
Abstract
Purpose
This study develops the evidence-base of interventions for inappropriate sexualised behaviour following brain injury involving adolescents.
Materials and Methods
We describe a Single-Case Multiple Baseline Design intervention of Positive Behavioural Support (PBS) across settings. It involves a 16 year old adolescent who had a severe Traumatic Brain Injury (TBI) and presented with sexualised talk and touch. PBS may potentially be a successful intervention to remediate this. The aim of the article was to determine whether PBS could reduce the frequency and impact of the sexualised behaviour in a variety of his key daily settings. Visual and quantitative analyses were completed before and after the introduction of the PBS intervention within home and school settings.
Results
Findings showed reduction in the frequency of sexualised talk and touch alongside subjective impact ratings in the home. Downward trends were encouraging in the school settings, but demonstrated smaller effects than home. The Overt Behaviour Scale showed a reduction in overall severity and the impact on others.
Conclusions
This study shows the promising impact on behaviour of introducing the PBS intervention within the home and school settings to support positive clinical change evidenced in the reduction in target behaviours and subjective response for caregivers.
IMPLICATIONS FOR REHABILITATION
Positive Behavioural Support is an effective intervention for managing inappropriate sexualised behaviour in a young person with a traumatic brain injury.
Positive Behavioural Support can improve the subjective experience of the young person and their caregivers in parallel to managing behaviour.
Single Case Experimental Design can be utilised across care and home settings for measuring change in person-centred interventions.
Introduction
Disinhibited sexualised behaviour is commonly associated with a frontal lobe brain injury due to neurological injury to circuitry that regulates urges and behaviours. Individuals can struggle to comply with social norms, lack awareness and insight into their difficulties, and lack an understanding of social and interpersonal conventions around behaviour [Citation1]. Indeed, Simpson and colleagues investigated a cohort of 507 adult Traumatic Brain Injury (TBI) patients and found 45 demonstrated inappropriate sexualised behaviour in the previous 3 months. Of those, 57.9% were sexualised talk and 29.8% were sexualised touching. They reference the brain injury as a pivotal life event that could lead such vulnerable individuals to becoming a victim and a perpetrator of a sexual assault, therefore external forms of intervention are required to reduce the adverse impact of the behaviour [Citation2,Citation3].
Neuropsychological deficits in dysexecutive disorder are known to influence certain forms of dysregulated behaviour by decreasing behavioural inhibition, impairing the ability to anticipate behavioural consequences or assess punishment and reward. This in turn can affect the ability to generate socially appropriate behaviour in challenging contexts [Citation4]. This is particularly evident in adolescents following TBI who present with marked behavioural dysregulation when compared to healthy controls and peers with brain lesions of alternative aetiology. The potential adverse impact on recovery and social re-entry is recommended to be the focus of effective and well-timed interventions to support recovery [Citation5]. Adverse Childhood Experiences, including head injury have been highlighted by Blasingame [Citation6] as potential developmental risk factors for later conduct problems and sexual offending, therefore he postulates the position of the need to provide early intervention for the child and adolescent population to prevent trajectories to later offending behaviour [Citation6].
Interventions in relation to disinhibited sexualised behaviour with individuals following a brain injury utilise specific behavioural interventions that provide clear boundaries around acceptable and unacceptable behaviour [Citation2]. A process of shaping socially appropriate behaviour through prompting the individual to cease engaging in the inappropriate behaviour and a process of fading prompts as the individual relearns boundaries around behaviour within social norms, have shown to reduce the frequency of socially inappropriate behaviours of concern [Citation2]. Behavioural analysis and Positive Behavioural Support (PBS) also provide an opportunity to reduce the setting conditions and triggers for the inappropriate behaviour, therefore making the behaviour less likely to occur [Citation7].
PBS is based on the social model of disability which pursues the notion that society, through its norms, structures and processes can disable a person with neurological deficits. Therefore, the environment and system around the individual needs to support and scaffold opportunities for the individual to participate in the normal life of the community on an equal level with others by adapting to their needs [Citation5]. It is an intervention that uses the enrichment of resources to redesign an individual’s living environment to enhance the individual’s quality of life and minimise his or her need or opportunity for inappropriate behaviour [Citation8].
A community-based intervention for treating inappropriate sexualised behaviour in adults with a brain injury was described as multi-focal, comprising of psychoeducation, environmental and behavioural change [Citation7]. This is consistent with a review of the effectiveness for treatments of children and adolescents with developmental disabilities in which behaviour, environment and education play a key role. For children and adolescents, the education needs to be adapted to their intellectual ability to aid understanding for the young person’s developing sexuality [Citation9]. An exploratory clinical trial of community based behavioural interventions for inappropriate sexualised behaviour in adults showed improvements from a multi-focal approach based on PBS for shaping pro-social behaviour long-term [Citation10]. However, the sample heterogeneity and lack of control within the study design supported the recommendation for utilising single case experimental design to respond to the unique nature of each brain injury and environment in which individuals are recovering [Citation10].
A Single Case Experimental Design (SCED) was adopted to measure a novel Cognitive Behavioural Therapy (CBT) intervention to support adults with hyposexuality to achieve improvement in sexual satisfaction. The non-concurrent baseline design demonstrated change for 9 participants (of which 4 were female) with mild to moderate TBI following an 8 week treatment phase and subsequent 8 week follow-up. This had promising results, but the mean age of the sample was over 40 years old and there was limited detail on the specific context or brain injury experienced by the participants. It also had procedural limitations as a consequence of the person-centred nature of the intervention, therefore it was not possible to define which components of the CBT intervention were utilised for each participant and what may have been effective [Citation11].
