key behaviours, such as dietary lapses. In terms of the current research, rather than using the traditional approach in psychology, of creating multiple regression models to evaluate which individual factors predict “binge eating” or “abandonment of diet”, BSA allows researchers to see the temporal flow of behavioural and situational events that preceded such dietary lapses. Also, importantly, BSA tracks the post-behaviour outcomes; in this case, how individuals respond emotionally, cognitively and behaviourally to a lapse in dietary restraint. Of course, behavioural sequences leading to a lapse in dietary restraint will ultimately be idiosyncratic at the highly specific contextual level. However, BSA can map the various higher order pathways into and out of a behaviour of interest.
The simplest and most widely-used form of BSA is referred to as lag-one BSA. This effectively means transitions of one step are made. For example, if we see someone report they felt emotion S, “Sad”, and this was followed by a lapse in dietary restraint (e.g., behaviour ECB, “Eat chocolate bar”), then we would see a lag-one BSA of S→ECB. Now, let us imagine the slightly more complex case in which multiple factors might lead to behaviour ECB. For example, alongside Sad (emotion S), someone might feel like they have earned a break from their diet, perhaps by engaging in vigorous physical exercise (behaviour PE). Now, in the dataset we see that many more people suggest that feeling Sad, S, leads to ECB than those who engaged in vigorous physical exercise PE→ECB. From this, we can see frequency scores, indicating more S→ECB transitions than PE→ECB transitions. We could conclude that experience of sadness is more likely to lead to eating a chocolate bar than licensing behaviours (e.g., vigorous physical exercise). This is the basic concept of BSA. Typically, in BSA, standardised residual scores are calculated as these provide a clearer indication of whether a transition between two variables is more likely than chance to occur. A final benefit of the BSA approach is that vast, complex, dynamic relationships between multiple variables can be synthesised into easy-to-follow flow diagrams, called state transition diagrams, which require no specialist training or statistical knowledge to interpret. This has made the method popular with end-users and applied practitioners (Keatley, Citation2020).
Separate predictors of dietary restraint lapses are, of course, informative in analysing behaviour with the goal of intervening and shaping behaviour. BSA attempts to provide greater insight and understanding of the target behaviour, by adding further context to the individual predictive behaviours. Specifically, further contextual understanding of lapses in dietary restraint could be achieved via observing the temporal ordering and relations between separate behaviours. For example, it is widely recognised that “personal stress”, “mental fatigue”, and “lack of self-control” are all related to binge eating (e.g. Goldstein et al., Citation2018). However, by understanding what events or behaviours lead to these risk factors, or indeed what behaviours or events occur between each risk factor and the target behaviour, can provide further insight that may assist in developing effective interventions. This is particularly important if eliminating a risk factor (e.g. stress) for lapsing in dietary restraint is not feasible or advisable for individuals. In this example, it may be more efficacious to identify maladaptive responses to stress that increase probability of lapsing, and to attempt to intervene and eliminate this interim behaviour rather than the experience of stress itself.
1.5. Study aims
There are three primary objectives of the current research study. The analysis aims to improve understanding of:
Behavioural sequences that lead individuals to lapse during periods of self-imposed dietary restraint.
Behavioural sequences that determine whether individuals persevere with, or abandon, dietary restraint in response to a momentary lapse in their self-imposed plan.
The potential value of behaviour sequence analysis as an analytical tool to generate knowledge and understanding in patterns of dietary restraint.
Underlying each of the above objectives is the aim to identify points of significance in the process of self-regulation failure in dieting behaviour. Given the expected high frequency of episodes of lapses in dietary restraint, and the potential abandonment of dietary restraint intentions, it is important to identify points when individuals can be supported with interventions. Identifying the sequence of events that increases probability of abandonment of an initially valued health goal, will aid both individuals and practitioners in creating contingency plans during periods of increased vulnerability.
2. Methodology
2.1. Participants
In total, 176 adultsFootnote2, including 41 males and 135 females, provided an autobiographical timeline to participate in the BSA study. The mean age of participants was 28.97 years (SD = 10.52), with the participants ages ranging from 18 to 66 years. With respect to geographical location, 56.8% of participants were from Great Britain and Ireland, 16.5% were from North America, 15.9% were from Mainland Europe, with 9.7% from Asia. The inclusion criteria for participation were to answer affirmatively to the following question: Have you made an attempt sometime in the last few months to control your food intake in terms of either quantity and/or content with an aim to lose weight or be healthier? Of the sample, 34.7% of participants reported that they intended to engage in dietary restraint for a time-limited period, whereas 65.3% were attempting to implement lifelong practices of dietary restraint.
2.2. Data collection and procedure
Data were collected via an online questionnaire created using QuestionPro software (QuestionPro Inc., 2021). The questionnaire recorded participant demographic details, whether they had recently engaged in dietary restraint and what their intentions were for self-imposing dietary restraint. If participants met the inclusion criteria, they were instructed to provide a detailed written timeline of a single episode in the recent past where they spontaneously lapsed in their dietary restraint plan, and consumed self-restricted food types or quantities. They were instructed to report their preceding behaviours and internal states (including emotions and thought processes), and social and environmental contexts, leading up to and after their lapse in dietary restraint, in sequential order. Participants were encouraged to provide as much detail of their experience as possible.
The questionnaire was posted for a period of 8 weeks on two online survey data collection platforms (SurveyCircle & PollPool), and in addition, the study was also advertised on social media channelsFootnote3. Participants within this convenience sample received no payment for their participation, however aggregated research contribution credits were awarded within SurveyCircle and Poll Pool platforms to reward study participation. The Ethical Review Board at the University of the West of Scotland approved the current study, and the study was completed in line with the 1964 Helsinki declaration on ethical standards for human research.
