
Abstract
Objective:
Job strain has been implicated in a variety of adverse health outcomes, particularly cardiometabolic and inflammatory diseases. However, the mechanisms underlying these effects remain largely unknown. One possibility is that the maladaptive coping response to stress, (perseverative cognition (PC); the cognitive representation of past stressful events (rumination) or feared future events (worry)), either in work or more generally, mediates the relationship between job strain and physical disease. The aim of this study was thus to test the potential role of both general, and work- related PC as a mediating, or potentially moderating, mechanism between job strain and ill- health outcomes.
Design & Measures:
Using an online cross- sectional design, 650 full- time employees completed measures of job strain, general and work- related PC (rumination & worry) and health outcomes (burnout, somatization, health behaviours & sleep quality).
Results:
General and work- related worry and rumination significantly mediated, often independently, the relationship between job strain and burnout, somatization, and sleep quality. No significant mediation effects were observed for health behaviours and no type of PC (general or work- related) moderated job strain- health outcome relations.
Conclusion:
Both general and work- related worry and rumination are likely to play important, and partly independent, roles in understanding the adverse relationships between job strain and various health outcomes.
Introduction
The United Kingdom Health and Safety Executive estimates 12.8 million working days are lost each year as a consequence of work-related stress, costing the taxpayer an annual bill of £5.2 billion (HSE, Citation2022). Research on work-related stress was relatively sparse until the late 1970s (Beehr, Citation1998), but a plethora of studies now exist showing that work-related stress is not only a risk factor for absenteeism (e.g. Kinnunen & Nätti, Citation1994; Palmer, Citation2018), but also for a range of negative mental and physical health outcomes (e.g. Levenstein et al., Citation2001; O’Connor et al., 2021). For example, individuals experiencing heightened stress at work report lower self-rated health (De Witte et al., Citation2016; Ferrie et al., Citation2005), high levels of mental distress (e.g. O’Connor et al., Citation2000a, Citation2021a), increased instances of coronary heart disease and hypertension (Levenstein et al., Citation2001) and are also more likely to suffer from obesity (Ferrie et al., Citation2005; Muenster et al., Citation2011). For these reasons, many now consider work-related stress a modern-day pandemic and call for urgent preventative action (Mental Health Foundation, Citation2020).
One of the most significant and long-standing models of occupational stress is the job demands-control model (Karasek, Citation1979). Two fundamental mechanisms underpin the model: psychological strain and active learning mechanisms. The former is characterised by the experience of high job demands with simultaneous low levels of control over decision-making, leading to greater psychological strain. The latter is categorized based on the experience of high job demands and low levels of control and is said to promote the development of new adaptive behaviours. Importantly, the model is underpinned by several existing theories within the stress literature (cf., Cohen et al., Citation2016; Brosschot et al., Citation2016, Citation2017, Citation2018) informed by the concept of ‘allostatic load’ (McEwen, Citation1998); attesting that the wear and tear that the body experiences is due to repeated and long-term exposure to stress. It would therefore follow that actions to meet work demands yield short-term psychological (e.g. mental fatigue) and physiological (e.g. increased heart rate, adrenaline secretion) reactions which, initially, are adaptive and reversible. However, when one fails to recover, the adaptive nature of the response turns into negative load effects, such as exhaustion, chronic tension and persistent sleep difficulties (Geurts & Sonnentag, Citation2006; Kuiper et al., Citation1998; O’Connor et al., Citation2007).
Empirical data dating back to the mid-nineties supports the adverse relationship between job strain and ill-health. The Whitehall II study (North et al., Citation1996) was a relatively early example of a study that demonstrated that low job control, whether through self-report or independent assessment, predicted significantly more incidences of coronary heart disease and higher rates of short term and long-term sickness absence. In fact, adjusting for low decision control reduced the odds-ratio to develop any form of heart disease in the lowest grade (compared with the highest grade) from 1.5 to 1.2. Furthermore, a range of endocrinological and physiological evidence also now exists supporting this link. Landesbergis et al. (Citation2013), in a meta-analysis of 22 cross-sectional studies, showed that a single exposure to job strain was associated with higher ambulatory systolic blood pressure and diastolic blood pressure. Jarczok et al. (Citation2013) systematically reviewed the association between job strain and heart-rate variability (HRV). Thirty-six studies representing over 27,000 employees from 10 countries showed that job strain and adverse work conditions again were associated with decreased HRV. This is especially significant given a recent large-scale study reported that low levels of vagally mediated HRV are associated with elevated risk of a range of cardiometabolic and inflammatory diseases (Jarczok et al., Citation2020; Mauss et al., Citation2015).
However, recent advances in stress theory have highlighted a new mechanism through which stress at work may affect a range of psychobiological processes, even long after the stressor is present in the environment. The perseverative cognition hypothesis (PC Hypothesis; Brosschot et al., Citation2005, Citation2006, Citation2014) suggests that worry and/or rumination (via repetitive thinking) may lead to disease by prolonging the stress-related physiological activity associated with facing a stressor, by both amplifying the short-term bodily response to stress, and by delaying the recovery and/or reactivating the stress response following a stressor. Rumination and worry are similar constructs but differ in terms of content. Worry is linked to future-oriented threat prediction, often in an (unsuccessful) attempt to reduce negative outcomes or solve a problem (Borkovec, Citation1994). Rumination is characteristically related to perseveration about one’s own symptoms, the consequences of those symptoms, and past experiences habitually, in an (unsuccessful) exertion to understand oneself (Nolen-Hoeksema et al., Citation2008). Critically, these processes represent stressors that, when prolonged, activate harmful physiological and psychological outcomes (for review, see Ottaviani, Citation2018) and trigger unhealthy behaviours (for review, see Clancy et al., Citation2022). Given that job stress is not strictly bound to the work environment and is likely, if not inevitable to spill over into non-work domains (see, Lourel et al., Citation2009), the maladaptive response to stress – experienced through worry or rumination – may be particularly sensitive to work-related stressors.
Existing empirical studies accounting for the role of perseverative cognition (PC) at work primarily focus on rumination and one’s recovery or respite from work (e.g. Cropley & Zijlstra, Citation2011), along with its consequences for psychological and emotional wellbeing (e.g. Hamesch et al., Citation2014), burnout (Marinelli & Piazza, Citation2002), and work reappraisal (Ray et al., Citation2008). Of the studies drawing associations between perseverative cognition and health consequences, many are dated (e.g. Roger & Hudson, Citation1995; Roger & Najarian, Citation1998; Cropley & Millward Purvis, Citation2003) and few of them attempt to capture a broad range of health outcomes within the same sample of participants (e.g. sleep, Van Laethem et al., Citation2016; burnout, May et al., Citation2020). Existing studies have also tended to focus solely on physical health outcomes and despite the findings being crucial to understanding the role of perseverative cognition at work – such as those showing men who cannot relax after work have a threefold increased risk of heart disease (Cropley et al., Citation2017) – demonstrate the role of health behaviours should not be overlooked. Some evidence does exist for the relationships between work-related rumination and biomarkers of sleep; for example, whereby high ruminators have been linked to a heightened cortisol awakening response (see, Steptoe et al., Citation2000). However, less work focuses on overall sleep quality, which is concerning given non-work time largely consists of sleeping and recuperation (Åkerstedt & Nilsson, Citation2003).
The respective role(s) of work-related worry and rumination, and how these relate to their more general counterparts, within the context of job strain and health outcomes is unclear. Because of their unique potential to prolong the impact of work-related stressors (e.g. Cropley et al., Citation2006), work-related worry and rumination may represent specific, and particularly damaging, manifestations of employees’ inability to ‘switch-off’ following work. There is some evidence to suggest work-related rumination is linked to physiological markers of ill-health (such as lower parasympathetic activity, see Cropley et al., Citation2017); however, a scarcity of studies exist which assess the role of worry at (or about) work (exceptions are Aasa et al., Citation2005; Flaxman et al., Citation2012; Van Laethem et al., Citation2015). This is significant as, in line with the PC Hypothesis, if people are likely to start thinking and anticipating work before they arrive then its more than probable that these feelings will decompartmentalize in some form of worry. Therefore, work-related (as well as general) worry and rumination may augment the adverse health impacts of stress at work, potentially serving as a moderating mechanism; such that more job strain and worry interact to produce poorer health outcomes. It may also be the case that work-related worry and rumination, in congruence with the PC Hypothesis, mediate this relationship; such that the path from increased job strain to poor health may be fully explained by higher scores in worry and rumination.