Kelly and Simpson [Citation12] recognise the complexity of interventions for sexualised behaviour and the priority to design effective interventions for the community and context in which individuals are living. They described the need for interventions to provide PBS in a manner that addresses both the environmental adaptations, but also responds to person-centred needs and supporting the network of caregivers [Citation12].
SCED’s provide an opportunity to document the complex and unique nature of behavioural formulations and person-centred positive behavioural supports when applied to brain-injury, based on a specific neuropsychological profile within a particular family and community setting [Citation13,Citation14]. It is particularly useful within neurorehabilitation when appropriate control group norms are not readily available and when the participant can serve as their own control to demonstrate meaningful change [Citation15–18]. This study is an opportunity to focus the research methodology on the adolescent age group to understand their specific developmental needs in responding to sexuality following TBI and within the context of a family and school setting. It is also an opportunity to test the impact of PBS as a preventative intervention to manage an early presentation of inappropriate sexualised behaviour in the brain injury population.
Aims
The aim is to study the effect of a PBS intervention on the severity of inappropriate sexualized behaviour in an adolescent and its impact on others. The study tests the premise that there will be change in inappropriate sexualised behaviour in response to the staggered introduction of PBS across settings.
The Primary goals for the PBS intervention were to: (a) reduce the frequency of inappropriate sexualised talk behaviour across settings; (b) reduce the impact on others of his inappropriate sexualised talk behaviour across settings; (c) reduce the frequency of inappropriate sexualised touch behaviour in the home setting; and (d) to reduce the impact of his inappropriate sexualised touch behaviour in the home setting.
Method
Design
The experimental design for the case study was a multiple baseline in which the intervention was applied with a staggered onset across three settings: home, school teaching and boarding school environments. The SCED design follows guidance of the SCRIBE group to ensure methodological quality in design and reporting [Citation16]. The dependent variables were the frequency of inappropriate sexualised talk and touch, and associated distress ratings, referred to as “impact ratings” of a second party within each setting. Sexualised touch was commonly associated with sexualised talk, but only in the home setting and was therefore included as an additional outcome measure in the home only.
Figure 1. The line graphs show a decrease in frequency of sexualised talk in the three settings after the introduction of the PBS intervention.
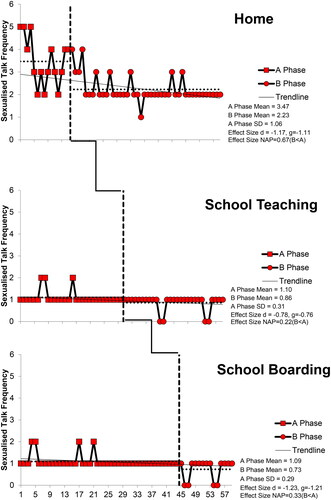
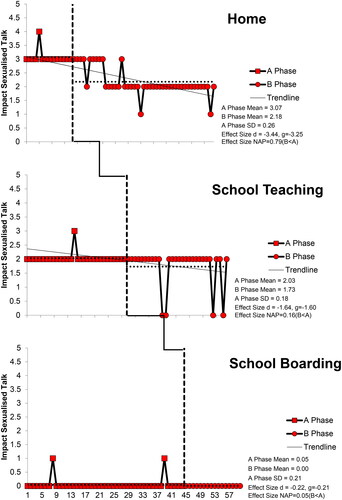
Figure 2. The line graphs show a decrease in the impact ratings in the three settings after the introduction of the PBS intervention. The impact ratings remained low in the School Boarding setting.
The target behaviours were identified using Antecedent Behaviour Consequences (ABC) charts completed by family members/school staff and operationally defined as: sexual talk: verbal comments towards females about their physical appearance; sexual touch: physical touching of females’ hair and face with hands.
The phase sequence is described in . The order was set a priori in order to stagger interventions to measure change in the dependent variables for each phase accordingly.
Table 1. The table described the procedure within each phase of the intervention for the baseline and three settings.
The onset of each phase in the multiple baseline was defined by the staggered delivery of the PBS intervention across the three settings: home, school teaching and boarding for inappropriate sexualised talk. Baseline data was collected concurrently across the settings and the PBS intervention for introduced for each setting in a staggered manner, starting with Home on Day 15, then Teaching School setting on Day 30 and finally, Boarding School setting on Day 44. The PBS intervention for sexualised touch was completed only in the home setting due to no reports of the touch behaviour in the two school settings.
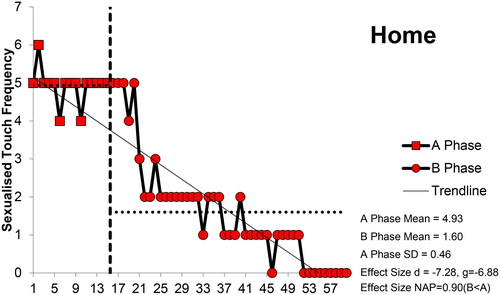
Figure 3. The line graph shows a decrease in the frequency of sexualised touch in the home setting after the introduction of the PBS intervention.
