
Abstract
Objective
In most countries, vaccine uptake is a voluntary decision. If people experience threats to this freedom, for example, by pro-vaccination media campaigns or government pressure, psychological reactance may be induced. To regain freedom, the opposite behaviour (vaccine refusal) may become more attractive, forming a vaccination barrier. It remains unclear how state reactance fluctuates and how it relates to vaccination intention versus behaviour. Therefore, this pre-registered longitudinal study aimed to gain insight in the changes in state reactance during a COVID-19 vaccination programme and its relationship with vaccine uptake.
Methods
A representative sample of Dutch adults under 60 completed questionnaires before being eligible for vaccination, shortly before they were invited for vaccination, and after the opportunity for vaccination.
Results
Data were analysed using regression analyses (N = 1411). Reactance did not change as hypothesised, but remained stable over time. As hypothesised, reactance predicted lower subsequent vaccination intention. Controlling for intentions, however, reactance did not predict vaccine uptake. Furthermore, reactance predicted lower decision confidence about vaccination, except for people who strongly opposed vaccination.
Conclusion
Reactance has a sustained role in anticipation of a vaccination decision. Although reactance seems to affect the process towards the decision, this does not determine the final choice.
Vaccination is the most effective way to stop the spread of infectious diseases such as COVID-19 (SARS-CoV-2; World Health Organisation, Citation2019, for COVID-19: Levine-Tiefenbrun et al., Citation2021). Scientific support for the effectiveness of new vaccines has yielded policy to aim for high vaccination rates across the globe (for an overview, see: Our World in Data, Citation2021). However, in most countries, whether or not to get vaccinated is a personal, voluntary decision. To stimulate vaccine uptake, governments and medical experts use health communication campaigns and other calls (Lee et al., 2021). The way people respond to these communications may be crucial in determining how effective a vaccination programme is.
Media campaigns that promote vaccination, as any health communication campaign (Quick et al., Citation2018), can be ineffective if people perceive them as a pressure to their autonomous decisions. When people experience such a threat to their freedom by controlling messages or persuasive attempts, this is a perceived freedom threat, to which we will refer as ‘freedom threat’ throughout the paper for the sake of brevity. Freedom threat thus consistently refers to a subjective experience of threatened personal freedom. Psychological Reactance Theory (PRT; Brehm, Citation1966) states that when people experience this threat, it may evoke a state of psychological reactance. This is a form of resistance to the persuasive attempt that is characterised by anger and counterarguing against the message and the messenger (Rains, Citation2013). Reactance drives the person to regain the desired freedom (Brehm, Citation1966), and this focus on taking action to attain a desired outcome makes reactance an approach-motivated state (Mühlberger et al., Citation2020). For the sake of brevity, we will refer to psychological state reactance shortly as ‘reactance’ throughout the article.Footnote1 In order to reinstate freedom, the threatened behaviour becomes more attractive, as has been shown for attitudes across diverse health behaviours (e.g., Dillard & Shen, Citation2005; Quick et al., Citation2018). Applied to vaccine uptake, strongly stimulating citizens to get vaccinated might lead to experienced threat to the freedom to refrain from vaccination, evoking reactance and resulting in suboptimal vaccination rates. Insight in how reactance affects vaccine uptake can help to mitigate it by adapting vaccination campaigns accordingly. Therefore, this article focuses on understanding changes in reactance to the vaccination campaign and its relationship with vaccine uptake.
The role of reactance as a barrier to vaccination has been predominantly based on measurements of vaccination intentions and attitudes, rather than actual behaviour. Previous correlational research has shown that trait reactance (i.e., individual differences in reactance experience across situations; Rosenberg & Siegel, Citation2018) was related to stronger general anti-vaccination attitudes (Hornsey et al., Citation2018; Soveri et al., Citation2020), and to lower COVID-19 vaccination intention specifically (Radosław & Dariusz, Citation2022). Moreover, experiments in which participants read messages advocating vaccination showed that momentary state reactance led to more negative COVID-19 attitudes (Lu & Sun, Citation2022) and lower hypothetical COVID-19 vaccination intentions (Sprengholz et al., Citation2021). Based on existing literature, both reactance as stable trait and as momentary state seem to underlie anti-vaccination attitudes, but the role of momentary state reactance in actual vaccine uptake remains unclear. Therefore, the current study focuses on reactance as a state and vaccine uptake behaviour.
People usually have ample time to decide whether to get vaccinated, which has two (related) consequences for decision-making. First, vaccine uptake is largely intentional (DaCosta Dibonaventura & Chapman, Citation2005; Fall et al., Citation2018). Second, the long period available for deciding implies that factors determining vaccine uptake have time to develop and may fluctuate. Due to more opportunities for overthinking one’s decision, angry emotions, such as those that are part of reactance, could increase as they did during induced rumination (Pedersen et al., Citation2011). However, campaigns and calls may also increase vaccination willingness over time.
Similarly, existing doubts may either be solved or strengthened, increasing or reducing decision confidence. This subjective feeling of certainty about the quality of one’s decisionsFootnote2 helps translating intentions to behaviour (Carlebach & Yeung, Citation2020). Indeed, being confident about one’s course of action is reflected in stronger determination about the decision (Harmon-Jones et al., Citation2009). People can express the extent to which they are confident they will make a good decision (Folke et al., Citation2016), and the degree of confidence even predicts the decisions people make later (Tormala & Rucker, Citation2018). It also guides action within the decision-making process, such that low confidence drives people to seek advice on their choices if they believe they will get high-quality advice (Carlebach & Yeung, Citation2020).
Understanding processes of reactance and doubt over time thus has practical implications for optimising campaigns. Ideally, these campaigns are tuned to counter barriers like reactance at the right moment to resolve hesitation and doubt, or reverse refusal.
However, the path of reactance over time is unknown. Originally, PRT (Brehm, Citation1966) posited that freedom restoration would occur over time, but the later consequences of experienced reactance lack longitudinal empirical support, as also noted by Ratcliff (Citation2019). As such, it remains unclear whether reactance only reduces vaccination intentions or turns into actual vaccine refusal—and at which point. Knowledge about these dynamics would complement PRT with a time dimension, and provide insight in the mechanisms underlying resistance to vaccination. Therefore, the current longitudinal study aims to shed light on how reactance evolves over time and how it relates to later actual vaccination decisions. Specifically, we investigated reactance and its relationships with the intention to get vaccinated and the confidence in this decision, as well as self-reported vaccination behaviour during a COVID-19 vaccination programme. Thereby, this study not only aimed to advance theory about the process underlying reactance and vaccine refusal, but also to gain insights for health campaigns by distinguishing how reactance relates to vaccine hesitancy in the form of lower intentions and confidence, and refusal in the form of lacking vaccine uptake. To the best of our knowledge, this is the first study to address changes in reactance to vaccination over time.