2.3. Data filtering and coding process
After eight weeks of data collection, in total, the questionnaire was viewed 826 times by potential participants, with 407 individuals beginning the questionnaire. However, only 243 participants completed and submitted the questionnaire; with attrition occurring due to participants either not meeting the inclusion criteria or electing to withdraw from the study during data collection. Of the 243 submitted questionnaires, 176 participants were retained with 67 questionnaires removed from the dataset because of incomplete or unusable data. Participant data were retained for analysis if they submitted a sequential timeline leading up to a lapse in dietary restraint with at least two transitions recorded. The exclusion of participant data was determined by an evaluation of whether the participant fully completed the task outlined in the study (Keatley, Citation2018). Full completion of the research task required participants to provide a detailed timeline of single, recent episode where they lapsed during a period of attempted dietary restraint.
Comprehensive itemisation of individual events into mutually exclusive codes is a pre-requisite for BSA (Bakeman & Quera, Citation2012; Keatley, Citation2018). As a starting point, an initial coding scheme was created based on expected codes extracted from existing dietary restraint research literature. In addition, an initial random sample of ten participant timelines were itemised into individual events by each of the study authors. Factors including internal states, cognitions, social and environmental contexts and cues, and behaviours were considered as individual events to be coded. Any additional codes that emerged from the process were agreed between the three authors and subsequently added to the coding scheme. During the coding process, the coding scheme was updated only if new individual events emerged from the data. Before data coding was initiated, five participant timelines were identified at random, and each author attempted to transform the raw data into event sequences, via application of the agreed coding scheme. To assess inter-rater reliability of the data coding process, emergent sequences of an independently evaluated sub-sample of each other’s coding were compared and agreed between authors before data analyses commenced. Good agreement between authors was established, with any disagreement between authors were settled via discussion.
2.4. Statistical analysis
Participants wrote autobiographical, diary accounts of their dietary behaviours leading-up to and following a lapse in their dietary plans. These qualitative accounts were first parsed into discrete behavioural events and situational events, ensuring that everything was mutually exclusive and coded. Long, detailed qualitative accounts essentially became strings of codes (e.g., A, B, C, D…n; A B D F G…n – where n is any number of codes that follow). The initial analyses were a frequency count of each individual code, that represents a behavioural event or a situational event. This gives an initial overview of how many individual codes occurred throughout the dataset. The next and more important stage was to calculate the lag-one transitions between codes for each participant. For example, how many times does A→B; B→C; C→D transitions occur in the dataset. Transition frequencies for the entire sample were then calculated and put into a transition frequency matrix, where rows are the antecedent initial behaviour in a transition pair, and columns were the sequitur, following behaviour in a lag-one transition pair.
Transition frequencies are fairly informative, but they can be biased towards behaviours that occur multiple times in the dataset occurring in sequence by chance. For example, if we imagine that we coded “X: blinks” and “Y: breaths in” and “Z breaths out” in our dataset, then we would expect X→Y, Y→Z and even X→Z to occur multiple times, by chance. They are frequently occurring, but they do not offer much information. Therefore, in BSA, standardised residual (SR) scores are calculated to show which transitions are occurring above the level expected by chance. Thus, high SR scores indicate that the transition is occurring more than we could expect by chance.
The final step of BSA is to provide data in a way that is useful for end-users. The transition frequency matrices with SR scores are typically extensively long and prohibitively complex to non-academic audiences. Rows and columns can spread across pages and following meaningful pathways is difficult. Therefore, the information is typically plotted in a flow diagram, called a state transition diagram. These diagrams plot the transitions between situational events and behavioural events that are occurring above the level of chance. They are simple flow diagrams that require no advanced statistical awareness and are typically enjoyed by practitioners and non-academic audiences. It should be remembered, however, that though the diagram is plotted as a long flow diagram, the analyses are lag-one. This means that although the diagram makes it look like longer chains are occurring (e.g., A→B→C), this is not the case. The diagram should be read and understood in pairs (e.g., A→B; B→C and so on). It is possible to perform higher order analyses to investigate longer chains; but it is typically advised against in the research literature (see Keatley, Citation2020). All analyses were conducted in a R script, however other statistical packages such as SPSS and Python can also be used to conduct BSA.
3. Results
The first stage of Behaviour Sequence Analysis is to report the frequencies of individual behavioural events and situational events. This provides an initial insight into trends observed within the data. shows the number of times participants responded that they experienced various factors associated with their self-imposed attempts at dietary restraint. Some of the most frequently occurring factors were: Negative affect from lapse (n = 53); Felt dejected (n = 41); Discounted and justified lapse (n = 39); and Stressed from work (n = 31). The individual factors are presented to show support for previous literature and indicate that the current dataset comprises behavioural events and situational events one would expect to see in this research.
Table 1. Frequency of individual behavioural and situational events.
3.1. Behaviour sequence analysis
The more valuable part of BSA research is to understand not only what occurs, but the order or sequence in which it occurs. In isolation, frequency counts can often be misleading and may not offer the best analyses of the data (Keatley, Citation2018, Citation2020), therefore Chi-Square analyses were conducted on the transition frequency matrix to ascertain the standardised residuals (SRs). Once SRs were calculated, they were then plotted into a state transition diagram, which allows the transitions between events to be more easily understood (see ). To read the diagram, audiences are instructed that thicker lines indicate higher SR scores, which means those transitions are occurring significantly more than we would expect by chance. For example, a strong transition was observed between ‘Planned a break in dietary restraint’ to ‘Offsetting behaviour’ (n = 2, SR = 13.68), though the raw frequency of this transition was low (n = 2), it occurred above the level expected by chance. Both raw transition frequencies and standardised residuals are presented to permit evaluation of state-transition significance and commonality separately.