There were no changes to the above procedure that occurred during the course of the study. There was no randomization or blinding procedure because it was only possible to visit the settings on certain days and there were safeguarding implications, involving negotiation with Social Services allocated to the family when considering randomisation to intervene in the high risk sexualised behaviour, for example a potential for sexualised behaviour with a student/female sibling. Replication at the six-month stage was not possible due to constraints of independent clinical funding.
Participant
The participant was a 16-year-old Caucasian male who sustained a severe traumatic brain injury as a pedestrian following a collision with a vehicle (GCS 7 at time of injury). It was a closed head injury with diffuse axonal injury.
Four years post injury, he presented with mild intellectual disabilities, significantly impaired working memory, verbal memory, speed of processing and executive functioning. He had significant difficulties in emotional and behavioural regulation, leading to disinhibited sexualised behaviour. He also had mental health problems, namely depression and post-traumatic stress disorder. He presented with various behaviour problems, including absconding, aggression towards others and destruction of property.
Prior to the intervention, safeguarding procedures had highlighted a risk to females known to the participant, including his mother and sister. Social Services were involved with the family following the sister’s historical disclosure that the participant had sexually touched himself in her presence and sought proximity to her during the encounter.
Method of recruitment was after review of the caseload of patients and discussing their participation with the patient, family, Case Manager and Social Services.
There were no formal inclusion and exclusion criteria because of the nature of the clinical work. The family and young person consented to participate in the SCED and the school approved of participating in the SCED procedure.
Function of participant’s behaviour in PBS intervention
Sexualised talk
The functional analysis indicated that the participant engaged in sexualised talk, including comments on females’ clothing for familiar individuals and in sexual reference to body shape and an intent of sexual urge/preference, for example “You look good, I could do you”; “Your bum looks sexy in those leggings”. The establishing operations involved a dysexecutive disorder including reduced inhibitory control. This was particularly evident in free and unstructured time at home and school. The context was of a male negotiating adolescence, where sexual relations move toward increasing interest in companionship and sexual expression. The discriminative stimulus was a familiar female that he found attractive, (this included his mother and sister). The behaviour would cease when an unfamiliar or male individual passed by or if the female person did not respond but ignored and turned away. The behaviour did not occur in the presence of other unfamiliar females or males.
The function of the behaviour can be hypothesised to access/approach sexual attention; to express his sexual preference, sexual thoughts and access sexual experiences. This function is consistent with other reported cases [Citation2]. The disinhibited nature of his behaviour counters social norms and has the potential to cause offence and personal discomfort to those around him.
It is important that the behaviour was managed with an antecedent-based approach to reduce its occurrence in its current form because the nature of his frontal lobe brain injury potentially disrupted his ability to learn from consequences [Citation17]. A behaviour management plan was devised to avoid social responses to his comments and to distract him by engaging in other areas of conversation at the early signs of onset in his sexualised talk. Also, to prevent the onset of the behaviour, antecedents were managed in that he was accompanied by male 1:1 staff in his learning and leisure activities in school and stepfather at home to supervise interactions with females. It was also agreed that he would have the opportunity to explore his feelings about the opposite sex and his wishes to develop a relationship with a girl in his neuropsychology therapy and school counselling sessions. The participant contributed to developing his person-centred goal and agreed with the management plan. Therefore, the intervention was designed to manage his lack of insight into his sexually inappropriate behaviours by providing safeguards within an antecedent-based approach. It also provided an opportunity for him to explore strategies to fine-tune and develop inhibitory control when interacting and relating with the opposite sex as an initial step towards achieving his personal goal.
Sexualised touch
The functional analysis indicated that the participant engaged in touch of familiar females within the home setting, including mother and sibling. This involved touch by caressing hair and face, standing in close proximity, holding head firming in his hands, smelling and kissing their head. The establishing operation was his dysexecutive disorder and disinhibited behaviour in male adolescence. The behaviour was particularly evident in free unstructured time when he was in a marginally agitated state in seeking an activity to occupy him. The discriminative stimulus was when the familiar female appeared in the room.
The function of the behaviour can be hypothesised to allow him to access/approach physical comfort and is sensorily stimulating in nature. It is important that the behaviour is managed with an antecedent-based approach to reduce the likelihood of his engaging in it.
A behaviour management plan was devised by providing appropriate sources of physical comfort when he was seeking it i.e., hug with mother controlled in type and duration, sensory activities, in addition to a structured daily timetable that prompted him to activities throughout the day to maintain a sense of direction and purpose. If the behaviour occurred, his mother was instructed to turn away and prompt him to problem-solve to gain direction and purpose in the situation, for example check his visual daily timetable and access sensory activities to self-regulate. The participant contributed to the management plan and agreed with the intervention.
Impact of behaviour
The participant’s mother and female school staff expressed distress due to the emotional impact of the inappropriate sexualised behaviours on them. The impact as well as the frequency of sexualised talk and touch behaviours at home and sexualised talk at school were monitored across the delivery of psychoeducation and Positive Behavioural Support in order to capture change.
Context
The clinical intervention formed part of a neurorehabilitation care package to assist the individual to adjust following a severe brain injury. The privately funded neuropsychological provision worked in partnership with NHS and Social Care agencies to support the individual in living at home with family and adjusting to his new educational placement in the community.
Approvals
Ethics for the study as part of a broader programme of using SCED in a normal clinical setting with associated protocol was obtained through the University of Bath Psychology Dept Ethics 17-224.