Consequently, the present study aimed to consider the relative impact of both general and work-related worry and rumination as a mediating/moderating mechanism between the job strain and health outcome relationship. In doing so, we aimed to provide a renewed consideration of the psychosocial work environment as a predictive factor in public health outcomes. Furthermore, due to concerns that the defence/vigilance response associated to PC is in fact derived from neuroticism (cf., Watson & Pennebaker, Citation1989) and in light of recent findings suggesting negative affectivity may serve as an additional emotional risk factor to health during the ongoing coronavirus pandemic (see, Kroencke et al., Citation2020), sensitivity analyses were conducted to check whether the key findings hold after controlling for neuroticism. Importantly, this approach enables us to determine if the relationship between different types of PC and health outcomes, as well as the associations between job strain (through PC) on health, still stand when controlling for neuroticism. To test these aims, a sample of adults in full-time employment were recruited and completed a series of measures of job demands and control (from which a measure of job strain was derived), general and work-related PC, and a range of health-related outcomes (burnout, somatization, health behaviours and sleep). It was predicted that:
Higher levels of general PC (worry & rumination), as well as work-related PC, will be significantly associated with poorer health outcomes (Hypothesis 1);
General PC (Hypothesis 2 A), as well as work-related PC (Hypothesis 2B), will moderate the negative relationship between job strain and health outcomes, such that this relationship will be stronger in individuals with higher levels of general and work-related PC compared to lower levels;
General PC (Hypothesis 3 A), as well as work-related PC (Hypothesis 3B), will mediate the job strain and health outcome relationship. In relation to this final hypothesis, multiple mediation models will be conducted to test whether the different types of PC (general worry, general rumination, work-related worry, work-related rumination) additively contribute to the pathway between job demands and health outcomes such that they play a significantly unique and independent role, whether they play a similar role (and thus render one another non-significant), or whether some forms of PC are significant while others are not.
Method
Design & participants
The present study employed an online cross-sectional design to capture self-reported feelings towards stress at work and was preregistered on AsPredicted (see, here). Recruitment was purposefully sampled across adults who reported experiencing ‘stress at work’ between 1st January 2020 and 30th January 2021. Social media adverts (e.g. Facebook, Twitter) and Prolific were used as the primary recruitment methods; advertising was also shared externally by the Mental Health Foundation and MIND. Participants recruited through Prolific were paid in line with Prolific’s participants reimbursement policy (equivalent to £5 per hour). To be eligible, participants had to be employed on a full-time basis and be aged 18 years or older. The study received institutional ethical approval from a university-based ethics committee (REF: PSY-763).
An a-priori power calculation (in G*Power version 3.1; Faul et al., Citation2009) indicated a minimum of 616 participants would be required to detect an effect size of g = .28 (equivalent to r = .14) based on a power (1- β) of .80 in a one-tailed test with alpha set at .05. This was based on a recent meta-analysis which identified the average association between PC and health outcomes (McCarrick et al., Citation2021).
Eight hundred and three participants initially provided responses to the online questionnaire. Of these, 73 did not provide any information beyond consent, 45 only reported their demographical data, 35 progressed beyond the demographics section but did not complete all of the study variables specified in the hypotheses and 650 participants completed all measures. Consistent with our preregistration, the final sample comprised only of the 650 full-time employed adults (Mage = 28.9 years, SD = 10.9 years) completing all relevant measures. The data can be accessed via the Open Science Framework (OSF, here).
Nationality and ethnicity were classified in accordance with the categories outlined by the Office for National Statistics (ONS, Citation2021) and, due to the diverse range of occupations reported by participants, the International Certification of Jobs (ISCO-08) was used as a framework to organise job titles into a clearly defined set of groups based on the authority, responsibilities, tasks and duties associated to the respective job roles.
Measures
Predictor: job strain
The 35-item Health & Safety Executive Management Standards Indicator Tool (HSE; Cousins et al., Citation2004) is an extensively validated measure (e.g. Marcatto et al., Citation2014) used by organizations to monitor working conditions that can lead to increased stress. The scale comprises 6 sub-scales relating to stress in the workplace. Consistent with previously validated methodology (see, Landsbergis et al., Citation1994; O’Connor et al., Citation2000b) we computed a measure of job strain by dividing job demands (α = .87, e.g. “It is clear what is expected of me at work”) by job control (α = .82, e.g. “I know how to go about getting my job done”).
Mediators/moderators: perseverative cognition
General worry
The 16-item Penn-State Worry Questionnaire (PSWQ; Meyer et al., Citation1990) is often noted as the ‘gold standard’ measure of state worry. It has routinely demonstrated high internal consistency in non-clinical criterion groups (α = .95, Molina & Borkovec, Citation1994), has high test-retest reliability amongst adult populations (r = .74–.92) as well as substantial inter-rater reliability (r = .55; Stöber, Citation1998). Participants are instructed to indicate how typical statements are of them on a five-point scale varying from 1 (“not at all typical of me”) to 5 (“very typical of me”). Example items include “My worries often overwhelm me” and “I am always worrying about something”. A total score is calculated by summing the items and scores range from 16–80, with higher scores representing a greater degree of pathological worry.
Work-related worry
Given there is not currently a widely accepted and implemented measure for worry in the workplace, the 4-item Stress Arousal Scale (SAS; Smith et al., Citation2012) was used and adapted for brevity. Participants responded to questions relating to the cognitive-affective precursors of physiological stress on a 1 (“never”) to 5 (“always”) point-scale, with higher scores indicative of greater worry. The items were adapted to include a work focus such as “I am concerned or worried about things, at work” and “I anticipate upsetting things, about work”. The measure has been used before to assess work-related worry (e.g. Borghini et al., Citation2020), has demonstrated high internal consistency within a sample of full-time employed adults (α = .88; Smith et al., Citation2014), and shows good convergent validity with the PSWQ (r = .60).
General rumination
A shorter 10-item (Treynor et al., Citation2003) version of the Rumination Response Scale (RRS; Nolen-Hoeksema, Citation1991) was used to measure the frequency of depressive rumination through brooding and reflection. The scale correlates strongly with the full 21-item scale (r = .72 − .82) and yields an ‘overall’ score, as well as two subscales, Brooding and Reflection. Example items include: Brooding “Why do I always think this way?” and “What I am I doing to deserve this?”; Reflection: “I write things down and analyse them” and “I go someplace alone to think about my feelings”; with higher scores reflecting greater instances of rumination. Given Brooding is seen as more damaging than reflection in terms of health (cf., Schoofs et al., Citation2010), we repeated the analyses substituting the overall general rumination scores with the brooding scores. The results for the analyses in which the analyses are run with Brooding-specific items (rather than the ‘overall’ rumination measure) are reported in OSM 1, Section 4. In brief, this change did not significantly influence any of the findings relating to the present study’s hypotheses
Work-related rumination
The 15-item Work-Related Rumination Questionnaire (WRRQ) assesses the content domains of affective rumination, problem-solving pondering, and detachment from the three-factor model of perseverative thinking about work (Cropley et al., Citation2012). Given the detachment subscale has been shown to be strongly and negatively correlated with both the affective rumination and problem-solving pondering subscales, only the affective rumination and problem-solving pondering sub-scales were used in this study. Example items include “Are you troubled by work-related issues when not at work?” and “After work I tend to think about how I can improve my performance”. Items are responded to along a 5-point Likert scale ranging from 1 (“never”) to 5 (“always”), yielding a total score for each sub-factor which ranges from 0 to 25 (which was summed to make a composite score). The scale has been used and validated in previous studies in working adults, with good to excellent internal consistency (α = .81 − .90).