Figure 1. Behavioural sequence analysis of pathways to and from lapses in dietary restraint.
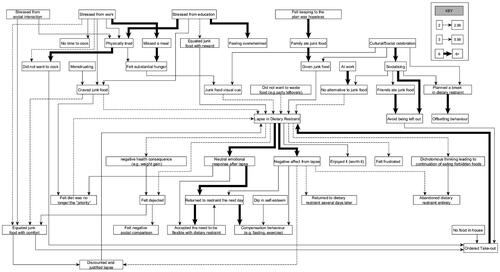
It is important to note that within BSA research studies less emphasis is placed on raw frequencies of specific transitional pairs in contrast to the consistency of pairings (Keatley, Citation2018). To demonstrate with an example, if in the data behaviour A was observed to precede behaviour B a total of 15 times (n = 15), and behaviour B represented only 20% of all behaviours that were observed to immediately follow behaviour A. In addition, within the same dataset, behaviour C was immediately followed by behaviour D on just four occasions (n = 4) and it was observed that D represented all of the observed behaviours in the dataset that immediately followed C. In this example, more theoretical emphasis is likely to be placed on the consistency of the C→D transition in comparison to the A→B transition, despite overall having a lower observed frequency. Ultimately, raw frequencies of observed transitional pairs do not in themselves determine theoretical importance. Rather, theoretical importance in BSA studies is determined based on the consistency of transitional pairings that are evaluated to be highly contextually related to the target behaviour or process (please see Keatley, Citation2018 for further explanation).
Given the potential excessive complexity of BSA, researchers often attempt to reduce the complexity in the diagrams by increasing the cut-off criteria for presentation (Ellis et al., 2018). In the present results, only those transitions that had a frequency above two and a standardised residual above two were plotted. This is simply to make the diagram more interpretable. The importance of specific state–transition pairs was determined via its SR magnitude and evaluations of their theoretical relevance to the overall research question.
Experience of negative internal states was observed to be one of the most prominent factors in lapses of dietary restraint. It was evident that a negative internal state, in combination with exposure to social and environmental cues of restricted and desirable foods were common pathways to dietary lapses. For example, ‘Felt dietary restraint was hopeless’ was associated with ‘Family ate junk food’ (n = 2, SR = 12.46), which itself was strongly connected to Given junk food (n = 2, SR = 6.45). Being Given junk food was an antecedent of lapse in dietary restraint (n = 9, SR = 3.79). More specifically, experience of stress from work and from education was observed to precede being Physically tired (n = 5, SR = 5.18 and n = 5, SR = 6.26, respectively); which in turn was an antecedent for Did not want to cook (n = 6, SR = 8.63). This is an important observation because not wanting to cook was observed to be closely associated with Ordered take-out (n = 4, SR = 4.78), which was associated with Lapse in dietary restraint (n = 25, SR = 6.85). Put simply, it appears that temporarily disengaging from dietary restraint could be triggered initially by experiencing the negative internal state of stress, leading to fatigue and behaviours related to more immediate gratification.
Conversely, probable positive internal states stemming from engaging in celebrations with family and friends, or socialising in general, were factors commonly observed in pathways leading to dietary lapse. Observing family and friends eating restricted but desirable food, and being offered such food by others, and also not wanting to feel left out of the social event, were all frequently reported factors in the pathway leading to a lapse in dietary restraint. It is clear from the pathways outlined in that a positive social context increases the probability of an individual temporarily abandoning weight loss or weight management efforts.
In addition, the environmental context, via a myriad of pathways, appeared to be a central factor leading up to a lapse in dietary restraint. One of the strongest transitions was At work to No alternative to junk food (n = 2, SR = 15.33). Essentially, participants consumed foods that were forbidden by their self-determined verbal rules when they were in a context where there were no available alternatives. Furthermore, the BSA identifies that often the final step in the sequence leading to a lapse in dietary restraint was being exposed to a Junk food visual cue or being Given junk food. In other words, it is evident that immediate availability of restricted foods was predictive of reduced self-control.
As well as identifying pathways leading to dietary lapses, it was important to identify different pathways that emerge in response to a lapse in dietary restraint. One of the most frequently occurring transitions was between Lapse in dietary restraint to Negative affect from lapse (n = 46, SR = 11.74). It was evident that a participant did not Abandon dietary restraint entirely, unless they first experienced Negative affect from lapse or engaged in Dichotomous thinking leading to continuation of eating forbidden foods. Alternatively, Returned to restraint the next day was strongly associated with not feeling guilt after lapsing (Neutral emotional response after lapse: n = 22, SR = 7.) and Accepted the need to be flexible with dietary restraint (n = 11, SR = 1.48). Therefore, whether a participant was able to return to dietary restraint after a lapse appeared to be determined by how they emotionally and cognitively responded to their lapse. If the participant was able to put the lapse of self-control in eating in its appropriate perspective, it was probable that they would soon return to their weight loss or weight management behaviours.