Current study: changes in reactance, doubt about vaccination and vaccine refusal
The first research question investigates reactance over time. Based on construal level theory, distal events are construed in a more abstract way, and proximal events are construed in more concrete terms (Trope & Liberman, Citation2010). When vaccination is still considered in an abstract form rather than in the form of a concrete action, it may provide people with a solution to a threatening situation, a situation in which reactance is less likely to arise (Rosenberg & Siegel, Citation2021). Reactance may only arise when people note that the call to vaccinate has consequences for their autonomy, which is when the actual behaviour of getting vaccinated comes closer and becomes concrete. Additionally, reactance becomes more likely when the threatened freedom is more self-relevant and extensive (Rosenberg & Siegel, Citation2018). As closer consequences loom larger (for a review on temporal discounting and health behaviour, see: Story et al., Citation2014), reactance may accordingly rise when the vaccination date approaches. Moreover, in The Netherlands, exposure to vaccination communication went from more general messages in the media, ‘We should vaccinate’, to the prospect of personal invitations by the government, gradually increasing self-relevance of vaccination communication. Therefore, Hypothesis 1 states that on average, reactance increases over time, from before being eligible for vaccination to being part of the target group that is about to receive an invitation for vaccination.
The second research question investigates whether reactance negatively predicts vaccination intentions. As reactance increases the attractiveness of behaviours opposing the message (Mühlberger et al., Citation2020, Rosenberg & Siegel, Citation2018) and involves arguing against the message (Rains, Citation2013), Hypothesis 2a posits that reactance and vaccination intention are negatively associated at the same time, and Hypothesis 2b states that reactance negatively predicts vaccination intention at the subsequent measurement.
The third research question investigates whether reactance relates to stronger determination about the choice to vaccinate. Reactance motivates people to take action to retain their freedom. Because of this focus on attaining a desired outcome, it is characterised as an approach-motivational state (based on approach behavioural and neurological patterns in experiments by Mühlberger et al., Citation2020). Likewise, anger is an approach-motivational emotion (Carver & Harmon-Jones, Citation2009). Another correlate that is part of approach motivation is stronger determination, confidence to pursue a decision (Harmon-Jones et al., Citation2009). Hypothesis 3a therefore states that reactance relates positively to confidenceFootnote3 in the decision to (not) get vaccinated at the same measurement. Moreover, the experience of reactance might further convince people of their choice. Hypothesis 3b states that reactance also positively predicts confidence about the vaccination decision at the subsequent measurement.
The fourth and final research question investigates whether reactance results in vaccine refusal, either directly by reducing vaccine uptake rates, or indirectly via lower vaccination intentions. The mediation via intention is exploratory, but it is expected in Hypothesis 4 that any relationship between reactance and vaccine uptake is negative, as doing the opposite of the target behaviour is a way to directly restore freedom (Quick & Stephenson, Citation2007), and this would be the behavioural consequence of the finding that reactance to vaccination predicted lower hypothetical vaccination intentions (Sprengholz, Citation2022).
Study context
The four research questions were examined in a representative sample of the population of healthy 18–59-year-old inhabitants of The Netherlands. In the Netherlands, COVID-19 vaccination is free and voluntary. The Dutch government announced in January 2021 that all citizens would be invited for vaccination in phases: the most vulnerable and older aged people first, followed by younger, healthy people. At the start of data collection, in April 2021, people of 60 years and older and those with severe health issues had already been invited. Vaccination invitations were issued by an online announcement and by letter, inviting a person to schedule their vaccination appointment (online or by phone). If people made this appointment, this meant that they took action to book the appointment, and they agreed on a time and location to get the vaccine. At the time of data collection, it was not possible to get vaccinated without an appointment, and when an appointment was scheduled, this almost always meant that people got their vaccination (around 3% no-shows, De Limburger et al., Citation2021).
To study real-life decisions (as opposed to hypothetical), the measurements were spread from when participants were not yet eligible for vaccination till after the possibility to schedule one’s vaccination. Specifically, the first measurement (Time 0; T0) took place when vaccines were available to some parts of the public but not yet for study participants. The second measurement (Time 1; T1) took place after 1 to 3 months, when participants were almost eligible for vaccination. This timing was personalised according to age, so when the government publicly announced that people of a certain age group would be invited in about one week, they received the T1 questionnaire. This was sent out in age groups per 10 years (i.e., 40–49; 50–59) for feasibility. The third measurement (Time 2; T2) took place after all participants were given the opportunity to schedule a vaccination appointment. This always was the first COVID-19 vaccination (i.e., no boosters).
Method
Transparency and openness
In this article, we report the sample size, all data exclusions and all measures that were included in the study. This study was pre-registered at the Open Science Framework, see https://osf.io/j6fv9 for information regarding data collection, and https://osf.io/dqfkh for the hypotheses and analysis plan. The data and analysis code are available on http://doi.org/10.17605/osf.io/X9DTK, including a report of additional research questions that fall outside the scope of this article (https://osf.io/vmr62/); the English translations of the original Dutch questionnaires are reported in the Methods section. The study was conducted in accordance with the ethics code for research involving humans of the World Medical Association (Declaration of Helsinki), and was reviewed and approved by the ethics committee of the authors’ institution (#ECSS-2021-025).
Participants
Participants were recruited from the FlyCatcher panel, a Dutch commercial online survey panel that consists of over 10.000 adults who have voluntarily declared to participate via active informed consent. The targeted sample of Dutch citizens was stratified on sex, age, education level and province to reflect the Dutch population of 18–59 years old. Panel members were approached via e-mail to participate in the current study, for which a unique hyperlink was provided. Participants received gift cards of their choice for their participation.
See for participant flow, attrition and exclusions (based on the pre-registered criteria of incomplete questionnaires, bad data quality based on standard FlyCatcher panel procedures, and having received vaccination at T1 already, because this indicates that participants had made their decision whether to get vaccinated. Consequently, their responses at T1 did not reflect the anticipation on the decision that this study was testing). The 865 participants who completed all three questionnaires had a mean age of 41.61 (SD = 11.73), 47.17% identified as women, and the other 52.82% as men. Sample characteristics per wave are presented in . This table also shows that the sample characteristics are distributed largely in line with the Dutch population.
Figure 1. Participant flow and attrition. Note. Data quality was assessed by the panel agency Flycatcher via their standard procedure based on open answers, consistency of answers, response time and straight lining.