Outcomes
Burnout
The 18-item Copenhagen Burnout Inventory (CBI; Kristensen et al., Citation2005) consists of 3 subscales measuring personal, work-placed, and client-related burnout. Given the scope of the present study, the ‘work-placed’ subscale was used to capture participants’ current susceptibility to burnout in their workplace; which has been shown to predict future sickness absence, sleep problems and the use of pain-killers (Skakon et al., Citation2010). The measure employs a 1 (never) − 5 (always) scale, with higher scores indicating greater signs of burnout. Example items include “I feel worn out at the end of the working day” and “My work is emotionally exhausting”. The subscale demonstrates high levels of internal consistency (α = .87) and has promising convergent validity in both the mental (r = .67) and physical (r = .49) health subscales of the health-related quality of life inventory (SF-36 Health Survey; Ware, Citation1999).
Somatization
The Brief Symptom Inventory (BSI; Derogatis & Spencer, Citation1982) is a multidimensional test to measure current levels of psychological and physiological symptoms. The present study used the ‘Somatization’ subscale of the measure to capture participants’ experience of psychological distress in the form of somatic symptoms. Participants are asked to rate the degree to which they experience individual somatic symptoms on a scale of 1 (“not at all”) to 4 (“very much so”). Example items include ‘I get pains in heart or chest’, ‘I have trouble getting my breath’ and ‘I feel weak in parts of my body’. The somatization subscale has demonstrated acceptable test–retest reliability (r = .71) and good internal consistency (α = .85).
Sleep quality
The Pittsburgh Sleep Quality Index (PSQI; Buysse et al., Citation1989) is often regarded as the ‘gold-standard’ self-report measure of sleep quality (for review, see Mollayeva et al., Citation2016). The PSQI consists of 19 items that produce a global sleep quality score and the following 7 component scores: sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbance, use of sleeping medications, and daytime dysfunction. PSQI items use varying response categories that include recording usual bed time, usual wake time, number of actual hours slept, and number of minutes to fall asleep, as well as forced-choice Likert-type responses, resulting in an overall sleep quality score, with higher scores depicting poorer sleep. The scale has demonstrated good test–retest reliability (r = .79 − .83) and internal consistency (α = .83).
Health behaviours
The 16-item Good Health Practices scale (Hampson et al., Citation2019) provides a broad coverage of health promoting behaviours. To be consistent with the other study measures, and for ease of communication, all items were reverse scored such that higher scores reflected poorer health behaviours. A total score is provided by summing all items together. Participants responded to a 5-point Likert scale (1 = not at all like me − 5 = very much like me), with higher scores indicating unhealthier behaviours. Example items include “I exercise to stay healthy” and “I eat a balanced diet”. In the original study, the scale was internally consistent (α = .92) and predicted physiological dysregulation (e.g. abnormal blood glucose levels; higher body-mass-index).
Covariates
In addition to age and gender, neuroticism was also assessed as a covariate. The 10-item Neuroticism subscale of the Revised NEO Personality Inventory (NEO-PI-R; Costa & McCrae, Citation2008) was used to gauge participants’ self-perceptions of negativity and emotionally instability. The NEO PI-R is widely accepted as the ‘gold-standard’ questionnaire measure of the Five Factor Personality Model. Participants respond to a 5-point Likert scale ranging from 1 (“never”) to 5 (“always”), with higher scores being indicative of higher Neuroticism. Example items include “I dislike myself” and “I get easily irritated”. The Neuroticism sub-scale has excellent internal consistency in adults (α = .87 - .92; Asendorpf et al., Citation2001) as well as promising convergent validity with other measures of emotional instability (r = .68, Thompson et al., Citation2012).
Body Mass Index (BMI) and the number of hours each participant worked per week (HWPW were also self-reported, but as the strength of the relationships between these variables and the health outcome measures were typically very weak, non-significant, and directionally inconsistent (see , BMI: r = .04 − .12; HWPW: r = −.08 − .04), they were not considered within the regression analyses.
Table 1. Interrelationships between study variables (SD).
Procedure
After providing informed consent to participate in a study titled ‘Work, Health & Wellbeing Study’, participants completed the measures on a survey site (Qualtrics) in the following order: job strain, neuroticism, general worry and rumination, work-related worry and rumination, somatization, burnout, health behaviours, and sleep. The median time taken to complete the survey was 14 min and 21 s (SD = 5.56 minutes). Following completion of the survey, participants were debriefed.
Method of analysis
Data were analysed in R-Studio (version 3.6.2).
Data was first tested for randomness using Little’s Missing Completely At Random (MCAR) test as a small amount of data was missing for Body Mass Index (BMI, N = 39). Little’s test was non-significant (p = .745) and further graphical summaries confirmed there were no missing cases elsewhere in the data (see OSM 2, Section 2). As an extra safe-guard, the analyses were run with and without imputed data for this variable (i.e. BMI, using single, expectation maximization imputation). The use of imputed data did not alter the results; therefore, the non-imputed findings are reported.
Prior to conducting the main analyses, a comprehensive check of the associated statistical assumptions for normality, linearity, statistical independence and homoscedasticity/homogeneity of variance were conducted. In addition to visual checks (e.g. scatter plots, Cullen & Frey graphs, QQ-plots, PP-plots etc.), formal tests (e.g. Durbin-Watson, Goldfield-Quandt, Variance Inflation Factor etc.) were also computed to ensure the data were appropriate for regression/mediation analysis. In short, no major concerns were raised by these checks and the data were considered suitable for regression-based analysis.
The ‘lm’ function (Base R) was used to calculate beta coefficients to determine if greater PC was associated with poorer health outcomes and to conduct moderated regressions to assess interactions between job strain and PC on health outcomes. Multiple R2 was calculated to indicate the size of effects for the relationship(s) between study variables (Hypothesis 1 & 2). According to effect-size conventions for R2, .02, .15, and .35 represent small, medium, and large effects (Rosnow & Rosenthal, Citation1989). Across all analyses, bootstrapping, with 5,000 random imputations, was used to assess robustness; bootstrapped confidence intervals and re-sampled p-values were generated.
Correlational analyses were conducted to assess the interrelationships between the predictor (job strain), mediator (general and work-related worry and rumination) and outcomes (burnout, somatization, health behaviours and sleep quality).
A series of hierarchical ordinary-least squares (OLS) regressions were then conducted to test if higher levels of general PC, as well as work-related PC (i.e. worry and rumination), significantly predicted poorer health outcomes (i.e. burnout, somatization, health behaviours & sleep) (Hypothesis 1). Separate regressions were performed for each construct of PC to aid in comparisons with previous research and to maximise statistical power (see Hayes, Citation2009) (see, OSM 1, Section 1, Tables 1–16).
Further OLS regressions were used to test if general PC (worry or rumination) (Hypothesis 2 A), as well as work-related PC (worry or rumination) (Hypothesis 2B), significantly moderated the negative relationship between job strain and health outcomes, such that this relationship is intensified within individuals reporting higher levels of general and work-related PC. For these analyses, job strain was entered at step 1, general worry or rumination (or work-related worry or rumination) at step 2, and the interaction between job strain and general worry or rumination (or work-related worry or rumination) was entered at step 3.
Mediation, using the product of ordinary-least-squares estimation approach, was computed to determine if general PC (Hypothesis 3A), as well as work-related PC (Hypothesis 3B), significantly mediated the job strain and health outcome relationship. The R package ‘psych’ (Revelle, Citation2015) was used to estimate the direct, indirect, and the total effects for the path from the proposed predictor(s) (i.e. job strain) to the mediator(s) (i.e. general and work-related PC), and for the path from the mediator to the outcome variable (i.e. health outcomes). In view of highlighting the precise mechanism through which job strain is exacerbated through PC, and because it is unlikely the effect of an independent variable on an outcome variable is only transmittable by one means alone (Preacher & Hayes, Citation2008), both general worry and rumination and work-related worry and rumination were entered into the same multiple mediation model.
Finally, an additional set of regressions were conducted to test whether each type of PC (general worry & rumination (as a set); work-related worry and rumination (as a set); both general and work-related worry & rumination (combined together)) independently predicted poorer health outcomes. This approach was employed to determine if variation across the different types of PC independently predicted poorer health across the outcome variables. This may have implications from an applied perspective, as targeting worry and rumination together (rather than one alone) may produce more favourable changes in the outcomes.