4. Discussion
Irrespective of its disputed efficacy, dietary restraint, characterised as adhering to self-devised verbal rules that regulate eating behaviour, is a prevalent method of weight loss and maintenance within the general populous (Ward & Mann, Citation2000). Hitherto, research has focused upon the role of dietary restraint in food-based decision making, potential differences among varying demographic and individual social cognitive factors and its role in eating pathology (Bublitz et al., Citation2010; Linardon et al., Citation2018; Manasse et al., Citation2018; Scott et al., Citation2008). However, no study to date has comprehensively investigated the temporal nature of the archetypal transitions before dietary lapses or even post-lapse behaviour in a non-clinical dieting population. Examining such is not only important to identify points of significance in the behavioural sequence leading up to, and following, dietary lapses but also helps better inform implementation intentions (or action plans). Implementation plans in this context are designed to improve dietary restraint, and more importantly, avoid subsequent abandonment of efforts upon a temporary violation. By employing the novel use of BSA, this study had three aims: a) to identify common pathways that lead to lapsing on dietary restraint; b) to identify the salient pathways that result from lapsing on dietary restraint; and c) to evaluate the potential contribution of a BSA approach to understanding weight loss, and weight management, behaviour.
4.1. Pathways to lapses in dietary restraint
It is evident from the BSA that lapses in dietary restraint are often precipitated by a negative internal state early in the sequence, such as experiencing various forms of stress (work, education, and social) and emotional discomfort. This may seem axiomatic to the reader, as stressors have been reliably found to impair self-control (Maier et al., Citation2015), increase consumption of calorie dense foods that are high in fat and sugar (Torres & Nowson, Citation2007) and decrease vegetable intake (O’Connor et al., 2008). There is some evidence, albeit inconsistent, to suggest that restrained eaters are significantly more likely to experience a momentary hyperphagic response following an acute exposure to stress (Heatherton & Baumeister, Citation1991; Lattimore & Maxwell, Citation2004); even beyond that of higher levels of perceived stress alone (Wardle et al., Citation2000). It is possible that this is due to restrained eaters being less responsive to their internal state of hunger, perhaps due to habituation of the sensation, and thus may be more likely to overeat (Heatherton et al., Citation1989).
What is particularly striking from the BSA is that stress appeared to lead to not only unpleasant psychological states, but also consequently resulted in negative psychosomatic experiences such as fatigue. Individual’s post-stress feelings of fatigue appeared to be an important factor leading to a reduction in dietary restraint via experiencing abnormally high levels of hunger and thus, becoming less resistant to environmental cues for foods that they were trying to eliminate or restrict. In addition, the BSA revealed that there was a lack of willingness to engage in behaviours that may be central to maintaining control, such as preparing a meal upon the emergence of feelings of fatigue. The highlighting of somatic (as well as mental) fatigue as the symptom of stress-induced eating should be examined further. For, despite the association between fatigue and stress, little research has been conducted into the role of mental and somatic fatigue on eating behaviour directly.
The current findings demonstrate support not only for a client-focused approach to dietary intervention plans, but also an appreciation of the temporal-sensitive nature of likely lapses to ensure the retention of such plans. For instance, many dietary intervention plans will integrate other components, such as action planning, to pro-actively determine an appropriate response to a known cue or stimuli that leads to an undesirable behaviour ahead of time (Michie et al., Citation2013). However, it has been observed that creating such plans or proactive rules have limited success particularly when the negative habitual response is so strong (Adriaanse et al., Citation2011). This is further compounded given that evading undesirable health behaviours are more difficult than engaging in health promoting behaviours (Adriaanse et al., Citation2011; Hagger & Luszczynska, Citation2014). What the current BSA project has demonstrated here is that interventions, and their parallel implementation intention, may be better directed towards an individual’s time-specific somatic and behavioural responses experienced in response to their trigger; rather than the trigger per say. For instance, if the individual is able to recognise that they are specifically vulnerable to a dietary lapse when fatigued due to substantial hunger, they can seek to quickly reduce the sensation of hunger to increase the probability of maintaining self-control. Evidence demonstrates that individuals who can engage in Action Planning, and repeatedly replace an undesirable response with an adaptive response that is functionally equivalent (in this example, eliminating discomfort from hunger) are more likely to successfully transform behaviour over the long-term (Gardner et al., Citation2021).
Interpreting the BSA output further in relation to existing literature, there is scope to propose that identifying foods that must not be consumed, and engaging in effortful vigilance and inhibition, may by default make these individuals associate lapsing on dietary restraint with reward and comfort (Gardner et al., Citation2021; Schaumberg et al., Citation2016; Stice, Citation2001). The effect of associating forbidden foods with relaxation of effort, reward and comfort is likely to increase its desirability for individuals who are experiencing somatic and psychological discomfort from stress or fatigue, and therefore increase motivation for consumption. The indirect pairing of eating restricted food types with reward and relaxation of effort, is likely to increase the salience of consuming such foods in response to agreeable social and leisure contexts. With respect to reducing the probability of lapsing on dietary restraint when engaging in social events and when feeling stressed and fatigued, it may be prudent to directly attempt to dissociate restricted food consumption with reward and comfort via clinical intervention. In other words, behavioural interventions could be implemented to directly associate junk food consumption with an aversive stimuli (e.g. an experience of discomfort) in order to minimise the salience of the problematic association of junk food consumption and reward/comfort during periods of negative internal states.