Measures and materials
Measures
Inappropriate sexualised behaviour
The inappropriate sexualised behaviours of talk and touch were continuously monitored by the parents and sexualised talk was continuously monitored by school teaching and boarding staff by recording in an ABC diary as shown in . The descriptions of informants were used to operationalise the target behaviours of sexualised talk and sexualised touch. They were selected for intervention because both were prioritised by the family and sexualised talk alone was prioritised by school staff as “behaviours of concern.” No reports of sexualised touch were recorded in the boarding or teaching settings. Training and supervision was provided throughout the SCED to family and school staff to support consistency for identification of the target behaviours and subjective ratings of distress.
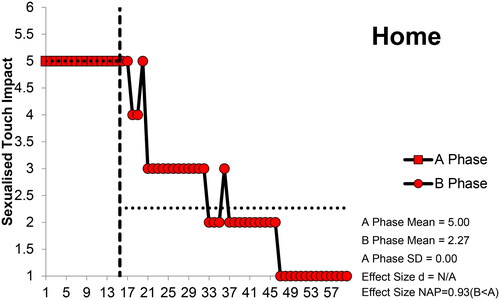
Figure 4. The line graph shows a decrease in the impact ratings within the home setting for sexualised touch after the introduction of the PBS intervention.
The frequency of behaviours and subjective impact rating by others (i.e., family or staff) of distress on exposure to the behaviours were collated daily across the three settings and throughout the baseline and intervention settings. The impact score was a Subjective Units of Distress Scale of 0–5 where 0 is no distress and 5 is extremely distressed. Family and school staff rated their distress when recording the occurrence of sexualised behaviours. These were recorded contemporaneously on a paper form using the worked example in . The daily frequency was low and the staff/family member could record each instance observed. There was an objective (frequency of behaviour observed) and a subjective (distress impact rating based on their personal experience) rating.
Table 2. The table shows an example of a behaviour observation form to record behaviour and impact ratings.
Secondary measures
Overt Behaviour Scale
A secondary outcome measure was the standardised measure of inappropriate sexualised behaviour, Overt Behaviour Scale (OBS) [Citation19], completed at pre intervention (before day 1) and post intervention (after day 58). This is a measure designed for adults with an acquired brain injury and includes items measuring sexualised behaviour including talk and touch. This was chosen because it is a highly reliable measure with interrater reliability of rs =0.99 and test-retest reliability coefficient of rs = 0.77. It has moderate to strong convergent and divergent validity coefficients ranging from rs = 0.36–0.66 with comparable measures of behaviour. There is no adolescent alternative measure, therefore a Reliable Change Index as outlined by Ogles et al. [Citation20] was calculated in relation to the participant’s own response to the intervention. This was calculated using the pre and post measure for the participant.
Goal attainment scaling
The participant’s person-centred goal attainment scaling (GAS) goal was: “To develop and maintain a relationship with a girl”. The PBS intervention was an initial step in supporting the participant to engage in socially appropriate interactions with females.
The goal attainment scaling framework by Turner-Stokes [Citation21] was used as a clinical tool to generate a person-centred goal to reflect his motivation to reduce the inappropriate sexualised behaviours to develop and maintain a positive relationship with a female peer. It was also used to review the clinical goals of reducing the frequency of inappropriate sexualised behaviour and reducing the impact (distress) on females when the behaviour occurs. The participant rated their baseline and outcome measures based on their subjective experience at the time of definition, such as “much worse than expected”, “worse than expected”, “as expected”, “better than expected” and “much better than expected”. Comparisons were made between the two timeframes of pre intervention (before day 1) and post intervention (after day 58) to measure a change on the goal for the participant.
This clinical tool was selected because it is useful to generate meaningful clinical goals for the participant and measure change over time. There is insufficient robust published evidence of its reliability because it is used at an individual or small group level and it measures multiple constructs based on the individual’s goals, i.e., is non-unidimensional, [Citation21,Citation22]. However, the person-centred nature of the measure makes it a useful clinical tool to engage and measure the meaningful subjective experience of the participant.
The participant rated the GAS goals at pre intervention (before day 1) and post intervention (after day 58) based on their subjective experience. He rated the importance of the goals and the clinician rated the difficulty at baseline on scales 1–3. The GAS comparison of pre and post intervention subjective ratings, weighted by level of difficulty and importance calculated a score of change [Citation22].
Table 3. The table shows the GAS goals utilised within the PBS intervention alongside baseline, outcome and improvement scores.
Intervention approach
The psychoeducation and PBS intervention involved partnership working with agencies, including Social Services, NSPCC to increase safeguards to prevent behaviours occurring through initial psychoeducational intervention to train family members and school staff about behavioural management and the dynamic risk assessments required for sexually inappropriate behaviour. In addition, the participant was involved in psychoeducation to help him identify and understand his behaviour. The PBS intervention was then delivered to family members and school teaching and boarding staff.
The psychoeducation aimed to increase the understanding of parents/teachers/boarding support staff about brain injury and inappropriate sexualised behaviour, increase personal safety awareness when interacting with the participant and heighten monitoring of interactions and behaviours between the participant and others.