Covariates
Given females were significantly more likely to suffer from burnout, t(572) = 2.60, p =.009, engage in poorer health behaviours, t(598) = 4.48, p <.001, and experience poorer sleep, t(572) = 3.44, p <.001; and because being younger was associated with significantly higher levels of burnout, β = −.04, p =.035, and somatization, β = −.09, p <.001, age and gender were considered as covariates. In addition to asess if the relationships between PC and the outcomes were independent from established personality correlates of stress (i.e. neuroticism, see Enns et al., Citation2005), the analyses were also ran with (and without) neuroticism included (at step 3). These results are reported within OSM 1.
Results
Participant characteristics
An overview of participants’ demographics can be found in . Typically, participants were white males aged around 29 years old, worked approximately 31.5 h a week, and were educated to university level (see ). Scores for both types of PC, as well as job strain, were particularly high in the present sample and the degree to which the scores were dispersed around the mean was relatively small. Further figures, for the different participant demographics and how they were related to the different measures of PC and health, are presented in OSM 2, Section 1 (see Figures 1–13).
Table 2. Participant demographics.
Hypothesis 1: Does greater PC predict poorer health outcomes?
The correlational analyses suggested that the all measures of PC were related with burnout (particularly the work-related measures of PC), somatization and sleep quality, with higher levels of PC associated with higher burnout, higher somatization and poorer sleep quality (see ). The PC measures were unrelated to the overall measure of health behaviours. The analyses also revealed that the measures of PC were modestly correlated with each other, with the exception of work-related worry and work-related rumination (i.e. all r’s between .34 and .62), suggesting that they are distinct constructs.
General perseverative cognition
In separate regressions for worry and rumination, general PC significantly predicted burnout (worry: β = .47, p <.001, R2 = .22; rumination: β = .46, p <.001, R2 = .21), somatization (worry: β = .41, p <.001, R2 = .17; rumination: β = .49, p <.001, R2 = .24), and sleep quality (β = .34, p <.001, R2 = .12; β = .31, p <.001, R2 = .09). These associations remained after controlling for age and gender together, as well as neuroticism alone (see OSM 1). Although higher levels of general worry were initially statistically unrelated to health behaviours (β = .04, p = .258, R2 = .01), it did become a significant predictor after controlling for age and gender (as a set), β = .09, p = .025, R2 = .01.
Higher levels of rumination were initially statistically unrelated to health behaviours, β = −.01, p = .849, R2 = .01), but when gender and neuroticism were controlled for (as a set) higher levels of general rumination was significantly associated to poorer health behaviours (β = −.15, p <.001, R2 = .02). Each of these associations, for both general worry and general rumination, also stood when controlling for neuroticism (see OSM 1).
Work-related perseverative cognition
Work-related PC significantly predicted burnout (worry: β = .64, p <.001, R2 = .41; rumination: β = .58, p <.001, R2 = .33), somatization (worry: β = .47, p <.001, R2 = .22; rumination: β = .39, p <.001, R2 = .15) and sleep quality (worry: β = .31, p <.001, R2 = .10; rumination: β = 18, p <.001, R2 = .03). Higher levels of work-related PC were statistically unrelated to health behaviours (worry: β = .02, p = .534, R2 = .01; rumination: β = −.04, p = .369, R2 = .01).
Although higher levels of work-related worry were initially statistically unrelated to health behaviours, β = .02, p = .534, R2 = .01, it did become a significant predictor after controlling for age and gender (as a set), β =.-.08, p <.001, R2 = .09. Further information on each of these analyses can be found in OSM 1.
Additional analyses
An extra set of sensitivity analyses testing if each type of PC (when entered together, at the same level, as predictor variables) predicted poorer health outcomes, revealed that, with the exception of the relationship between work-related rumination and sleep quality, β = −.01, p = .608, R2 = .01, each type of PC remained a significant predictor of greater burnout and somatization, as well as poorer sleep quality. As in the main analyses, no relationships were observed for health behaviours (see, OSM 1, Section 3, Tables 21–23). This suggests worry and rumination (both general and work-related) are uniquely important predictors of ill-health.
Hypothesis 2: Does Perseverative Cognition moderate the relationship between job strain and health outcomes?
While job strain significantly predicted greater burnout across each analyses containing the different types of PC, B = 12.87 to 37.47, SE = 5.73 − 9.12, all p <.01, R2 = .32 − .47, none of the PC measures (general or work-related) moderated the relationships between job strain and any of the outcome variables. The regression models for these results can be found in OSM 1, Tables 17–20.
Hypothesis 3: Does Perseverative Cognition mediate the relationship between job strain and health outcomes?
The mediation models revealed significant indirect paths between job strain and burnout, somatization, and sleep quality (but not health behaviours), via total PC (general worry; general rumination; work-related worry; work-related rumination) (see ). These paths remained significant when controlling for age, gender and neuroticism.
Table 3. Mediation analysis for job strain, PC, and health outcomes.
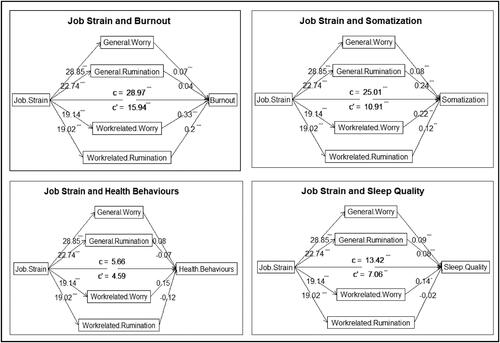
The individual paths from job strain to each outcome, via each type of PC, are shown in . With the exception of the paths from all types of PC to health behaviours, as well as the path from work-related rumination to sleep, and general rumination to burnout, all paths from job strain to PC and from PC to health outcomes (and the indirect paths) were significant.
Figure 1. Mediation path analysis for Job Strain, PC, and Health Outcomes. Note: The figure shows the individual paths from job strain to each outcome, via each type of PC. With the exception of the paths from all types of PC to health behaviours, as well as the path from work-related rumination to sleep, and general rumination to burnout, all paths from job strain to PC and from PC to health outcomes (and the indirect paths) were significant. Numbers reflect the unstandardized regression coefficients; C = the total effect of x on y; C’ = the direct effect of x on y; ***p < .001; **p < .01; *p < .05.
Discussion
The aim of the present study was to test the relative impact of both general and work-related worry and rumination as a mediating and/or moderating mechanism between job strain and health outcomes. The data were broadly in support of our hypotheses regarding the predictive role of PC on health and its function as a mediator between stress and ill-health, although PC and job strain did not interact to predict health outcomes. Both types of general and work-related worry and rumination predicted significantly higher scores in burnout and somatization, as well as lower scores in sleep quality (Hypothesis 1). Until age and gender were controlled for, no significant relationships were observed for the impact of any type of PC on health behaviours. While job strain significantly predicted greater burnout across each analysis containing the different types of PC, none of the PC measures (general or work-related) interacted with job strain to predict any of the health outcome variables (Hypothesis 2). However, for the mediation analyses, with the exception of the paths from all types of PC to health behaviours, as well as the path from work-related rumination to sleep, and general rumination to burnout, all paths from job strain to PC and from PC to health outcomes (and the indirect paths) were statistically significant (Hypothesis 3). Thus, together, the results of the present study provide fresh evidence for the damaging nature of PC, its role as an important mediating mechanism between exposure to stress and adverse health outcomes as well as the potential unique, additive contributions of different types of PC.
Similar to previous studies linking PC to health consequences (for reviews, see Ottaviani, Citation2018; Clancy et al., Citation2020a), and in conjunction with Hypothesis 1, higher scores in PC predicted more adverse health outcomes. In the present study, this finding is extended to a large, multi-cultural, sample of full-time employees. Specifically, all types of PC (both general and work-related) predicted significantly higher scores in burnout and somatization, as well as lower scores in sleep quality. This is significant as, despite emerging reports linking rumination specifically about work to physiological consequences (see Cropley et al., Citation2017) and some contemporary evidence for the effect of worry in the workplace (see Aasa et al., Citation2005 & Flaxman et al., Citation2012), we show, for the first time, that work-related worry and rumination – as well as its more general counterparts – represent a uniquely harmful threat to a range of health markers. It is also consistent with the original perseverative cognition hypothesis (see Brosschot et al., Citation2005), wherein the repetitive and pervasive thinking styles represented by worry and/or rumination (or in this case about work) may amplify the short-term bodily response to stress and delay the recovery and/or reactivation of the stress response following exposure to a stressor. Thus, it would follow that, employees’ psychological manifestations of past and future stressors experienced either through worry or rumination about work (e.g. upcoming deadlines; fractious relationships with colleagues), or just more generally (e.g. personal feelings of inadequacy; analyzing past behaviours), likely contribute to their inability to ‘switch-off’ following work (through rumination) and to mentally loiter over stressors (via worry). It is also important to note that all of the observed effects held after controlling for neuroticism indicating that PC is a distinct and independent predictor of these outcomes.