4.2. Pathways emerging from lapses in dietary restraint
Previous literature, and the current findings, both indicate that lapses in dietary restraint are to be expected given the inevitability of experiencing of negative affective and somatic states such as stress and fatigue, and its impact on maintaining inhibitory control (Gardner et al., Citation2021; Goldstein et al., Citation2018). Therefore, arguably, when attempting to develop interventions to support weight loss perseverance and maintenance, attention should focus on understanding adaptive and maladaptive responses to the inevitable lapses. Understanding what leads an individual to abandon dietary restraint entirely in response to a lapse, as opposed to returning to their self-imposed weight loss plan the following day, would appear to be a critical task.
The current findings support existing literature in identifying that the key determinant of whether a single lapse leads to complete abandonment of weight loss attempts is how the individual emotionally and cognitively responds to the loss of self-control. In the current study, participants did not abandon their weight loss efforts unless they first experienced a negative emotional response or engaged in dichotomous thinking behaviour, interpreting the single lapse as eliminating all previous and future dietary successes.
The BSA also revealed that when individuals pre-plan a dietary break, typically in response to a planned social event, they were likely to engage in offsetting or “pre-compensation” (Lenne et al., Citation2017). These included actions such as fasting and exercise, to mitigate any negative consequences emerging from the planned lapse. This was also characterised by a more positive cognitive and emotional framing of the dietary lapse and, subsequently, the likelihood of the reinstating the initial dietary plan. Given that not experiencing negative emotion after lapsing was linked to returning to dietary restraint the next day and not abandoning weight-loss efforts entirely, it may be prudent for individuals to plan and accept a temporal lapse when it is known to be highly probable based on past behaviour (e.g., Thanksgiving). If pre-determined breaks in restraint are associated with positive emotional framing of the lapse, this reduces the probability of the individual abandoning weight-loss attempts entirely after inevitable occasional slips. In addition, social events, particularly cultural celebrations such as Christmas, are often not spontaneous events, and therefore there is an opportunity to pre-plan adaptive contingencies. Regardless of whether the pre-planned responses to probable dietary lapses involve pre-compensation behaviours, reducing probable hunger by making permitted alternatives available, or simply accepting that restraint will be temporarily suspended, such premeditated behaviours are likely to moderate post-lapse negative internal states.
Existing literature has also identified dichotomous thinking in response to lapses as a salient predictor of giving up on weight loss efforts completely (Byrne et al., Citation2004; Rodgers et al., Citation2018). In contrast, individuals who were able to put the single lapse in perspective with previous successes and accept that an occasional lapse in dietary restraint is to be expected, were much more likely to return to dietary restraint the following day. This finding supports existing literature, indicating the importance of flexible interpretation and responses to lapses in self-control, rather than using an ‘all or nothing’ evaluative frame (Buchanan et al., Citation2019; Cooper & Fairburn, Citation2001). As a result, a potential point of intervention to support perseverance in weight loss attempts after inevitable lapses, would be in assisting clients to minimise dichotomous thinking interpretations and promote and encourage flexible responding in this context.
4.3. Future research and limitations of BSA
The emergent findings demonstrating that negative affective states, and environmental and social stimuli are important predictors of lapses in self-regulation of eating is not particularly revelatory. There is a large body of research demonstrating that self-control is more likely to be relaxed when an individual is stressed or fatigued, in the context of social facilitation and an obesogenic environment with immediate availability of highly palatable, calorically dense food (Buchanan et al., Citation2019; Goldstein et al., Citation2018; Larsen, Citation2007). However, BSA has successfully organised these factors into coherent sequential temporal pairs, and therefore, identified the most salient pathways to and from the target variable of dietary lapse. BSA also highlights the most salient points of transition in each observed pathway. This is valuable because by identifying the most consistently paired behaviours or events in a sequential process, it is possible to identify points of critical significance that may be effective target points for intervention.
For example, current findings demonstrate a strong association between fatigue and not wanting to prepare a meal, in the pathway leading to lapses in dietary restraint. Therefore, when attempting to reduce the probability of lapsing, individuals may benefit from taking pre-planned action when feeling fatigued, mitigating the consequence of not wanting to prepare a meal. Such pre-planned actions are likely to differ vastly dependent on specific environmental and individual contexts. However, an example of a mitigation strategy here could include being readily aware of where one could order Take-Out food that would not violate self-imposed restrictions, or having microwaveable meals in the freezer that largely negate effortful meal preparation.
The value of BSA research is the identification of upstream factors, organised in a hierarchy of importance, that could be targeted within behavioural modification processes. Furthermore, as the homogeneity of the sample increases, it is probable that the sequential pathways observed and the critical points for intervention and action planning will become clearer and more robust. A limitation of the current study has been the lack of narrow inclusion criteria for participation beyond simply being an adult who has recently lapsed in dietary restraint attempts, drawn from an online convenience sample. Therefore, the observed pathways and the relative importance of points of transition is reflective of a diverse set of individuals who could be either obese or not, or who may have had very prescriptive dietary restrictions or were holding much more ambiguous dietary intentions, for example. It is probable that pathways towards, and from, lapses in dietary restraint are likely to vary substantially between individuals within different individual contexts. In this regard, now that the potential value of BSA as an analytical mechanism has been demonstrated, future research should apply BSA techniques within more narrow populations. In particular, BSA could have applied value in better understanding the psychological processes involved in the common phenomenon in a narrow sample of previously obese individuals who were initially successful in losing weight, abandoning dietary restraint and return to previous or higher levels of weight.