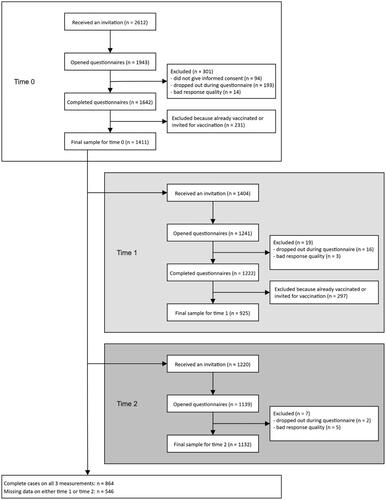
Table 1. Characteristics of the research sample.
The sample that completed all questionnaires was compared to the sample that had missing data on the focal variables. Missing data occurred only when a participant was not included in a data collection wave, as a response was mandatory on all items of the focal variables. Participants who completed all questionnaires scored higher on reactance, and lower on vaccination intention and confidence compared to those with missing data (independent samples t-test for reactance: t = 2.78, p = .005; for intention: t = −4.79, p < .001 and for confidence: t = −2.53, p = .012). Furthermore, participants with complete data were more likely to report not getting vaccinated (χ2 (1) = 54.76, p < .001) than participants who had missing data. Specifically, participants who missed T1 only returned for the final questionnaire if they had scheduled the vaccination appointment or already got vaccinated. In sum, it seemed that complete data was more likely for participants who were more negative about vaccination. One reason for this pattern is that the 297 participants who already scheduled their vaccination appointment at T1 had to be excluded, and they were arguably relatively less reactant and more confident and intending to get vaccinated. In addition, reactance itself could be a reason for completing the questionnaires to express one’s negative opinion, but the randomness of missing data is not a testable assumption.
The attrition over time is potentially influential for the analysis of the fluctuation of reactance over time (research question 1). We followed the recommendation for longitudinal data by Gad and Abdelkhalek (Citation2017) to use complete cases only, as mentioned in the pre-registration, to minimise the possibility that any pattern is caused by biased selection in later waves. In the other analyses, as many of the existing data as possible are used without creating data that may introduce additional biases (following Gad & Abdelkhalek, Citation2017; Hayes, Citation2017).
Materials
All questionnaires were administered in Dutch. Brief scales were used to minimise attrition. For consistency, all scales were transformed to a 101-point slider scale ranging from 0 = completely disagree to 100 = completely agree.
Vaccine uptake was assessed with the multiple-choice question ‘Have you been vaccinated against the coronavirus disease?’ The question had four answer options: ‘No and I have also not made an appointment’, coded as ‘Not vaccinated’ (0); ‘Yes, I am fully vaccinated’; ‘Partly, I have had one vaccination but I need to get a second one’; ‘No, but I have made an appointment’, all three coded as ‘Vaccinated or planned’ (1), with ‘planned’ meaning that the appointment was scheduled, since descriptive research showed that making the appointment almost always was followed by vaccine uptake (de Limburger et al., Citation2021).
Vaccination intention was measured with one item, ‘Do you plan on getting vaccinated against the coronavirus disease when you are invited to do so?’, answered on the scale from 0 to 100 with anchors ‘definitely no’ and ‘definitely yes’.
Confidence in the vaccination decision was measured by a 3-item scale to reflect the subjective experience of relative uncertainty or certainty about the decision to get vaccinated. It consisted of three items: ‘I feel uncertain about the decision to get vaccinated against the coronavirus disease’ (reversed), ‘I know what I’m up for if I get vaccinated against the coronavirus disease’, and ‘I find it hard to decide whether getting vaccinated against the coronavirus disease is the best decision for me’ (reversed). Reliability was acceptable (T0 α = .74, at T1 α = .73).
Freedom threat as subjective experience was captured by a mean score of three freedom threat items, based on Dillard and Shen perceived threat to freedom scale (2005), which showed good convergent validity with reactance (Shen & Dillard, Citation2005). Their items often refer to ‘the message’, which was replaced by ‘the governments’ call to get vaccinated’. The item mentioning feeling pressure was left out because it closely resembled the item about threat to freedom to choose when translated. The items were: ‘I think the governments’ call to get vaccinated is manipulative’; ‘The governments’ call to get vaccinated makes me feel like I cannot decide myself’; ‘The governments’ call to get vaccinated threatens my freedom to choose’. Reliability as assessed by Chronbach’s alpha was excellent both at T0 and T1, α = .94.
Reactance, indicating a resistant reaction to the vaccination campaign, consisted of a mean score of three reactance items, based on the Experience of Reactance subscale of the Salzburger State Reactance Scale, which had good convergent and divergent validity (Sittenthaler et al., Citation2015). The phrase ‘reaction of the landlord’ was replaced by ‘governments’ call to get vaccinated’, and the item asking about perceived threat to freedom was not included because it had the lowest factor loading and this was covered by our freedom threat scale. The items were: ‘I am frustrated about the governments’ call to get vaccinated’; ‘The governments’ call to get vaccinated annoys me’; ‘I am offended/disturbed by the governments’ call to get vaccinated agree’. Reliability was excellent, at T0 α = .97, at T1 α = .96.
Because the scale for confidence was newly developed and we slightly adapted the original wording of the freedom threat and reactance scales, the one-factor structure of each scale was tested in a confirmatory factor analysis (CFA). For all three scales, the fit was good (at both measurements, Comparative Fit Index (CFI) > .999, Root Mean Square Error of Approximation (RSMEA) < .001, Standardised Root Mean Square Residual (SRMR) < .001), see for the factor loadings. As pre-registered, this allowed for including confidence as a unitary construct.
Table 2. Factor loadings on confidence, freedom threat and reactance scales.
Procedure
Data collection took place in 2021. The first measurement (T0) was sent out on April 13th and remained open until April 22nd. Data from the second measurement wave (T1) were collected between May 3rd and June 18th. Participants received the questionnaire as soon as the government announced that their birth decade would be invited for vaccination. Data collection for the third measurement wave (T2) took place between July 19th and August 2nd.
Participants first answered a verification question to prevent other people with access to their e-mail from participating. They completed the questionnaires on the Flycatcher website. Participants saw the different scales on separate pages in the above-described order (freedom threat and reactance on one page) and could not change answers on previous pages. All questions required an answer and automatic routeing was applied. The measures reported in this paper were administered as part of a larger questionnaire that took around 10 min to complete at T0 and T1, and around 2 min at T2.