An antecedent-based approach was used to adapt the environment to reduce the likelihood of behaviours. The behavioural assessment and functional analysis determined the contingencies of the behaviours and identified the establishing operations and discriminative stimuli. This allowed for targeted adaptations to reduce the occurrence of the behaviours by removing behavioural antecedents. Adaptations were applied across three settings: home; school teaching and school boarding.
Procedural fidelity was ensured in that the SCED procedure was monitored by the treating clinician who met with the family and school staff both face to face and remotely within treatment phases on a weekly basis to deliver training, ongoing support and guidance. This aimed to maintain the integrity of the SCED design in rolling out the PBS interventions in a staggered process across each setting. Progress through the PBS procedure was monitored within the psychoeducation and PBS intervention with regular clinical supervision of family and school staff groups in utilising behavioural guidelines within the three settings. The school staff and family were trained to recognise the target behaviours to be monitored within the intervention. This was further validated during clinical supervision of the intervention.
No adverse events were noted for the participant or environment during the SCED to impact on the fidelity of the procedure. In fact, the onset of the SCED was delayed by three months to stabilise the participant’s mental health before beginning the behavioural intervention. The participant was then emotionally stable and able to complete the intervention across all three settings.
Analysis
Data analysis
The frequency and impact scores of the behaviours were analysed using qualitative visual analysis within and at transition between phases as guided by Ledford et al. [Citation23]. “Stability Envelopes” for baselines were established utilising the definition of 80% of values falling within ± 25% of the median [Citation24]. Effect size changes were quantitatively calculated between phases using Non-overlap of all pairs NAP and 95% Confidence Interval [Citation24–27]. The confidence intervals are based on expressions for the standard error of NAP which assume that the data are not autocorrelated which is an assumption which may not be tenable [Citation28]. Therefore, cautionary interpretation of NAP analyses is required.
Visual analysis is an in-depth analysis of data across all conditions and making determinations about behavioural change based on visual data characteristics. Contingent changes in the values of dependent variables within and between conditions can be observed to potentially demonstrate the effect of an intervention [Citation23]. The least squares regression line was used to show trends in the datapoints between baseline and intervention for each setting. The analysis includes the level of a dependent variable (i.e., behaviour during the conditions), trend, variability, overlap, immediacy and what it means for the behaviour of interest.
Results
Each of the sets of data for sexualised talk contained a stable baseline (defined as 80% of values falling within ± 25% of the median) as shown in .
Sexualised talk frequency within the home setting
There was a quantitative effect (NAP= 0.67) of the intervention on sexualised talk frequency in the home setting (median 3 to 2, range 2–4). The qualitative visual analysis showed a reduction in the expected direction with negligible variability. There was limited variability in level in the baseline. There was limited overlapping on the data point of 2 after the introduction of the intervention and the frequency of behaviour reduced. Changes following the introduction of PBS at home occurred after a slight delay and in the intended downward direction.
Sexualised talk frequency in the school teaching setting
In the school teaching setting, no quantitative effect A-B (NAP= 0.22) of the intervention was found on sexualised talk (median 1, range 1–2 to median 1, range 0–1). The qualitative visual analysis showed a small reduction in the expected direction with little variability. There was limited variability in the baseline. There was limited overlapping in data point of 1 as the frequency of behaviour reduced. The change in frequency was almost immediate after the school teaching intervention. Changes were in the intended downward direction following the introduction of the PBS strategies.
Sexualised talk frequency in the boarding school setting
There was no quantitative effect A-B (NAP = 0.33) on sexual talk in the boarding school. The qualitative visual analysis showed a small reduction following a stable baseline in frequency of sexualised talk (median 1, range 1–2 to median 1, range 0–1). The reduction was in the expected direction with no unexpected variability. There was limited variability in the baseline. There was no overlapping of data points. Change was immediate after the intervention and was in the intended downward direction following the introduction of the PBS strategies.
A functional relation is present in the expected downward trend across settings in the visual analysis. There was consistency in data patterns of stable baselines and a consistent reduction in frequency post intervention across settings. There was inconsistency in quantitative effect due to very low baseline of sexualised talk frequency in the school settings, therefore a larger change was evident in the home setting. We are confident that PBS had a beneficial impact on the downward trend of sexualised talk frequency across settings.
A stable baseline in subjective impact experienced by family or staff can be seen in each of the settings as shown in .
Sexualised talk impact in home setting
There was a quantitative effect (NAP = 0.79) on subjective impact of sexual talk in home. Qualitative visual analysis showed that sexualised talk impact scores reduced A-B (median 3, range 2–4 to median 2, range 2–3) in the expected direction. There was no unexpected variability in the home setting. There was limited variability in the baseline. There was no overlapping of data points as sexualised talk impact scores reduced. Change in distress was almost immediate after the Home intervention. Change was in the intended downward direction when introducing the PBS strategies.
Sexualised talk impact in school teaching setting
No quantitative effect A-B (NAP = 0.16) is observed in the school teaching setting on this variable. Qualitative visual analysis of sexualised talk impact scores showed a small reduction A-B in trend (median 2, range 2–3 to median 2, range 0–2), in the expected direction with variability. There no overlapping data points evident. Change was not immediate in this setting, but it was in the intended downward direction. There was a slight delay in effect following the introduction of the behavioural approach.
Sexualised talk impact in boarding school setting
No quantitative effect on subjective impact is observed in the boarding school A-B (NAP = 0.05). Qualitative visual analysis showed that impact scores showed a small reduction A-B in trend in the expected direction (median 1, range 0–1 to median 0, range 0–0). There was no unexpected variability or overlapping in the setting. Change was in the intended downward direction.