Given the expected extensive variance in pathways to lapsing in dietary restraint, because of vastly different contextual factors and individual differences within any given sample, perhaps the most effective application of BSA in this domain will be at the level of the individual. A further limitation of the current study is that data were only available in relation to a single episode of dietary lapse for each participant (i.e., their most recent lapse). It is probable that each individual may have multiple behavioural pathways that lead to lapses in dietary restraint, further reinforcing the potential value of observing behaviour across an extended time period, at an individual level. A restrictive factor in the application of BSA at the individual level will be the sheer amount of data required to run analyses from a statistical power perspective. A potential solution to the demand for substantial amounts of data required per individual could be the use of Ecological Momentary Assessment (EMA) digital techniques to record associations between internal states, environmental and social contexts and eating behaviour in a minimally invasive way. Holmes et al. (Citation2014) and Rodgers et al. (Citation2018) successfully demonstrated that such associations between internal states and restrictive and binge eating behaviours could be effectively assessed via EMA methods, even across one seven-day data collection period. With sufficient data, EMA techniques would greatly assist in creating individually tailored supportive interventions.
Furthermore, although emphasis in interpreting the BSA outcomes has been placed on the standardised residuals of consistent pairs of behaviours and events rather than the absolute frequency counts, it is important to note that several of the transitional pairs had relatively low absolute frequencies. Therefore, it would be advisable to replicate the study using variant populations to evaluate consistency of transitional pairings identified and consider the representativeness of the findings of the current study. Despite further investigation being recommended, the current BSA study has provided a foundation in which to build on understanding between the risk factors for violating dietary plans either temporarily and perhaps even indefinitely. It is hoped that this will act as a springboard to further exploration into the complexity of eating behaviours and inform effective intervention plans.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Disclosure statement
The authors declare that they have no conflict of interest.
Funding
The author(s) reported there is no funding associated with the work featured in this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Notes
1 In this context, cognitions are categorised as verbal behaviours (Skinner, Citation1957)
2 Presently, there is no power analysis for BSA research (Keatley, Citation2018). In existing literature samples range from n- of −1 through to >100. The current sample was determined based on agreed of saturation where new participants were no longer added new substantive concepts.
3 Individual researchers’ Twitter and University of [removed for blind review] Facebook accounts.
References
- Adriaanse, M. A., Van Oosten, J. M., De Ridder, D. T., De Wit, J. B., & Evers, C. (2011). Planning what not to eat: Ironic effects of implementation intentions negating unhealthy habits. Personality & Social Psychology Bulletin, 37(1), 69–81. https://doi.org/10.1177/0146167210390523
- Adriaanse, M. A., Vinkers, C. D., De Ridder, D. T., Hox, J. J., & De Wit, J. B. (2011). Do implementation intentions help to eat a healthy diet? A systematic review and meta-analysis of the empirical evidence. Appetite, 56(1), 183–193.
- Applebaum, M. (2008). Why diets fail-expert diet advice as a cause of diet failure. The American Psychologist, 63(3), 200–201. https://doi.org/10.1037/0003-066X.63.3.200
- Bakeman, R., & Quera, V. (2012). Sequential analysis and observational methods for the behavioral sciences. Cambridge: Cambridge University Press.
- Buchanan, K., Sheffield, J., & Tan, W. H. (2019). Predictors of diet failure: A multifactorial cognitive and behavioural model. Journal of Health Psychology, 24(7), 857–869. https://doi.org/10.1177/1359105316689605
- Bublitz, M. G., Peracchio, L. A., & Block, L. G. (2010). Why did I eat that? Perspectives on food decision making and dietary restraint. Journal of Consumer Psychology, 20(3), 239–258. https://doi.org/10.1016/j.jcps.2010.06.008
- Byrne, S. M., Cooper, Z., & Fairburn, C. G. (2004). Psychological predictors of weight regain in obesity. Behaviour Research & Therapy, 42(11), 1341–1356. https://doi.org/10.1016/j.brat.2003.09.004
- Carels, R. A., Douglass, O. M., Cacciapaglia, H. M., & O’Brien, W. H. (2004). An ecological momentary assessment of relapse crises in dieting. Journal of Consulting & Clinical Psychology, 72(2), 341–348. https://doi.org/10.1037/0022-006X.72.2.34
- Clarke, D. D., & Crossland, J. (1985). Action systems: An introd. to the analysis of complex behaviour. London: Methuen.
- Cooper, Z., & Fairburn, C. G. (2001). A new cognitive behavioural approach to the treatment of obesity. Behaviour Research & Therapy, 39(5), 499–511. https://doi.org/10.1016/S0005-7967(00)00065-6
- Ellis, H. E., Clarke, D., & Keatley, D. (2017). Perceptions of behaviours in stranger rape cases: A sequence analysis approach. Journal of Sexual Aggression, 23(3), 328–337. https://doi.org/10.1080/13552600.2017.1361618
- Forman, E. M., Schumacher, L. M., Crosby, R., Manasse, S. M., Goldstein, S. P., Butryn, M. L., Wyckoff, E. P., & Graham Thomas, J. (2017). Ecological momentary assessment of dietary lapses across behavioral weight loss treatment: Characteristics, predictors, and relationships with weight change. Annals of Behavioral Medicine: A Publication of the Society of Behavioral Medicine, 51(5), 741–753. https://doi.org/10.1007/s12160-017-9897-x
- Gardner, B., Lally, P., & Rebar, A. L. (2020). Does habit weaken the relationship between intention and behaviour? Revisiting the habit–intention interaction hypothesis. Social & Personality Psychology Compass, 14(8), Article, e12553. https://doi.org/10.1111/spc3.12553
- Gardner, B., Richards, R., Lally, P., Rebar, A., Thwaite, T., & Beeken, R. J. (2021). Breaking habits or breaking habitual behaviours? Old habits as a neglected factor in weight loss maintenance. Appetite, 162, 105183–105187. https://doi.org/10.1016/j.appet.2021.105183
- Goldstein, S. P., Dochat, C., Schumacher, L. M., Manasse, S. M., Crosby, R. D., Thomas, J. G., Butryn, M. L., & Forman, E. M. (2018). Using ecological momentary assessment to better understand dietary lapse types. Appetite, 129(129), 198–206. https://doi.org/10.1016/j.appet.2018.07.003
- Green, A. R., Larkin, M., & Sullivan, V. (2009). Oh stuff it! The experience and explanation of diet failure: An exploration using interpretative phenomenological analysis. Journal of Health Psychology, 14(7), 997–1008. https://doi.org/10.1177/1359105309342293
- Hagger, M. S., & Luszczynska, A. 1. (2014). Implementation intention and action planning interventions in health contexts: State of the research and proposals for the way forward. Applied Psychology: Health & Well‐Being, 6(1), 47.