Analyses
All analyses were conducted in R (version 4.1.1, R Core Team, Citation2021). The pre-registered initial model to test all hypotheses simultaneously using structural equation modelling (without transformations or additions) had a bad fit as indicated by the robust fit statistics (CFI = .287, RMSEA = .201, SRMR = .201), and the covariance matrix of the residuals of the observed variables (theta) was not positive definite. As pre-registered, the model was adapted by adding parameters based on the modification indices in a step-wise fashion until an acceptable fit was reached and estimates were obtained using the robust WLSMV estimator, but the strong correlations between observed variables and skewed distributions remained problematic so that not all paths could be estimated. For a step-by-step explanation, see the online supplemental materials (https://osf.io/vmr62/). Therefore, the hypotheses were tested in separate analyses, staying as close to the initial plan as possible by obtaining bootstrapped estimates where applicable and combining the effectsFootnote4 on vaccine uptake as predicted in Hypothesis 4 in one model.
Hypothesis 1, the expectation that reactance would increase over time, was tested in a linear mixed-effects model using the package ‘lme4’ (Bates et al., Citation2014) with reactance as outcome variable, time (T0; T1) as predictor, and random intercepts per participant. Confidence intervals (CIs) were obtained at the 95% level by parametric bootstrapping with 10.000 samples using the ‘lme4’ package. The log-transformed scores of reactance were used to deal with the violation of normality of the outcome variable.
Hypothesis 2a, higher reactance is related to lower vaccination intentions, was tested in two-sided pairwise Spearman correlations (to obtain estimates for skewed distributions, package ‘stats’; R Core Team, Citation2021) between reactance and vaccination intention at both T0 and T1. Hypothesis 2b, higher reactance predicts later lower vaccination intentions, was tested with a linear regression using the package ‘stats’ with vaccination intention at T1 as outcome, and reactance at T0 and vaccination intention at T0 as predictors. Bias-corrected bootstrapped 95% CIs were obtained from 10.000 bootstrapping samples using the package ‘boot’ (Canty & Ripley, Citation2021).
Likewise, Hypothesis 3a, higher reactance is related to higher confidence, was tested using pairwise Spearman correlations between Reactance and Confidence at both T0 and T1, and Hypothesis 3b, higher reactance predicts higher confidence at a later wave, was tested using linear regression with T1 Confidence as outcome, and T0 reactance and T0 confidence as predictors, and interpreted using the same bootstrapped CIs as for Hypothesis 2b.
Hypothesis 4, that reactance had a negative direct or indirect effect on vaccine uptake, was tested in a mediation model using the PROCESS macro model 4 (PROCESS version 4.0.1, Hayes, Citation2017). Thus, reactance at T0 served as predictor (X) and vaccine uptake behaviour at T2 as outcome (Y), estimated by logistic regression. Intention at T1 (centered) was added as mediator (M); and intention at T0 as covariate to M as well as Y. Bias-corrected bootstrap CIs were obtained based on 10,000 bootstrap samples, and cases with missing data were automatically deleted. In addition, mean reactance scores for participants who got vaccinated or had a vaccination appointment vs. those who did not, were explored in an independent sample t-test on log-transformed T0 reactance scores.
Results
Descriptive statistics
presents the means for all variables that were part of the hypothesis tests as well as their mutual correlations. To check the assumption that freedom threat was positively associated with reactance, Spearman’s correlations between freedom threat and reactance scores were tested at both T0 and T1. As predicted, freedom threat and reactance were positively and strongly associated at both measurements, see .
Table 3. Descriptive statistics of the measured variables at T0, T1 and T2.
Research question 1: Does reactance increase over time?
The linear mixed-effects model showed that reactance scores did not change significantly from T0 to T1 as zero lies within the bootstrapped confidence interval (B = 0.004, SE = 0.018, 95% CI [−0.03, 0.04]), so reactance remained stable (see ). This means that Hypothesis 1 was not supported, reactance did not increase over time.
Research question 2: Does reactance negatively relate to vaccination intentions?
There was a significant and strong negative correlation between reactance and intention at both measurements (see ). This confirmed Hypothesis 2a that participants with higher reactance on average had lower vaccination intentions.
Hypothesis 2b tested the effect of reactance on later intentions. The overall linear regression model significantly predicted intentions at T1 (adjusted R2 = .83, F (2, 922) = 2230.00, p < .001). Vaccination intention at T0 significantly and positively predicted vaccination intention at T1 (B = 0.85, SEB = 0.02, β = 0.86, 95% CI [0.78, 0.90]) so that participants who started with a high vaccination intention were also the ones with higher intentions later. Reactance at T0 had a significant negative effect on subsequent vaccination intention at T1 (B = −0.07, SEB = 0.02, β = −.06, 95% CI [−0.14, −0.01]), so higher reactance predicted lower intention. This confirmed Hypothesis 2b; participants with higher reactance at the start of the vaccination programme on average had lower vaccination intentions right before receiving their invitation, controlling for earlier intentions.
Research question 3: Does reactance relate to higher confidence in the choice that is under freedom threat?
Reactance correlated significantly with confidence but in the opposite direction as expected: there was a strong negative association (see ). This means that Hypothesis 3a was not supported; higher reactance was on average related to lower instead of higher confidence.
Hypothesis 3b tested this relationship across timepoints. The overall regression model significantly explained confidence at T1 (adjusted R2 = .53, F (2, 922) = 512.80, p < .001). Confidence at T0 predicted confidence at T1 significantly and positively (B = 0.63, SEB = 0.02, β = .67, 95% CI [0.58, 0.68]), indicating that participants who felt more confident at first, were on average also more confident later. Reactance at T0 significantly and negatively predicted confidence at T1 (B = −0.09, SEB = 0.02, β = −.11, 95% CI [−0.13, −0.04]), indicating that higher reactance at first resulted in lower confidence at the subsequent measurement, controlling for earlier confidence. Thus, Hypothesis 3b was not supported; participants with higher reactance did on average not get more but less confident in their vaccination decision.
Research question 4: Does reactance relate to vaccine refusal directly or via intentions?
Participants’ intention to get vaccinated seemed to be closely related to vaccine uptake: only 23 people out of the 708 who got vaccinated and had complete data did so without having a positive vaccination intention (lower than 50, the scale midpoint) right before their invitation; and also only 23 out of 157 who did not get vaccinated opposingly had a positive intention (higher than 50). This difference is also evident in average intention strength at T1 for participants who got vaccinated or not: participants who got vaccinated or had scheduled their appointment had an average intention of 91.84 (SD = 16.00), while those who did not had an average intention of 20.20 (SD = 27.11).