A functional relation is present in the expected downward trend across settings in the visual analysis. There was consistency in the data patterns in the baselines and consistent reductions in impact ratings across settings post intervention. However, there was inconsistency in quantitative effect due to very low baseline impact ratings in the school settings, therefore a larger change was found in the home setting. We are confident that PBS improved the impact ratings across settings.
Sexualised touch frequency in home setting
As sexualised touching occurred only in the home setting, this and its subjective impact on the parent was only recorded in the home.
After a stable baseline (80% of values falling within ± 25% of the median), there was a quantitative effect (NAP = 0.90) between A-B on frequency of sexualised touch. Qualitative visual analysis of frequency showed reduction in the intended direction (median 5, range 4–6 to median 2, range 2–5). There was limited variability in the baseline and no overlap of data points to note. Change was not immediate after the introduction of the intervention but occurred several days into the implementation of the PBS strategies. A functional relation is present in the expected downward trend and we are confident that PBS had an effect on the frequency of sexualised touch within the home setting as shown in .
Sexualised touch impact in home setting
After a stable baseline (80% of values falling within ± 25% of the median), there was a quantitative effect (NAP = 0.93) in change in subjective distress A-B. Qualitative visual analysis showed sexualised touch impact scores reduction A-B (median 5, range 5–5 to median 3, range 3–5), in the intended downward direction. There was limited variability in the baseline and no overlap of data points. As with the frequency of touch, change was not immediate after the introduction of the behavioural intervention. We are confident that PBS had an effect on the sexualised touch impact scores within the home setting as shown in .
Figure 5. The column chart shows a decrease in Total Severity and Sexualised Behaviour Impact in the Overt Behaviour Scale scores when comparing pre and post intervention measures. Sexualised Behaviour Cluster remains stable due to continued sexualised talk behaviour.
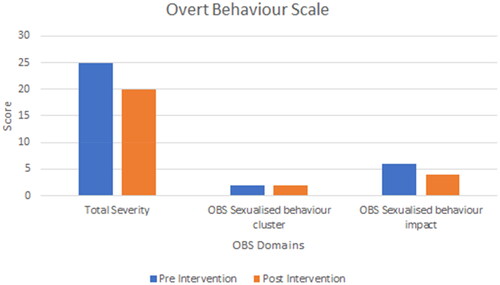
Overt Behaviour Scale
The standardised measure of inappropriate sexualised behaviour, Overt Behaviour Scale indicates that there has been a reduction in overall severity and the impact on others as shown in . However, the participant remained engaged in sexualised behaviour in the form of sexualised talk although at a reduced frequency. Reliability Change Index (RCI) for point decrease for total severity was 4.55 and 5.14 for sexualised behaviour impact. This indicates a reliable change in score for the participant [Citation20]
Goal attainment scale
Prior to the intervention, the participant reported that the situation was much worse than he expected for this stage in his life and recovery from brain injury. At the post intervention review, progress exceeded his expectations with a GAS T-score at review of 77.21, a change score of 51.01 when compared to pre-intervention [Citation21] as shown in .
Discussion
The overall aim of the study was to analyse the effect of a PBS intervention on the severity of inappropriate sexualized behaviour in an adolescent and its impact on others. The SCED methodology was a good fit to test the premise that there would be change in the frequency and impact ratings of inappropriate sexualised behaviour in response to the delivery of PBS psychoeducation and intervention in the home, school teaching and boarding school settings. The results show that the staggered introduction of the intervention led to beneficial downward trends in the frequency and impact of sexualised talk across settings. However, the magnitude of change was not consistent across settings due to very low baselines in the school settings. We have seen a large reduction in sexualised touch frequency and the impact ratings within the home setting. Given the study design we can claim with some confidence that due to the application of PBS, there were improvements in reducing the frequency and impact of inappropriate sexualised behaviour across settings. However, this was most robustly demonstrated within the home setting for which this was an area of concern and clinical priority. Therefore, the primary goals for the PBS intervention were achieved.
A good stability level for the frequency and impact ratings of the behaviours were achieved in the baseline from which to potentially demonstrate change based on the introduction of the PBS intervention in each setting. This was achieved by developing good working relationships with the school staff and family members in understanding not only the nature of the intervention that would be used, but also becoming comfortable with the structure of how this would be delivered and regular “checking in” sessions to provide reassurance and guidance about the measures being used for daily behaviour collection and impact ratings.
The PBS intervention was initially introduced within the home setting. It included training and supporting family members to use the strategies based on the assessment and functional analysis. The home setting was prioritised because the frequency of sexualised behaviours of concern were highest out of the three settings and it was causing the most distress and impact on his family members. The family had been experiencing much stress and pressure since responding to the safeguarding concerns raised by the adolescent’s sexualised behaviour. They were motivated to work towards an approach to supporting him to regulate his behaviour alongside reducing the risk posed to family members. The home setting saw a large reduction in sexualised touch frequency and impact/distress ratings. A beneficial reduction in sexualised talk was also found within the home intervention. The tangible outcome of the intervention was that the risk posed by the young person reduced to a level at which Social Services were confident to withdraw their input from the family home. The adolescent and family had more flexibility of choice in terms of access to community activities with peers and participation in age-appropriate tasks of independence. This further demonstrates the need to include the social network around the individual to support sustainable change in community interventions for sexualised behaviour [Citation12]. This is even more important for young people transitioning into adulthood and developing independence.