- Hartmann-Boyce, J., Johns, D. J., Jebb, S. A., Summerbell, C., & Aveyard, P, Behavioural Weight Management Review Group (2014). Behavioural weight management programmes for adults assessed by trials conducted in everyday contexts: Systematic review and meta-analysis. Obesity Reviews: An Official Journal of the International Association for the Study of Obesity, 15(11), 920–932. https://doi.org/10.1111/obr.12220
- Heatherton, T. F., & Baumeister, R. F. (1991). Binge eating as escape from self-awareness. Psychological Bulletin, 110(1), 86–108.
- Heatherton, T. F., Polivy, J., & Herman, C. P. (1989). Restraint and internal responsiveness: Effects of placebo manipulations of hunger state on eating. Journal of Abnormal Psychology, 98(1), 89–92.
- Herman, C. P., & Polivy, J. (1984). Boundary model for the regulation of eating. Research publications – Association for Research in Nervous & Mental Disease, 62, 141–156.
- Herman, C. P., & Polivy, J. (2011). The self-regulation of eating: Theoretical and practical problems. In K. D. Vohs & R. F. Baumeister (Eds.), Handbook of self-regulation: Research, theory, and applications (pp. 522–536). Guilford Press.
- Holmes, M., Fuller-Tyszkiewicz, M., Skouteris, H., & Broadbent, J. (2014). Improving prediction of binge episodes by modelling chronicity of dietary restriction. European Eating Disorders Review: The Journal of the Eating Disorders Association, 22(6), 405–411.
- Keatley (2018). Pathways in crime: An introduction to behaviour sequence analysis. Palgrave Macmillan. https://doi.org/10.1007/978-3-319-75226-6
- Keatley (2020). The timeline toolkit: Temporal methods for crime research. ReBSA Publications.
- Larsen, J. K., van, S. T., Eisinga, R., Herman, C. P., & Engels, R. C. (2007). Dietary restraint: Intention versus behavior to restrict food intake. Appetite, 49(1), 100–108. https://doi.org/10.1016/j.appet.2006.12.005
- Lattimore, P., & Maxwell, L. (2004). Cognitive load, stress, and disinhibited eating. Eating Behaviors, 5(4), 315–324.
- Lenne, R. L., Panos, M. E., Auster-Gussman, L., Scherschel, H., Zhou, L., & Mann, T. (2017). Behavioral compensation before and after eating at the Minnesota State Fair. Appetite, 118, 113–119.
- Linardon, J., Phillipou, A., Newton, R., Fuller-Tyszkiewicz, M., Jenkins, Z., Cistullo, L. L., & Castle, D. (2018). Testing the relative associations of different components of dietary restraint on psychological functioning in anorexia nervosa and bulimia nervosa. Appetite, 128, 1–6. https://doi.org/10.1016/j.appet.2018.05.138
- Maier, S. U., Makwana, A. B., & Hare, T. A. (2015). Acute stress impairs self-control in goal-directed choice by altering multiple functional connections within the brain’s decision circuits. Neuron, 87(3), 621–631. https://doi.org/10.1016/j.neuron.2015.07.005
- Magallares, A., & Pais-Ribeiro, J. L. (2014). Mental health and obesity: A meta-analysis. Applied Research in Quality of Life, 9(2), 295–308. https://doi.org/10.1007/s11482-013-9226-x
- Manasse, S. M., Schumacher, L. M., Goldstein, S. P., Martin, G. J., Crosby, R. D., Juarascio, A. S., Butryn, M. L., & Forman, E. M. (2018). Are individuals with loss-of-control eating more prone to dietary lapse in behavioural weight loss treatment? An ecological momentary assessment study. European Eating Disorders Review: The Journal of the Eating Disorders Association, 26(3), 259–264. https://doi.org/10.1002/erv.2583
- Mann, T., Tomiyama, A. J., Westling, E., Lew, A.-M., Samuels, B., & Chatman, J. (2007). Medicare’s search for effective obesity treatments: Diets are not the answer. The American Psychologist, 62(3), 220–233. https://doi.org/10.1037/0003-066X.62.3.220
- Michie, S, Richardson, M, Johnston, M, Abraham, C, Francis, J, Hardeman W, Eccles MP, Cane J, Wood CE. (2013 Aug). The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: building an international consensus for the reporting of behavior change interventions. Annals of Behavioral Medicine, 46(1), 81–95. https://doi.org/10.1007/s12160-013-9486-6. PMID: 23512568.