Hypothesis 4 tested whether higher reactance was related to lower likelihood of vaccine uptake, potentially via lower vaccination intentions (see ). The overall mediation model significantly predicted the mediator, vaccination intention, as well as the outcome, vaccine uptake (see for the results). Specifically, vaccination intention at T1 significantly and positively predicted vaccine uptake. However, in contrast to the results of Hypothesis 2b, the path from reactance at T0 to intentions to get vaccinated at T1 was no longer significant in this smaller sample of N = 865 complete cases, controlled for intentions at T0. Correspondingly, higher reactance was not significantly directly related to vaccine uptake, controlling for intentions. The indirect path of reactance on vaccine uptake via intentions was not significant either. This means that there was no support for Hypothesis 4 that higher reactance predicts lower vaccine uptake. Thus, although the average reactance for participants who did not get vaccinated (M = 54.40, SD = 32.54) was higher than the average reactance for participants who got vaccinated or had a vaccination appointment (M = 12.82, SD = 21.95) as explored in an independent sample t-test (for log-transformed reactance: t(287.73) = 19.67, p < .001, r = .76), when controlling for intentions in the model, this did not explain their vaccination decision.
Figure 2. Indirect effects of reactance on vaccine uptake via vaccination intention. Note. Intention T0 effects on vaccine uptake are reported at high (+1 SD) and low (−1 SD) confidence. The coefficients represent B-weights, and paths to the categorical outcome variable are indicated with odds ratios. Dotted lines indicate included effects of the covariate (intentions at T0). * p < .05, as derived from bootstrapped CIs.
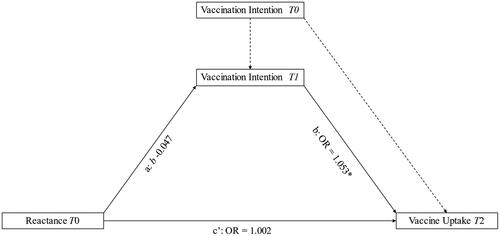
Table 4. Regression table for research question 4.
Exploratory analyses on the relationship between reactance and confidence
The results of research question 3 showed an unexpected negative relationship between reactance and confidence. However, most participants intended to get vaccinated, and reactance may only lead to stronger determination for those with low vaccination intentions to begin. This was tested in an exploratory moderation analysis using PROCESS macro model 1 (Hayes, Citation2017). The coefficients of this linear regression analysis were obtained from 10000 bias-corrected bootstrapped samples. Confidence at T1 was regressed on reactance at T0 with intentions at T0 as the moderator. The model significantly explained confidence (R2 = .34, F(3, 921) = 158.36, p < .001), and the moderation significantly improved this fit (R2change = .06, F(1, 921) = 85.71, p < .001). Intentions significantly moderated the effect of reactance on confidence (B = −0.13, SE = 0.02, 95% CI [−0.17; −.09]). Specifically, for participants with a higher vaccination intention, higher reactance predicted lower confidence in the vaccination decision (1 SD above the mean of vaccination intention: B = −6.98, SE = 0.59, 95% CI [−8.13; −5.83]), whereas for participants with a lower vaccination intention, higher reactance predicted higher confidence (1 SD below the mean of vaccination intention: B = 2.28, SE = 0.87, 95% CI [0.57; 3.98]). Thus, reactance seemed to instil hesitation in those who were tending to vaccination and determination in those who were tending to refuse vaccination.
Exploratory analyses with control variables
As an additional check of the robustness of the main statistical analyses, the statistical models were analysed with control variables related to vaccination intention and uptake. The addition of control variables increases internal validity by limiting the influence of extraneous variables, thereby controlling for confounding effects of, for example, demographic factors or health-related influences. The included controls were measured at T0 and related to demographic factors that were predictive of COVID-19 vaccine uptake (gender, age, education level, spirituality; Galanis, Citation2021; Robertson et al., Citation2021) and health and perceived threat of COVID-19 (health, worry about COVID-19, risk of getting infected by COVID-19; Galanis, Citation2021; Wong et al., Citation2020). This selection was based on the scientific literature at the moment of data collection and aimed to represent a wide but relevant range of possible influential variables on the decision to get vaccinated against COVID-19.
The pattern of results and associated conclusions concerning the hypotheses remained the same for research questions 1, 2 and 3. For research question 4, one path of the mediation model became significant. That is, reactance related negatively to vaccination intention, the exact same effect as was shown in the simple correlation test of research question 2. As a result, the indirect effect of reactance on vaccine uptake via intentions became significant as well. The exact outcomes of the analyses including control variables are reported in the online supplementary materials (https://osf.io/vmr62/).
Discussion
This study investigated changes in reactance across two time points during the COVID-19 pandemic prior to the invitation to vaccinate. State reactance, vaccination intention, confidence in the vaccination decision and reported voluntary COVID-19 vaccine uptake were studied over 4 months in a representative sample of of Dutch adults under 60. Reactance was unexpectedly stable from before participants were targeted by the vaccination campaign to the week prior to receiving a vaccination invitation. Higher reactance predicted later lower vaccination intentions and also lower confidence about the vaccination choice. Only participants with high reactance and, moreover, no vaccination intention felt more confident to refuse vaccination. Finally, the assumed relationship between reactance and vaccine uptake was not structurally confirmed.
Reactance and attitude formation during a vaccination programme
This study contributes to the field of health psychology and communication by measuring reactance at two points during a COVID-19 vaccination campaign, with the remarkable finding that reactance remained stable over a 3-month period. The contrasting hypothesis that reactance would increase with time was based on the idea that people would interpret the call to vaccinate as a concrete assignment to do something compared to a more abstract solution interpretation earlier in time (Trope & Liberman, Citation2010) that people desire in a threatening situation (Rosenberg & Siegel, Citation2021). The sustained reactance levels may directly reflect ongoing freedom threat perceptions, as the call to get vaccinated did not change and remained relevant throughout the decision-making process. This explanation would imply that reactance seems to remain active once evoked in a given situation.
An alternative explanation for the notable stability is a strong relationship between state and trait reactance. The current study measured state reactance during the vaccination campaign, so note that explanations involving trait reactance are hypothetical. Still, the reported reactance and freedom threat levels might partly reflect individual differences in trait reactance, which would not fluctuate over time. Trait reactance, like state reactance, is related to the perception of freedom threat, but rather seen as antecedent than consequence of freedom threat experiences (Quick et al., Citation2011). For instance, a certain level of trait reactance might have been a condition for state reactance to arise. Indeed, trait reactance has been related to lower COVID-19 vaccination intentions (e.g., Radosław & Dariusz, Citation2022). Moreover, trait reactance might have influenced to what extent efforts to mitigate reactance in the vaccination campaign were effective, as research showed that freedom evoking strategies did not work similarly for participants with different levels of trait reactance (Richards et al., Citation2021). Thus, state reactance to diffuse, long-term freedom threats such as a large vaccination campaign, may be partly intertwined with trait reactance.