Following the home setting, the intervention was introduced to the teaching and classroom support staff at his school. Instances of sexualised talk were few, but caused an impact with the level of distress experienced by teaching staff. A number of female teaching staff had felt “unease” in the company of the adolescent due to the content of his comments towards them. The sexualised talk was infrequent within the School Teaching setting because the adolescent was involved in structured education activities for much of the time and there were limited opportunities for him to engage in informal conversation with familiar females. Following the PBS intervention, teaching staff gained an understanding of his behaviour within the context of his TBI and stage of development. This supported them to respond confidently to his behaviour and feel less discomfort. This setting saw a beneficial slight downward trend in sexualised talk frequency and impact ratings, but the magnitude of change was not evident or consistent with that seen in the home setting due to the low baseline.
Following the school teaching setting, the intervention was introduced to the school boarding and leisure support staff. There were very few instances of sexualised talk and low ratings of impact on school teaching and boarding staff. It must be noted that the majority of the boarding/evening leisure support staff were male and this may also account for the slight differential from teaching staff reports of sexualised behaviour. Nevertheless, the setting saw a beneficial slight downward trend in sexualised talk frequency and the impact ratings following the PBS intervention, but similarly to the other school setting, it was not evident or consistent with the magnitude of change seen in the home setting due to the low baseline. The tangible outcome from the intervention was that with negligible presentation of sexualised behaviour, the risk assessment was amended and the adolescent was able to access increasing peer interactions without direct observation by staff and further independence in leisure activities within the boarding house.
When reflecting on working with the family and the school staff teams, there was a sense of increasing understanding and compassion for the adolescent alongside confidence and competence in using the PBS strategies over time. This contributed at times to a slight delay in change seen following the introduction of the intervention. Confidence of staff is potential area for future direction of work when evaluating the impact of behavioural interventions.
There was a risk that staggered delivery over the different settings would adversely impact on the effectiveness of reducing the inappropriate sexualised behaviour. However, the staggered delivery prevented the family and school staff from being overwhelmed by strategies and allowed time for consolidation of the approaches in each setting. Clinically, it was advantageous to the treating team to stagger the introduction of the intervention in a manner which the family and school staff could tolerate, it also supported the research design by allowing the possibility to clearly measure change in his behaviour due to the timed introduction of the intervention in the three settings.
When reviewing the GAS goals to reduce the frequency of sexualised touch and talk as well as its impact on others with the participant, achievement of these exceeded his expectation, leading to “much better than expected” change. Within the GAS, the person-centred goal: “to develop and maintain a relationship with a girl”, was achieved by maintaining an age-appropriate romantic relationship with a girl for approximately 6 months. The PBS interventions at home, school teaching and boarding settings helped the participant to shape his behaviour around females to fit within social norms. His sexualised talk persisted, but was less frequent and family and school staff had strategies to manage it effectively, therefore a sense of agency provided by the intervention was seen to reduce their distress. This evidence further affirms the clinical need for early intervention for young people presenting with sexualised “behaviours of concern” in order to prevent the potential trajectory to offending and exploitation following a brain injury [Citation6].
The SCED design was useful to demonstrate the impact of a PBS intervention for a risky, “behaviour of concern” across different settings. The multiple-baseline design illustrated that the behaviour could be more problematic in one setting than another. Even a low daily frequency of sexual touch or talk was associated with high ratings of impact and distress for others. The SCED design measured an encouraging trend of the PBS intervention having an impact at each setting. SCED is useful in this situation as repeated measures of behaviour are clinically meaningful and allow a participant to act as their own control. PBS is also an intervention applicable for brain injured individuals where environmental controls can be highly effective in managing challenging behaviours.
Limitations
Randomisation is the gold standard for research when measuring the impact and effect of a clinical intervention. The safeguarding nature of this case limited the freedom of choice in applying randomisation to the design. However, options to include randomisation that would be acceptable and feasible in complex cases, such as randomising the baseline length or start points for intervention are potential areas to pursue in further studies [Citation29].
There is the potential bias of male school staff members rating the impact of sexualised talk and touching. This is because the behaviour most often occurred when the participant was in the presence of females and it caused distress to females. There is also potential that fewer instances were occurring in the presence of male 1:1 staff within the teaching and boarding school settings because the behaviour did not occur in connection with the male gender. However, this also demonstrates the effectiveness of the antecedent focused approach in managing his environment.
It would have been beneficial to add in a component to the intervention that supported the young person to explore his own cognitions and feelings around sexuality and the prospects of developing intimate relationships with a female to further consolidate behavioural change as recommended by Fraser et al. [Citation11] alongside Kelly and Simpson [Citation12].
Another limitation is that there is no follow-up at 6 months timeframe to replicate measurement for consistency of results because the independently funded clinical provision was unable to continue due to funding constraints. Clinical provision for the case was transitioned to statutory NHS services and it was not possible for the psychologist within their NHS role capacity to continue with the SCED procedure. The parents reported continuing low-level sexualised talk which would have benefited from further cognitive remediation therapy to address cognitions involved in the behaviours, for example issues of consent in relationships. This again was not possible to support as part of the SCED due to funding constraints and a cessation of independently funded clinical provision.