- Neal, D. J., & Carey, K. B. (2004). Developing discrepancy within self-regulation theory: Use of personalized normative feedback and personal strivings with heavy-drinking college students. Addictive Behaviors, 29(2), 281–297. https://doi.org/10.1016/j.addbeh.2003.08.004
- O’Connor, D. B., Jones, F., Conner, M., McMillan, B., & Ferguson, E. (2008). Effects of daily hassles and eating style on eating behavior. Health Psychology: Official Journal of the Division of Health Psychology, American Psychological Association, 27(1S), S20–S31. S20. https://doi.org/10.1037/0278-6133.27.1.S20
- Parretti, H. M., Jebb, S. A., Johns, D. J., Lewis, A. L., Christian-Brown, A. M., & Aveyard, P. (2016). Clinical effectiveness of very-low-energy diets in the management of weight loss: A systematic review and meta-analysis of randomized controlled trials. Obesity Reviews: An Official Journal of the International Association for the Study of Obesity, 17(3), 225–234. https://doi.org/10.1111/obr.12366
- Polivy, J., & Herman, C. P. (2002). If at first you don’t succeed: False hopes of self-change. The American Psychologist, 57(9), 677–689. https://doi.org/10.1037/0003-066X.57.9.677
- Putterman, E., & Linden, W. (2004). Appearance versus health: Does the reason for dieting affect dieting behavior? Journal of Behavioral Medicine, 27(2), 185–204. https://doi.org/10.1023/B:JOBM.0000019851.37389.a7[Mismatch]
- Rodgers, R. F., Fuller-Tyszkiewicz, M., Holmes, M., Skouteris, H., & Broadbent, J. (2018). When does behavior follow intent? Relationships between trait level dietary restraint and daily eating behaviors. Appetite, 120(120), 449–455. https://doi.org/10.1016/j.appet.2017.09.030
- Schaumberg, K., Anderson, D. A., Anderson, L. M., Reilly, E. E., & Gorrell, S. (2016). Dietary restraint: What’s the harm? A review of the relationship between dietary restraint, weight trajectory and the development of eating pathology. Clinical Obesity, 6(2), 89–100. https://doi.org/10.1111/cob.12134
- Scott, M. L., Nowlis, S. M., Mandel, N., & Morales, A. C. (2008). The effects of reduced food size and package size on the consumption behavior of restrained and unrestrained eaters. Journal of Consumer Research, 35(3), 391–405. https://doi.org/10.1086/591103
- Skinner, B. F. (1957). Verbal behavior. Appleton Century Crofts. https://doi.org/10.1037/11256-000
- Slof-Op ‘t Landt, M. C. T., van Furth, E. F., van Beijsterveldt, C. E. M., Bartels, M., Willemsen, G., de Geus, E. J., Ligthart, L., & Boomsma, D. I. (2017). Prevalence of dieting and fear of weight gain across ages: A community sample from adolescents to the elderly. International Journal of Public Health, 62(8), 911–919. https://doi.org/10.1007/s00038-017-0948-7
- Stice, E. (2001). A prospective test of the dual-pathway model of bulimic pathology: Mediating effects of dieting and negative affect. Journal of Abnormal Psychology, 110(1), 124–135. https://doi.org/10.1037/0021-843X.110.1.124
- Stice, E., & Shaw, H. E. (2002). Role of body dissatisfaction in the onset and maintenance of eating pathology: A synthesis of research findings. Journal of Psychosomatic Research, 53(5), 985–993. https://doi.org/10.1016/S0022-3999(02)00488-9
- Tanamas, S. K., Ng, W. L., Backholer, K., Hodge, A., Zimmet, P. Z., & Peeters, A. (2016). Quantifying the proportion of deaths due to body mass index- and waist circumference-defined obesity: Mortality attributable to obesity. Obesity (Silver Spring, Md.), 24(3), 735–742. https://doi.org/10.1002/oby.21386
- Torres, S. J., & Nowson, C. A. (2007). Relationship between stress, eating behavior, and obesity. Nutrition (Burbank, Los Angeles County, Calif.), 23(11-12), 887–894. https://doi.org/10.1016/j.nut.2007.08.008.
- Townsend, E., Wadman, R., Sayal, K., Armstrong, M., Harroe, C., Majumder, P., Vostanis, P., & Clarke, D. (2016). Uncovering key patterns in self-harm in adolescents: Sequence analysis using the Card Sort Task for Self-harm (CaTS). Journal of Affective Disorders, 206, 161–168. https://doi.org/10.1016/j.jad.2016.07.004
- Wang, Y. C., McPherson, K., Marsh, T., Gortmaker, S. L., & Brown, M. (2011). Health and economic burden of the projected obesity trends in the USA and the UK. The Lancet, 378(9793), 815–825. https://doi.org/10.1016/S0140-6736(11)60814-3
- Ward, A., & Mann, T. (2000). Don’t mind if I do: Disinhibited eating under cognitive load. Journal of Personality & Social Psychology, 78(4), 753–763. https://doi.org/10.1037//0022-3514.78.4.753
- Wardle, J., Steptoe, A., Oliver, G., & Lipsey, Z. (2000). Stress, dietary restraint and food intake. Journal of Psychosomatic Research, 48(2), 195–202.
- Wing, R. R., & Phelan, S. (2005). Long-term weight loss maintenance. The American Journal of Clinical Nutrition, 82(1 Suppl), 222S–225S. https://doi.org/10.1093/ajcn/82.1.222S