Alternatively, the expected increase in state reactance may have been masked by opposing simultaneous situational changes, which intensified reactance early in time, and suppressed it later on. Specifically, the start of the vaccination programme was paired with safety concerns about the vaccines (Fall et al., Citation2018). These potential adverse health effects made vaccination highly self-relevant, a source of higher reactance (Rosenberg & Siegel, Citation2018). In contrast, later in the vaccination programme, the encouraging outlook that vaccination would bring more freedom (e.g., going on a holiday), and matching high vaccination intentions, may have mitigated reactance (Sprengholz et al., Citation2021).
However, values of confidence and vaccination intention also remained relatively unchanged, requiring a more general explanation. The intentionality of vaccine uptake suggests that the actual decision is already formed early on, before the targeted campaign started. Indeed, Sanders et al. (Citation2021) studied vaccination intentions in The Netherlands until vaccines became available for the general population, and showed an increase in vaccination intention right before they were made available. The current study subsequently observed steady intentions in line with self-reported behaviour, suggesting that people seem to make their choice well ahead of the crucial point (when the invitation arrives) instead of afterwards, as Sanders and colleagues suggested. A possible explanation for the stability in confidence and intention is that both stem from a general attitude about the choice to get vaccinated against COVID-19 and the communication strategy, as these attitudes can be relatively strong and stable over time (Petty & Krosnick, Citation1995).
Implications for psychological reactance theory (PRT)
The finding that reactance relates to later lower vaccination intentions but not robustly to higher confidence and less uptake suggests refinements to improve PRT (Brehm, Citation1966). Strong reactance only predicted higher confidence for individuals who were already tending not to get vaccinated. Although this exploratory finding should be interpreted with caution, this is in line with the approach-motivational character of reactance that instils determination (Mühlberger et al., Citation2020), and with experiments showing higher reactance to vaccination when vaccination intentions are low (Sprengholz et al., Citation2021). However, for all other participants, reactance led to lower confidence in their decision, so reactance does not necessarily increase determination. Given the strong default to comply with pro-vaccination messages (Sanders et al., Citation2021), doubting this default signals resistance as well. The low confidence may reflect the struggle of ambivalence between acting based on the best health protection or one’s irritation about the way this is communicated.
Furthermore, the lacking predictive effect of reactance on vaccine uptake behaviour casts doubt on the assumption that reactance translates into boomerang behaviour (Mühlberger et al., Citation2020). While reactance co-occurred with lower vaccination intentions, it did not robustly predict direct freedom restoration in the form of refusing vaccination. A possible explanation is that refusing vaccination may be an excessive sacrifice to regain freedom—especially since most people hold favourable attitudes towards vaccination and COVID-19 posed a considerable health threat. Freedom may instead be restored indirectly in exercising or searching out related free health behaviours (Quick & Stephenson, Citation2007). Thus, these field results imply that caution is warranted when making claims about the detrimental effects of reactance on vaccine uptake, since they seem to focus more on vaccine hesitancy.
Practical implications
Even when reactance does not directly influence vaccine uptake, it did predict intentions in anticipation of a vaccination invitation. This indicates the importance of preparing the vaccination campaign well. For instance, spreading clear and accessible information as early as possible may help to boost vaccination intentions and reach high vaccination rates as an efficient way out of a pandemic (World Health Organisation, Citation2019).
Furthermore, the stability of reactance and intentions points out that freedom threat is not resolved by automatically. Instead, its impact may linger. Similarly, indirect freedom restoration may involve acting out on related (health) behaviours, with negative consequences for the spread of infectious diseases. For instance, Sprengholz et al. (Citation2022) showed that reactance to mandatory vaccination scenarios decreased intention to take influenza vaccines and intention to follow other COVID-19 protective behaviours. Thus, it is important to prevent reactance by minimising pressure (Quick & Stephenson, Citation2007) from the start of a vaccination campaign. Before implementation, the ethical considerations of adapting communication as to influence decision-making should be carefully weighed.
The small observed effects are no exception in psychological research (Schäfer & Schwarz, Citation2019), but do indicate that people’s vaccination decision comes with many simultaneous considerations. However, for behaviour across a whole population, such as preventive health behaviour in general, even small effects may bear considerable implications. With the currently studied diverse sample, these practical lessons can be extended to a wide public. Furthermore, when generalising the findings, it should be noted that the results reflect the situation in The Netherlands, with relatively little pressure in the vaccination campaign at the time of data collection (e.g., using expressions like: ‘It’s your choice, so make sure you’re well-informed’). Although this is similar in other countries’ vaccination campaigns, people who experience stronger personal threat may respond differently.
Limitations and future directions
This study advanced insight in the process of reactance to vaccination campaigns thanks to its unique combination of a longitudinal design, representative large sample and measurement of both intention and behaviour. However, this study is not without its limitations. It is important to bear in mind possibly negatively biased averages created by selective response of participants who wanted to vent their disagreement with vaccination, as these participants seemed more likely to complete all questionnaires. This may have led to artificially high perceptions of freedom threat, and artificially low vaccination intentions. We did not see reactance arise, implying that it already had unfolded earlier. Still, it remains to be investigated at what point it did: was it the result of communication around the development of vaccines, or perhaps strengthened by other COVID-19 measures? Furthermore, the small gap between vaccination intentions and behaviour may have been articifially close by the commitment implied by reporting intentions, and because behaviour was self-reported. Still, the question-behaviour effect is expected to have been minimal because vaccination already was an often-discussed public topic. Besides, reporting errors of behaviour were reduced as far as possible by the dichotomous question format (yes, no) and because a vaccination appointment is a rare event, easy to recall (DaCosta Dibonaventura & Chapman, Citation2005).
An additional note for interpretation and further research is that freedom threat was not experimentally manipulated, so causality inferences are based on time order and theoretical assumptions. An experiment with different and more extreme communication styles may give fruitful applied insights on how to deal with reactance in different phases of vaccination or other health campaigns, and replicate distinctive effects of reactance on doubt and final choice. The current surveys went out before participants received their invitation, and thus did not test the impact of the vaccination invitation specifically, but instead tested the impact of the vaccination campaign more broadly. Future studies could extend measures to the phase following a personal mandate. Clearly, the possibilities for experimental studies are bounded by ethical constraints.
Future research to the dynamics of state reactance could extend insight in the fluctuation pattern by including fine-grained change measures like experience sampling and measurements between a personal invitation and the enactment of the choice, or study the development of reactance by adding baseline measures before a campaign starts. Future studies addressing the important topic of vaccine uptake may continue research to dynamic decision-making and investigate the fluctuations of other barriers to vaccination, such as distrust (Soveri et al., Citation2020) and safety concerns (Hornsey et al., Citation2018). Research beyond vaccine uptake may also benefit from approaching health behaviour change as a process. Many behaviours that improve health or prevent illness are not constrained by time, but become more beneficial if they are executed sooner or more frequently rather than later or never (ranging from exercise and drinking less alcohol to taking medicines and visiting the dentist). Measuring how predictors of these behaviours fluctuate could increase insight in the time dimension of health psychology theories like the Health Belief Model (adding to Fall et al., Citation2018).