While job strain, that is high job demand and low job control, did predict significant increases in burnout, our consideration of the interplay between PC and health within the context of job strain, was not in line with our hypotheses (see Hypothesis 2 A & 2B). Indeed, no moderation effects were observed between any type of PC (general or work-related) and job strain on any health outcome. Some consistency can be sought, however, between this null result and of those reported by previous studies. Cropley et al. (Citation2006), for example, found that work-rumination did not significantly moderate the relationship between job strain and sleep quality; though, this was observed in a much smaller (N = 152) and homogeneous sample (i.e. school teachers). Equally, also for sleep, Van Laethem et al. (Citation2015) reported similar size associations between PC and sleep quality in a longitudinal study (r = .28 − .32). It is also notable that the absolute strength of the reciprocal relationships between PC and sleep in that study were much smaller than those in the present study (e.g. direct effect, B = .03 vs B = 7.06); although, crucially, moderation effects were not formally assessed.
While there is plentiful evidence showing that high job strain is related to ill-health (for review, see Amiri & Behnezhad, Citation2020) and some showing that coping resources do moderate the link between work stress and sleep (Åkerstedt et al., Citation2002; Sadeh et al., Citation2004), there are few studies that document the moderating effects of (the different types) of PC and job stain on the other health outcomes explored in this study (i.e. burnout; somatization; health behaviours) and what we could find was not in agreement and assessed largely homogeneous samples (i.e. school teachers). For example, Pieper et al. (Citation2007) found that teachers reporting high job strain displayed elevated cardiac activity that was no different to teachers reporting low job strain, nor did they report daily worry episodes more frequently. Whereas earlier reports by Cropley et al. (Citation1999) demonstrated that schoolteachers with high job strain were around twice as likely to experience worry and nearly two and half times more likely to report somatic symptoms. Further, in a recent review of 12 studies concluding that job strain is associated with lower psychological detachment from work, the authors pointed out the requirement for future work to consider other modes of perseverative thinking and its impact on a diversification of health outcomes (Türktorun et al., Citation2020).
The present study did, however, find significant mediation effects for the associations between PC and poorer health outcomes. Our findings (in particular the mediation models) support the theoretical link between job strain, different types of PC, and burnout, somatization and sleep quality. Indeed, with the exception of the paths from all types of PC to health behaviours, as well as the path from work-related rumination to sleep, and general rumination to burnout, all paths from job strain to PC and from PC to health outcomes (and the indirect paths) were statistically significant. Not only does this finding broadly support Hypothesis 3 but it is consistent with a range of empirical evidence (for reviews, see; Clancy et al., Citation2016; Clancy et al., Citation2020b; Ottaviani, Citation2018; Verkuil et al., Citation2010) and theoretical considerations advocating the causal chain through which PC influences health (see Brosschot et al., Citation2005 for the original PC Hypothesis; O’Connor et al., Citation2021b). While it might appear axiomatic that people with high job strain, and who engage in worry and/or rumination are more prone to burnout, somatization and poorer sleep, to the best of our knowledge, this is the first time this relationship has been examined collectively.
The main findings of the current study also have implications for interventions looking to reduce the negative effects of PC on health and wellbeing. In particular, our multi-mediator models and sensitivity analyses (see OSM 1, Section 3) suggest that targeting both worry and rumination may produce more positive outcomes than targeting either alone. Further research should be conducted to identify the types of techniques that best influence worry and rumination. As noted by McCarrick et al’s. (Citation2021) review of the experimental literature, relatively few intervention techniques have been used to try reduce PC with only 7 broad types of intervention identified and worry and/or rumination were rarely considered as a primary outcome in studies. Moreover, it is not known, how well specific techniques work for work-related worry and rumination explicitly. Nevertheless, the results of the present study highlight the need for future work-based studies considering health to examine maladaptive cognitive processes, such as PC; especially considering work-related PC has now also been shown to play a damaging role in both general and work-related and general distress (see Prudenzi et al., Citation2021).
This study is not without its limitations. First, this study relies exclusively on self-report measures to assess both its predictor and outcome variables. Several problems have been associated with the use of self-report measures such as social desirability or retrospection (Furnham, Citation1986). Future studies should therefore seek to not solely rely on self-report tools, but to use objective methods to assess, for instance, at least the outcome measures for health. For example, one could use actigraphy (see Van Laethem et al., Citation2013) to assess sleep quality or use daily-diary style methods to capture individual types of health behaviours (e.g. Clancy et al., Citation2020a). In addition, we also recognise the limitations of using a cross-sectional design in terms temporal validity and issues relating to causality (e.g. Maxwell et al., Citation2011). Therefore, future research ought to attempt to replicate the current findings using large scale longitudinal designs. Quasi-experimental field studies may also represent a fruitful avenue of future research to help understand the bidirectional relationships between stress, PC, work-related PC, and health outcomes. In addition, the work-based and general PC measures were not entirely matched with differences across items not just related to context (workplace vs. general). As such, differences in work-based and general PC findings cannot be entirely attributable to differences in context. Finally, while the composite measure used to tap health behaviours is useful for broadly understanding the relationships between PC and health behaviours overall, stronger relationships may arise with specific health behaviours (e.g. sleep, Radstaak et al., Citation2014; unhealthy snacking, Eschle & McCarrick, Citation2021) that are not detectable in the composite measure we used. Future studies should therefore look to explore the interrelationships between PC and individual health behaviours, ideally via prospective study designs (e.g. McCarrick et al., Citation2022).
To conclude, the present study provides supportive evidence for the PC Hypothesis and the role worry and rumination play as related, yet distinct, cognitive processes in contributing to ill-health. Both types of general and work-related worry and rumination predicted significantly higher scores in burnout and somatization, as well as lower scores in sleep quality, but further work is needed to understand the role of health behaviours. Job strain significantly predicted greater burnout across each analysis containing the different types of PC, but none of the PC measures (general or work-related) interacted with job strain to predict any of the health outcome variables. However, for the mediation analyses, with the exception of the paths from all types of PC to health behaviours, as well as the path from work-related rumination to sleep, and general rumination to burnout, all paths from job strain to PC and from PC to health outcomes (and the indirect paths) were statistically significant implying the additive roles of different types of PC. Therefore, taken together, the results of the present study provide new evidence for the damaging nature of PC and its role as an important mediating factor between stress and health-related outcomes.
Supplemental Material
Download Zip (531.3 KB)Acknowledgement
This research was undertaken in partial fulfilment of the lead author’s PhD.
Funding
This research was funded by the Economic & Social Research Council.
References
- Aasa, U., Brulin, C., Ängquist, K. A., & Barnekow-Bergkvist, M. (2005). Work-related psychosocial factors, worry about work conditions and health complaints among female and male ambulance personnel. Scandinavian Journal of Caring Sciences, 19(3), 251–258. https://doi.org/10.1111/j.1471-6712.2005.00333.x
- Åkerstedt, T., Fredlund, P., Gillberg, M., & Jansson, B. (2002). Work load and work hours in relation to disturbed sleep and fatigue in a large representative sample. Journal of Psychosomatic Research, 53(1), 585–588. https://doi.org/10.1016/S0022-3999(02)00447-6
- Åkerstedt, T., & Nilsson, P. M. (2003). Sleep as restitution: An introduction. Journal of Internal Medicine, 254(1), 6–12. https://doi.org/10.1046/j.1365-2796.2003.01195.x
- Amiri, S., & Behnezhad, S. (2020). Smoking and risk of sleep-related issues: A systematic review and meta-analysis of prospective studies. Canadian Journal of Public Health/Revue Canadienne de Sante Publique, 111(5), 775–786. https://doi.org/10.17269/s41997-020-00308-3
- Asendorpf, J. B., Borkenau, P., Ostendorf, F., & van Aken, M. A. G. (2001). Carving personality description at its joints: Confirmation of three replicable personality prototypes for both children and adults. European Journal of Personality, 15(3), 169–198. [Database] https://doi.org/10.1002/per.408
- Beehr, T. (1998). An organizational psychology meta-model of occupational stress. Theories of organizational stress (pp. 6–27). Oxford University Press.