Conclusion
This study offers a process-perspective on reactance in anticipation of the decision whether to get vaccinated. Reactance to vaccination calls arises early on and does not fade away. With this longitudinal approach of both self-reported experiences and behaviour in a diverse sample, this study implies that reactance relates more robustly to hesitancy about vaccination than vaccine refusal, instilling doubt instead of opposite determination. This nuances predictions for vaccine uptake based on approach-motivation and Psychological Reactance Theory. Vaccinations are the most promising way out of a pandemic, but they mostly also are a free decision, which brings challenges throughout the vaccination campaign.
Transparancy and Data Availability
This study was pre-registered at the Open Science Framework, see https://osf.io/j6fv9 for information regarding data collection, and https://osf.io/dqfkh for the hypotheses and analysis plan. The data, analysis code and supplemental materials are available on http://doi.org/10.17605/osf.io/X9DTK; including a report of additional research questions that fall outside the scope of this paper. (https://osf.io/vmr62/). In this article, we report the sample size, all data exclusions and all measures that were included in the study. We have no conflicts of interest to disclose.
Disclosure Statement
The authors report no conflict of interest.
Additional information
Funding
Notes
1 The tendency to experience reactance also varies as a trait between individuals (Rosenberg & Siegel, Citation2018); when this trait reactance is discussed, it will be specified.
2 This confidence in one’s decision is fully termed ‘decision confidence’. In the current article, it always applies to confidence in the decision to get vaccinated against COVID-19, so it is described shortly as ‘confidence’ throughout the article.
3 Decision confidence covers a continuum from experienced uncertainty to certainty, and was phrased from the perspective of uncertainty in the pre-registration (e.g., changes described as decreased uncertainty instead of increased confidence). To facilitate interpretation, the term confidence is used throughout the article.
4 The word ‘effect’ is used to indicate longitudinal, statistical effects and does not imply causality, since there was no experimental control.
References
- Bates, D., Mächler, M., Bolker, B., & Walker, S. (2014). Fitting linear mixed-effects models using lme4. arXiv preprint arXiv:1406.5823. https://doi.org/10.18637/jss.v067.i01
- Brehm, J. W. (1966). A theory of psychological reactance. Academic Press.
- Canty, A., & Ripley, B. (2021). boot: Bootstrap R (S-Plus) Functions. R package version 1.3-28. https://CRAN.R-project.org/package=boot.
- Carlebach, N., & Yeung, N. (2020). Subjective confidence acts as an internal cost-benefit factor when choosing between tasks. Journal of Experimental Psychology: Human Perception and Performance, 46(7), 729–748. https://doi.org/10.1037/xhp0000747
- Carver, C. S., & Harmon-Jones, E. (2009). Anger Is an approach-related affect: Evidence and implications. Psychological Bulletin, 135(2), 183–204. https://doi.org/10.1037/a0013965
- DaCosta Dibonaventura, M., & Chapman, G. B. (2005). Moderators of the intention-behavior relationship in influenza vaccinations: Intention stability and unforeseen barriers. Psychology and Health, 20(6), 761–774. https://doi.org/10.1080/14768320500183368
- De Limburger, Kalkman N., & Scholenberg, M. (2021). Verspilling vaccins lager dan verwacht: ‘We hebben wat echt fantastische prikkers”. https://www.limburger.nl/cnt/dmf20210129_92739286
- Dillard, J. P., & Shen, L. (2005). On the nature of reactance and its role in persuasive health communication. Communication Monographs, 72(2), 144–168. https://doi.org/10.1080/03637750500111815
- Fall, E., Izaute, M., & Chakroun-Baggioni, N. (2018). How can the health belief model and self-determination theory predict both influenza vaccination and vaccination intention ? A longitudinal study among university students. Psychology and Health, 33(6), 746–764. https://doi.org/10.1080/08870446.2017.1401623
- Folke, T., Jacobsen, C., Fleming, S. M., & De Martino, B. (2016). Explicit representation of confidence informs future value-based decisions. Nature Human Behaviour, 1, 0002. https://doi.org/10.1038/s41562-016-0002
- Gad, A. M., & Abdelkhalek, R. H. M. (2017). Imputation methods for longitudinal data: A comparative study. International Journal of Statistical Distributions and Applications, 3(4), 72–80. https://doi.org/10.11648/j.ijsd.20170304.13
- Galanis, P. (2021). Predictors of COVID-19 vaccination uptake and reasons for decline of vaccination: A systematic review. medRxiv, https://doi.org/10.1101/2021.07.28.21261261
- Harmon-Jones, E., Harmon-Jones, C., Abramson, L., & Peterson, C. K. (2009). PANAS positive activation is associated with anger. Emotion, 9(2), 183–196. https://doi.org/10.1037/a0014959
- Hayes, A. F. (2017). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach. Guilford Publications.
- Hornsey, M. J., Harris, E. A., & Fielding, K. S. (2018). The psychological roots of anti-vaccination attitudes: A 24-nation investigation. Health Psychology, 37(4), 307–315. https://doi.org/10.1037/hea0000586
- Lee, J.-K., Bullen, C., Ben Amor, Y., Bush, S. R., Colombo, F., Gaviria, A., Karim, S. S. A., Kim, B., Lavis, J. N., Lazarus, J. V., Lo, Y.-C., Michie, S. F., Norheim, O. F., Oh, J., Reddy, K. S., Rostila, M., Sáenz, R., Smith, L. D. G., Thwaites, J. W., … Xue, L. (2021). Institutional and behaviour-change interventions to support COVID-19 public health measures: A review by the Lancet Commission Task Force on public health measures to suppress the pandemic. International Health, 13(5), 399–409. https://doi.org/10.1093/inthealth/ihab022
- Levine-Tiefenbrun, M., Yelin, I., Katz, R., Herzel, E., Golan, Z., Schreiber, L., Wolf, T., Nadler, V., Ben-Tov, A., Kuint, J., Gazit, S., Patalon, T., Chodick, G., & Kishony, R. (2021). Initial report of decreased SARS-CoV-2 viral load after inoculation with the BNT162b2 vaccine. Nature Medicine, 27(5), 790–792. https://doi.org/10.1038/s41591-021-01316-7
- Lu, F., & Sun, Y. (2022). COVID-19 vaccine hesitancy: The effects of combining direct and indirect online opinion cues on psychological reactance to health campaigns. Computers in Human Behavior, 127, 107057. https://doi.org/10.1016/j.chb.2021.107057
- Mühlberger, C., Klackl, J., Sittenthaler, S., & Jonas, E. (2020). The approach-motivational nature of reactance—Evidence from asymmetrical frontal cortical activation. Motivation Science, 6(3), 203–220. https://doi.org/10.1037/mot0000152
- Our World In Data. (2021, September). COVID-19 vaccination policy. https://ourworldindata.org/grapher/covid-vaccination-policy
- Pedersen, W. C., Denson, T. F., Goss, R. J., Vasquez, E. A., Kelley, N. J., & Miller, N. (2011). The impact of rumination on aggressive thoughts, feelings, arousal, and behaviour. British Journal of Social Psychology, 50(2), 281–301. https://doi.org/10.1348/014466610X515696
- Petty, R. E., & Krosnick, J. A. (Eds.) (1995). Attitude strength: Antecedents and consequences. Psychology Press.
- Quick, B. L., LaVoie, N. R., Reynolds-Tylus, T., Martinez-Gonzalez, A., & Skurka, C. (2018). Examining mechanisms underlying fear-control in the Extended Parallel Process Model. Health Communication, 33(4), 379–391. https://doi.org/10.1080/10410236.2016.1266738
- Quick, B. L., Scott, A. M., & Ledbetter, A. M. (2011). A close examination of trait reactance and issue involvement as moderators of psychological reactance theory. Journal of Health Communication, 16(6), 660–679.
- Quick, B. L., & Stephenson, M. T. (2007). The reactance restoration scale (RRS): A measure of direct and indirect restoration. Communication Research Reports, 24(2), 131–138. https://doi.org/10.1080/08824090701304840
- R Core Team. (2021). R: A language and environment for statistical computing. R Foundation for Statistical Computing. https://www.R-project.org/.
- Radosław, T., & Dariusz, D. (2022). Data on COVID-19 vaccination intention and its predictors in Poland. Data in Brief, 42. https://doi.org/10.1016/j.dib.2022.108227
- Rains, S. A. (2013). The nature of psychological reactance revisited: A meta-analytic review. Human Communication Research, 39(1), 47–73. https://doi.org/10.1111/j.1468-2958.2012.01443.x
- Ratcliff, C. L. (2019). Characterizing reactance in communication research: A review of conceptual and operational approaches. Communication Research, 48(7), 1033–1058. https://doi.org/10.1177/0093650219872126
- Richards, A. S., Bessarabova, E., Banas, J. A., & Larsen, M. (2021). Freedom-prompting reactance mitigation strategies function differently across levels of trait reactance. Communication Quarterly, 69(3), 238–258.
- Robertson, E., Reeve, K. S., Niedzwiedz, C. L., Moore, J., Blake, M., Green, M., Katikireddi, S. V., & Benzeval, M. J. (2021). Predictors of COVID-19 vaccine hesitancy in the UK household longitudinal study. Brain, Behavior, and Immunity, 94, 41–50. https://doi.org/10.1016/j.bbi.2021.03.008
- Rosenberg, B. D., & Siegel, J. T. (2018). A 50-year review of psychological reactance theory: Do not read this article. Motivation Science, 4(4), 281–300. https://doi.org/10.1037/mot0000091
- Rosenberg, B. D., & Siegel, J. T. (2021). Threatening uncertainty and psychological reactance: Are freedom threats always noxious? Current Psychology, 1966 https://doi.org/10.1007/s12144-021-01640-8
- Sanders, J. G., Spruijt, P., van Dijk, M., Elberse, J., Lambooij, M. S., Kroese, F. M., & de Bruin, M. (2021). Understanding a national increase in COVID-19 vaccination intention, the Netherlands, November 2020–March 2021. Eurosurveillance, 26(36), 2100792. https://doi.org/10.2807/1560-7917.ES.2021.26.36.2100792
- Schäfer, T., & Schwarz, M. A. (2019). The meaningfulness of effect sizes in psychological research: Differences between sub-disciplines and the impact of potential biases. Frontiers in Psychology, 10, 1–13. https://doi.org/10.3389/fpsyg.2019.00813
- Sittenthaler, S., Traut-Mattausch, E., Steindl, C., & Jonas, E. (2015). Salzburger State Reactance Scale (SSR Scale): Validation of a scale measuring state reactance. Zeitschrift fur Psychologie/Journal of Psychology, 223(4), 257–266. https://doi.org/10.1027/2151-2604/a000227
- Shen, L., & Dillard, J. P. (2005). Psychometric properties of the Hong Psychological Reactance Scale. Journal of Personality Assessment, 85(1), 74–81. https://doi.org/10.1207/s15327752jpa8501_07
- Soveri, A., Karlsson, L. C., Mäki, O., Antfolk, J., Waris, O., Karlsson, H., Karlsson, L., Lindfelt, M., & Lewandowsky, S. (2020). Trait reactance and trust in doctors as predictors of vaccination behavior, vaccine attitudes, and use of complementary and alternative medicine in parents of young children. PLoS One, 15(7), 1–16. https://doi.org/10.1371/journal.pone.0236527
- Sprengholz, P., Betsch, C., & Böhm, R. (2021). Reactance revisited: Consequences of mandatory and scarce vaccination in the case of COVID-19. Applied Psychology: Health and Well-Being, 13(4), 986–995. https://doi.org/10.1111/aphw.12285
- Sprengholz, P., Felgendreff, L., Böhm, R., & Betsch, C. (2022). Vaccination policy reactance: Predictors, consequences, and countermeasures. Journal of Health Psychology, 27(6), 1394–1407. https://doi.org/10.1177/13591053211044535
- Story, G. W., Vlaev, I., Seymour, B., Darzi, A., & Dolan, R. J. (2014). Does temporal discounting explain unhealthy behavior? A systematic review and reinforcement learning perspective. Frontiers in Behavioral Neuroscience, 8, 1–20. https://doi.org/10.3389/fnbeh.2014.00076
- Tormala, Z. L., & Rucker, D. D. (2018). Attitude certainty: Antecedents, consequences, and new directions. Consumer Psychology Review, 1(1), 72–89. https://doi.org/10.1002/arcp.1004
- Trope, Y., & Liberman, N. (2010). Construal-level theory of psychological distance. Psychological Review, 117(2), 440–463. https://doi.org/10.1037/a0018963
- Wong, L. P., Alias, H., Wong, P. F., Lee, H. Y., & AbuBakar, S. (2020). The use of the health belief model to assess predictors of intent to receive the COVID-19 vaccine and willingness to pay. Human Vaccines and Immunotherapeutics, 16(9), 2204–2214. https://doi.org/10.1080/21645515.2020.1790279
- World Health Organisation. (2019, December). Immunization. https://www.who.int/news-room/facts-in-pictures/detail/immunization