- Borghini, G., Di Flumeri, G., Aricò, P., Sciaraffa, N., Bonelli, S., Ragosta, M., … Babiloni, F. (2020). A multimodal and signals fusion approach for assessing the impact of stressful events on. Air Traffic Controllers. Scientific Reports, 10(1), 1–18.
- Borkovec, T. D. (1994). The nature, functions, and origins of worry. Worrying: Perspectives on theory, assessment and treatment. John Wiley & Sons.
- Brosschot, J. F., Gerin, W., & Thayer, J. F. (2006). The perseverative cognition hypothesis: A review of worry, prolonged stress-related physiological activation, and health. Journal of Psychosomatic Research, 60(2), 113–124. https://doi.org/10.1016/j.jpsychores.2005.06.074
- Brosschot, J. F., Geurts, S. A. E., Kruizinga, I., Radstaak, M., Verkuil, B., Quirin, M., & Kompier, M. A. J. (2014). Does unconscious stress play a role in prolonged cardiovascular stress recovery? Stress and Health: Journal of the International Society for the Investigation of Stress, 30(3), 179–187. https://doi.org/10.1002/smi.2590
- Brosschot, J. F., Pieper, S., & Thayer, J. F. (2005). Expanding stress theory: Prolonged activation and perseverative cognition. Psychoneuroendocrinology, 30(10), 1043–1049. https://doi.org/10.1016/j.psyneuen.2005.04.008
- Brosschot, J. F., Verkuil, B., & Thayer, J. F. (2016). The default response to uncertainty and the importance of perceived safety in anxiety and stress: An evolution-theoretical perspective. Journal of Anxiety Disorders, 41, 22–34. https://doi.org/10.1016/j.janxdis.2016.04.012
- Brosschot, J. F., Verkuil, B., & Thayer, J. F. (2017). Exposed to events that never happen: Generalized unsafety, the default stress response, and prolonged autonomic activity. Neuroscience and Biobehavioral Reviews, 74(Pt B), 287–296. https://doi.org/10.1016/j.neubiorev.2016.07.019
- Brosschot, J. F., Verkuil, B., & Thayer, J. F. (2018). Generalized unsafety theory of stress: Unsafe environments and conditions, and the default stress response. International Journal of Environmental Research and Public Health, 15(3), 464. https://doi.org/10.3390/ijerph15030464
- Buysse, D. J., Reynolds, C. F., III, Monk, T. H., Berman, S. R., & Kupfer, D. J. (1989). The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Research, 28(2), 193–213.
- Clancy, F., O’Connor, D. B., & Prestwich, A. (2020a). Do worry and brooding predict health behaviors? A daily diary investigation. International Journal of Behavioral Medicine, 27(5), 591–601. https://doi.org/10.1007/s12529-020-09898-1
- Clancy, F., Prestwich, A., Caperon, L., & O’Connor, D. B. (2016). Perseverative cognition and health behaviours. A systematic review and meta-analysis. Frontiers in Human Neuroscience, 10, 534.https://doi.org/10.3389/fnhum.2016.00534
- Clancy, F., Prestwich, A., Caperon, L., Tsipa, A., & O’Connor, D. B. (2020b). The association between worry and rumination with sleep in non-clinical populations. A systematic review and meta-analysis. Health Psychology Review, 14(4), 427–448. https://doi.org/10.1080/17437199.2019.1700819
- Clancy, F., Prestwich, A., Ferguson, E., & O’Connor, D. B. (2022). Cross-sectional and prospective associations between stress, perseverative cognition and health behaviours. Psychology & Health, 37(1), 87–104.
- Cohen, S., Gianaros, P. J., & Manuck, S. B. (2016). A stage model of stress and disease. Perspectives on Psychological Science: A Journal of the Association for Psychological Science, 11(4), 456–463. https://doi.org/10.1177/1745691616646305
- Costa, P. T., Jr., & McCrae, R. R. (2008). The Revised NEO Personality Inventory (NEO-PI-R). Sage Publications, Inc.
- Cousins, R., Mackay, C. J., Clarke, S. D., Kelly, C., Kelly, P. J., & McCaig, R. H. (2004). ‘Management standards’ work-related stress in the UK: Practical development. Work & Stress, 18(2), 113–136. https://doi.org/10.1080/02678370410001734322
- Cropley, M., Steptoe, A., & Joekes, K. (1999). Job strain and psychiatric morbidity. Psychological Medicine, 29(6), 1411–1416.
- Cropley, M., Dijk, D. J., & Stanley, N. (2006). Job strain, work rumination, and sleep in school teachers. European Journal of Work and Organizational Psychology, 15(2), 181–196. https://doi.org/10.1080/13594320500513913
- Cropley, M., Michalianou, G., Pravettoni, G., & Millward, L. J. (2012). The relation of post-work ruminative thinking with eating behaviour. Stress and Health: Journal of the International Society for the Investigation of Stress, 28(1), 23–30. https://doi.org/10.1002/smi.1397
- Cropley, M., & Millward Purvis, L. (2003). Job strain and rumination about work issues during leisure time: A diary study. European Journal of Work and Organizational Psychology, 12(3), 195–207. https://doi.org/10.1080/13594320344000093
- Cropley, M., Plans, D., Morelli, D., Sütterlin, S., Inceoglu, I., Thomas, G., & Chu, C. (2017). The association between work-related rumination and heart rate variability: A field study. Frontiers in Human Neuroscience, 11, 27.
- Cropley, M., & Zijlstra, F. R. (2011). Work and rumination. Handbook of Stress in the Occupations, 487, 503.
- De Witte, H., Pienaar, J., & De Cuyper, N. (2016). Review of 30 years of longitudinal studies on the association between job insecurity and health and well-being: Is there causal evidence? Australian Psychologist, 51(1), 18–31. https://doi.org/10.1111/ap.12176
- Derogatis, L. R., & Spencer, D. S. (1982). The Brief Symptom Inventory (BSI): Administration, scoring, and procedures manual - 1. Johns Hopkins University School of Medicine, Clinical Psychometrics Research Unit.
- Enns, M. W., Cox, B. J., & Clara, I. P. (2005). Perfectionism and neuroticism: A longitudinal study of specific vulnerability and diathesis-stress models. Cognitive Therapy and Research, 29(4), 463–478. https://doi.org/10.1007/s10608-005-2843-04
- Eschle, T. M., & McCarrick, D. (2021). Perseverative cognition and snack choice: An online pilot investigation. Behavioral Sciences, 11(3), 33. https://doi.org/10.3390/bs11030033
- Faul, F., Erdfelder, E., Buchner, A., & Lang, A. G. (2009). Statistical power analyses using G* Power 3.1: Tests for correlation and regression analyses. Behavior Research Methods, 41(4), 1149–1160. https://doi.org/10.3758/BRM.41.4.1149
- Ferrie, J. E., Shipley, M. J., Newman, K., Stansfeld, S. A., & Marmot, M. (2005). Self-reported job insecurity and health in the Whitehall II study: Potential explanations of the relationship. Social Science & Medicine, 60(7), 1593–1602. https://doi.org/10.1016/j.socscimed.2004.08.006
- Flaxman, P. E., Ménard, J., Bond, F. W., & Kinman, G. (2012). Academics’ experiences of a respite from work: Effects of self-critical perfectionism and perseverative cognition on postrespite well-being. The Journal of Applied Psychology, 97(4), 854–865. https://doi.org/10.1037/a0028055
- Furnham, A. (1986). Response bias, social desirability and dissimulation. Personality and Individual Differences, 7(3), 385–400. https://doi.org/10.1016/0191-8869(86)90014-0
- Geurts, S. A., & Sonnentag, S. (2006). Recovery as an explanatory mechanism in the relation between acute stress reactions and chronic health impairment. Scandinavian Journal of Work, Environment & Health, 32(6), 482–492. https://doi.org/10.5271/sjweh.1053
- Hamesch, U., Cropley, M., & Lang, J. (2014). Emotional versus cognitive rumination: Are they differentially affecting long-term psychological health? The impact of stressors and personality in dental students. Stress and Health: Journal of the International Society for the Investigation of Stress, 30(3), 222–231. https://doi.org/10.1002/smi.2602
- Hampson, S. E., Edmonds, G. W., & Goldberg, L. R. (2019). The Health Behavior Checklist: Factor structure in community samples and validity of a revised good health practices scale. Journal of Health Psychology, 24(8), 1103–1109. https://doi.org/10.1177/1359105316687629
- Hayes, A. F. (2009). Beyond Baron and Kenny: Statistical mediation analysis in the new millennium. Communication Monographs, 76(4), 408–420. https://doi.org/10.1080/03637750903310360
- Health & Saftey Executive (2022). The Health and Safety Executive annual report and accounts 2021 to 2022. https://www.gov.uk/government/publications/the-health-and-safety-executive-annual-report-andaccounts-2021-to-2022.
- Jarczok, M. N., Jarczok, M., Mauss, D., Koenig, J., Li, J., Herr, R. M., & Thayer, J. F. (2013). Autonomic nervous system activity and workplace stressors—A systematic review. Neuroscience and Biobehavioral Reviews, 37(8), 1810–1823. https://doi.org/10.1016/j.neubiorev.2013.07.004
- Jarczok, M. N., Jarczok, M., & Thayer, J. F. (2020). Work stress and autonomic nervous system activity. Handbook of socioeconomic determinants of occupational health: From macro-level to micro-level evidence (pp. 1–33). Springer.
- Karasek, R. A.Jr, (1979). Job demands, job decision latitude, and mental strain: Implications for job redesign. Administrative Science Quarterly, 24(2), 285–308. https://doi.org/10.2307/2392498
- Kinnunen, U., & Nätti, J. (1994). Job insecurity in Finland: Antecedents and consequences. European Work and Organizational Psychologist, 4(3), 297–321. https://doi.org/10.1080/13594329408410490
- Kristensen, T. S., Borritz, M., Villadsen, E., & Christensen, K. B. (2005). The Copenhagen Burnout Inventory: A new tool for the assessment of burnout. Work & Stress, 19(3), 192–207. https://doi.org/10.1080/02678370500297720
- Kroencke, L., Geukes, K., Utesch, T., Kuper, N., & Back, M. D. (2020). Neuroticism and emotional risk during the COVID-19 pandemic. Journal of Research in Personality, 89, 104038. https://doi.org/10.1016/j.jrp.2020.104038
- Kuiper, J. I., Van der Beek, A. J., & Meijman, T. F. (1998). Psychosomatic complaints and unwinding of sympathoadrenal activation after work. Stress Medicine, 14(1), 7–12. https://doi.org/10.1002/(SICI)1099-1700(199801)14:1<7::AID-SMI751>3.0.CO;2-Y
- Landsbergis, P. A., Dobson, M., Koutsouras, G., & Schnall, P. (2013). Job strain and ambulatory blood pressure: a meta-analysis and systematic review. American Journal of Public Health, 103(3), e61–e71.
- Landsbergis, P. A., Schnall, P. L., Warren, K., Pickering, T. G., & Schwartz, J. E. (1994). Association between ambulatory blood pressure and alternative formulations of job strain. Scandinavian Journal of Work, Environment & Health, 20(5), 349–363. https://doi.org/10.5271/sjweh.1386
- Levenstein, S., Smith, M. W., & Kaplan, G. A. (2001). Psychosocial predictors of hypertension in men and women. Archives of Internal Medicine, 161(10), 1341–1346. https://doi.org/10.1001/archinte.161.10.1341
- Lourel, M., Ford, M. T., Gamassou, C. E., Guéguen, N., & Hartmann, A. (2009). Negative and positive spillover between work and home: Relationship to perceived stress and job satisfaction. Journal of Managerial Psychology, 24(5), 438–449. https://doi.org/10.1108/02683940910959762
- Marcatto, F., Colautti, L., Larese Filon, F., Luis, O., & Ferrante, D. (2014). The HSE management standards indicator tool: Concurrent and construct validity. Occupational Medicine (Oxford, England), 64(5), 365–371. https://doi.org/10.1093/occmed/kqu038
- Marinelli, M., & Piazza, P. V. (2002). Interaction between glucocorticoid hormones, stress and psychostimulant drugs. The European Journal of Neuroscience, 16(3), 387–394. https://doi.org/10.1046/j.1460-9568.2002.02089.x
- Mauss, D., Li, J., Schmidt, B., Angerer, P., & Jarczok, M. N. (2015). Measuring allostatic load in the workforce—A systematic review. Industrial Health, 53(1), 5–20. https://doi.org/10.2486/indhealth.2014-0122
- May, R. W., Bauer, K. N., Seibert, G. S., Jaurequi, M. E., & Fincham, F. D. (2020). School burnout is related to sleep quality and perseverative cognition regulation at bedtime in young adults. Learning and Individual Differences, 78, 101821. https://doi.org/10.1016/j.lindif.2020.101821
- Maxwell, S. E., Cole, D. A., & Mitchell, M. A. (2011). Bias in cross-sectional analyses of longitudinal mediation: Partial and complete mediation under an autoregressive model. Multivariate Behavioral Research, 46(5), 816–841.
- McCarrick, D., Prestwich, A., & O’Connor, D. B. (2022). Perseverative cognition and health behaviours: Exploring the role of intentions and perceived behavioural control. Psychology & Health. https://doi.org/10.1080/08870446.2022.2130921
- McCarrick, D. J., Prestwich, A., Prudenzi, A., & O’Connor, D. B. (2021). Health effects of psychological interventions for worry and rumination: A meta-analysis. Health Psychology, 40(9), 617–630. https://doi.org/10.1037/hea0000985
- McEwen, B. S. (1998). Protective and damaging effects of stress mediators. The New England Journal of Medicine, 338(3), 171–179. https://doi.org/10.1056/NEJM199801153380307
- Mental Health Foundation. (2020). https://mhfaengland.org/mhfa-centre/research-and-evaluation/mental-health-statistics/
- Meyer, T. J., Miller, M. L., Metzger, R. L., & Borkovec, T. D. (1990). Development and validation of the penn state worry questionnaire. Behaviour Research and Therapy, 28(6), 487–495. https://doi.org/10.1016/0005-7967(90)90135-6
- Molina, S., & Borkovec, T. D. (1994). The Penn State Worry Questionnaire: Psychometric properties and associated characteristics. Behaviour Research and Therapy, 30(1), 33–37.
- Mollayeva, T., Thurairajah, P., Burton, K., Mollayeva, S., Shapiro, C. M., & Colantonio, A. (2016). The Pittsburgh sleep quality index as a screening tool for sleep dysfunction in clinical and non-clinical samples: A systematic review and meta-analysis. Sleep Medicine Reviews, 25, 52–73. https://doi.org/10.1016/j.smrv.2015.01.009
- Muenster, E., Rueger, H., Ochsmann, E., Letzel, S., & Toschke, A. M. (2011). Association between overweight, obesity and self-perceived job insecurity in German employees. BMC Public Health, 11(1), 1–7. https://doi.org/10.1186/1471-2458-11-162
- Nolen-Hoeksema, S. (1991). Responses to depression and their effects on the duration of depressive episodes. Journal of Abnormal Psychology, 100(4), 569–582. https://doi.org/10.1037//0021-843x.100.4.569
- Nolen-Hoeksema, S., Wisco, B. E., & Lyubomirsky, S. (2008). Rethinking rumination. Perspectives on Psychological Science: A Journal of the Association for Psychological Science, 3(5), 400–424. https://doi.org/10.1111/j.1745-6924.2008.00088.x
- North, F. M., Syme, S. L., Feeney, A., Shipley, M., & Marmot, M. (1996). Psychosocial work environment and sickness absence among British civil servants: The Whitehall II study. American Journal of Public Health, 86(3), 332–340. https://doi.org/10.2105/ajph.86.3.332
- O’Connor, D. B., Hall, L. H., & Johnson, J. (2021a). Job strain, burnout, wellbeing and patient safety. In A. Montgomery, M. Van der doef, E. Panagopoulou, & M. Leiter (Eds.), The triple challenge: Connecting health care worker well-being, patient safety and organisational change (pp. 11–23). Springer.
- O’Connor, D. B., O’Connor, R. C., White, B. L., & Bundred, P. E. (2000a). Job strain and ambulatory blood pressure in British general practitioners: A preliminary study. Psychology, Health & Medicine, 5(3), 241–250.
- O’Connor, D. B., O’Connor, R. C., & Marshall, R. (2007). Perfectionism and psychological distress: Evidence of the mediating effects of rumination. European Journal of Personality, 21(4), 429–452. https://doi.org/10.1002/per.616
- O’Connor, D. B., Thayer, J. F., & Vedhara, K. (2021b). Stress and health: A review of psychobiological processes. Annual Review of Psychology, 72, 663–688. https://doi.org/10.1146/annurev-psych-062520-122331
- O’Connor, D., O’Connor, R., White, B., & Bundred, P. (2000b). The effect of job strain on British general practitioners’ mental health. Journal of Mental Health, 9(6), 637–654. https://doi.org/10.1080/713680290
- Office for National Statisitics (2021). Ethnic group, national identity and religion. https://www.ons.gov.uk/methodology/classificationsandstandards/measuringequality/ethnicgroupnationalidentityandreligion
- Ottaviani, C. (2018). Brain-heart interaction in perseverative cognition. Psychophysiology, 55(7), e13082. https://doi.org/10.1111/psyp.13082
- Palmer, E. (2018). The heavy cost of care: Systemic challenges in Norwegian work absenteeism. Social Sciences, 7(6), 94. https://doi.org/10.3390/socsci7060094
- Pieper, S., Brosschot, J. F., van der Leeden, R., & Thayer, J. F. (2007). Cardiac effects of momentary assessed worry episodes and stressful events. Psychosomatic Medicine, 69(9), 901–909. https://doi.org/10.1097/PSY.0b013e31815a9230
- Preacher, K. J., & Hayes, A. F. (2008). Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods, 40(3), 879–891. https://doi.org/10.3758/brm.40.3.879
- Prudenzi, A., Graham, C. D., Clancy, F., Hill, D., O’Driscoll, R., Day, F., & O’Connor, D. B. (2021). Group-based acceptance and commitment therapy interventions for improving general distress and work-related distress in healthcare professionals: A systematic review and meta-analysis. Journal of Affective Disorders, 295, 192–202. https://doi.org/10.1016/j.jad.2021.07.084
- Radstaak, M., Geurts, S. A., Beckers, D. G., Brosschot, J. F., & Kompier, M. A. (2014). Work stressors, perseverative cognition and objective sleep quality: A longitudinal study among Dutch Helicopter Emergency Medical Service (HEMS) pilots. Journal of Occupational Health, 56(6), 469–477.
- Ray, R. D., Wilhelm, F. H., & Gross, J. J. (2008). All in the mind’s eye? Anger rumination and reappraisal. Journal of Personality and Social Psychology. 94(1), 133.
- Revelle, W. (2015). Package ‘psych’. The Comprehensive R Archive Network, 337, 338.
- Roger, D., & Hudson, C. (1995). The role of emotion control and emotional rumination in stress management training. International Journal of Stress Management, 2(3), 119–132. https://doi.org/10.1007/BF01740298
- Roger, D., & Najarian, B. (1998). The relationship between emotional rumination and cortisol secretion under stress. Personality and Individual Differences, 24(4), 531–538. https://doi.org/10.1016/S0191-8869(97)00204-3
- Rosnow, R. L., & Rosenthal, R. (1989). Definition and interpretation of interaction effects. Psychological Bulletin, 23(5), 143–146.
- Sadeh, A., Keinan, G., & Daon, K. (2004). Effects of stress on sleep: the moderating role of coping style. Health Psychology, 23(5), 542. https://doi.org/10.1007/s10862-010-9182-9
- Schoofs, H., Hermans, D., & Raes, F. (2010). Brooding and reflection as subtypes of rumination: Evidence from confirmatory factor analysis in nonclinical samples using the Dutch Ruminative Response Scale. Journal of Psychopathology and Behavioral Assessment, 32(4), 609–617. https://doi.org/10.1007/s10862-010-9182-9
- Skakon, J., Nielsen, K., Borg, V., & Guzman, J. (2010). Are leaders’ well-being, behaviours and style associated with the affective well-being of their employees? A systematic review of three decades of research. Work & Stress, 24(2), 107–139. https://doi.org/10.1080/02678373.2010.495262
- Smith, K. J., Everly, G. S., & Haight, G. T. (2012). SAS4: Validation of a four-item measure of worry and rumination. Advances in accounting behavioural research. Emerald Group Publishing Limited.
- Smith, K. J., Rosenberg, D. L., & Timothy Haight, G. (2014). An assessment of the psychometric properties of the perceived stress scale-10 (PSS 10) with business and accounting students. Accounting Perspectives, 13(1), 29–59. https://doi.org/10.1111/1911-3838.12023
- Steptoe, A., Cropley, M., & Joekes, K. (2000). Task demands and the pressures of everyday life: Associations between cardiovascular reactivity and work blood pressure and heart rate. Health Psychology: Official Journal of the Division of Health Psychology, American Psychological Association, 19(1), 46–54. https://doi.org/10.1037//0278-6133.19.1.46
- Stöber, J. (1998). Worry, problem elaboration and suppression of imagery: The role of concreteness. Behaviour Research and Therapy, 36(7-8), 751–756. https://doi.org/10.1016/S0005-7967(98)00027-8
- Thompson, R. J., Mata, J., Jaeggi, S. M., Buschkuehl, M., Jonides, J., & Gotlib, I. H. (2012). The everyday emotional experience of adults with major depressive disorder: Examining emotional instability, inertia, and reactivity. Journal of Abnormal Psychology, 121(4), 819–829. https://doi.org/10.1037/a0027978
- Treynor, W., Gonzalez, R., & Nolen-Hoeksema, S. (2003). Rumination reconsidered: A psychometric analysis. Cognitive Therapy and Research, 27(3), 247–259. https://doi.org/10.1023/A:1023910315561
- Türktorun, Y. Z., Weiher, G. M., & Horz, H. (2020). Psychological detachment and work-related rumination in teachers: A systematic review. Educational Research Review, 31, 100354. https://doi.org/10.1016/j.edurev.2020.100354
- Van Laethem, M., Beckers, D. G., Kompier, M. A., Dijksterhuis, A., & Geurts, S. A. (2013). Psychosocial work characteristics and sleep quality: A systematic review of longitudinal and intervention research. Scandinavian Journal of Work, Environment & Health, 39(6), 535–549. https://doi.org/10.5271/sjweh.3376
- Van Laethem, M., Beckers, D. G., Kompier, M. A., Kecklund, G., van den Bossche, S. N., & Geurts, S. A. (2015). Bidirectional relations between work-related stress, sleep quality and perseverative cognition. Journal of Psychosomatic Research, 79(5), 391–398. https://doi.org/10.1016/j.jpsychores.2015.08.011
- Van Laethem, M., Beckers, D. G., van Hooff, M. L., Dijksterhuis, A., & Geurts, S. A. (2016). Day-to-day relations between stress and sleep and the mediating role of perseverative cognition. Sleep Medicine, 24, 71–79. https://doi.org/10.1016/j.sleep.2016.06.020
- Verkuil, B., Brosschot, J. F., Gebhardt, W. A., & Thayer, J. F. (2010). When worries make you sick: A review of perseverative cognition, the default stress response and somatic health. Journal of Experimental Psychopathology, 1(1), jep-009110. https://doi.org/10.5127/jep.009110
- Ware, J. E., Jr. (1999). SF-36 health survey. Spine, 25(24), 3130–3139.
- Watson, D., & Pennebaker, J. W. (1989). Health complaints, stress, and distress: Exploring the central role of negative affectivity. Psychological Review, 96(2), 234–254. https://doi.org/10.1037/0033-295X.96.2.234