Applicability
The findings of the study demonstrate that PBS can be an effective intervention for managing inappropriate sexualised behaviour in an adolescent with a TBI. The SCED design can be utilised across care and home settings for an individual and tailored to their specific clinical needs. It can give strong evidence of process and outcome of goals achieved in neuropsychological rehabilitation. In litigation funded rehabilitation, where causality can be strongly contended and needs clear demonstration, it is an excellent tool. Furthermore, when there is limited evidence for the effectiveness of intervention in paediatric rehabilitation, SCED can be used to build the evidence base of “what works for whom.” It can also be of clinical value to visibly demonstrate to teachers and carers what can be achieved in behavioural interventions when maintaining their commitment and motivation to the intervention.
Conclusions
The study showed encouraging results for the beneficial impact of Positive Behavioural Support on the frequency and distress caused by inappropriate sexualised behaviour within a home, teaching and leisure environments for an adolescent following a TBI. The SCED methodology allowed causal relationships in complex clinical neuropsychological cases to be confirmed with a level of confidence. A multiple baseline design across settings systematically demonstrated impact and quantified the effect of the PBS intervention. The intervention developed and consolidated competency of family and school staff in using the treatment approach to assist the adolescent to change and shape his behaviour to better fit social norms.
Further considerations for research
The SCED was useful in measuring change across settings to demonstrate outcome for a clinical intervention. It would be beneficial to further develop processes of measurement to ease the application in normal clinical practice, for example involving digital daily measurements that reduce burden on caregivers. It would also be useful to further research the process of behavioural skill acquisition for PBS within and across clinical settings to further understand the stages of educational instruction to consolidation and autonomy. It is important to broaden and replicate the evidence-base of psychological interventions used within clinical neuropsychology and neurorehabilitation using single-case experimental design to document the heterogeneity in clinical presentation within the adolescent population and across contexts within the field of brain injury.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Anderson MI, Parmenter TR, Mok M. The relationship between neurobehavioural problems of severe traumatic brain injury (TBI), family functioning and the psychological well-being of the spouse/caregiver: path model analysis. Brain Inj. 2002;16(9):743–757. doi:10.1080/02699050210128906.
- Kelly G, Simpson G. Remediating serious inappropriate sexual behaviour in a male with severe acquired brain injury. Sex Disabil. 2011;29(4):313–327. doi:10.1007/s11195-011-9213-9.
- Simpson G, Sabaz M, Daher M. Prevalence, clinical features, and correlates of inappropriate sexual behavior after traumatic brain injury: a multicenter study. J Head Trauma Rehabil. 2013;28(3):202–210. doi:10.1097/HTR.0b013e31828dc5ae.
- Ogilvie JM, Stewart AL, Chan RCK, et al. Neuropsychological measures of executive function and antisocial behaviour: a meta-analysis. Crim. 2011;49(4):1063–1107. doi:10.1111/j.1745-9125.2011.00252.x.
- Pastore V, Galbiati S, Recla M, et al. Psychological and behavioural difficulties following severe TBI in adolescence: a comparison with a sample of peers with brain lesions of other origin and with a control group. Brain Inj. 2018;32(8):1011–1020. doi:10.1080/02699052.2018.1469041.
- Blasingame G. Traumatic brain injury and sexually offensive behaviors. J Child Sex Abus. 2018;27(8):972–977. doi:10.1080/10538712.2018.1510454.
- Ylvisaker M, Turkstra LS, Coelho C. Behavioural and social interventions for individuals with traumatic brain injury: a summary of the research and clinical implications. Semin Speech Lang. 2005;26(4):256–267. doi:10.1055/s-2005-922104.
- Barnes C. Disabled people in Britain and discrimination: a case for anti-discrimination legislation. London (UK): Hurst and Co; 1991.
- Gore NJ, McGill P, Toogood S. Definition and scope of positive behavioural support. BILD Int J Posit Behav Supp. 2013;3(2):14–23.
- Kelly G, Brown S, Gillett L, et al. Can behaviour support interventions successfully treat inappropriate sexual behaviour after acquired brain injury in community settings? A case series (N = 24). Neuropsychol Rehabil. 2022;32(3):407–428. doi:10.1080/09602011.2020.1830807.
- Fraser E, Downing M, Haines K, et al. Evaluating a novel treatment adapting a cognitive behaviour therapy approach for sexuality problems after traumatic brain injury: a single case design with nonconcurrent multiple baselines. J Clin Med. 2022;11(12):3525. doi:10.3390/jcm11123525.
- Kelly G, Simpson G. The behaviour support elements checklist: profiling intervention elements in community-based behaviour support for sexualised behavior after acquired brain injury. Brain Inj. 2023;37(6):551–561. doi:10.1080/02699052.2023.2184494.
- McLay L, Carnett A, Tyler-Merrick G, et al. A systematic review of interventions for inappropriate sexual behaviour of children and adolescents with developmental disabilities. Rev J Autism Dev Disord. 2015;2(4):357–373. doi:10.1007/s40489-015-0058-5.
- Arco L, Bishop J. Single participant studies in positive behaviour support for parents of individuals with brain injuries. Brain Impair. 2009;10(3):307–319. doi:10.1375/brim.10.3.307.
- Brown F, Anderson JL, Pry Rl D. Individual positive behaviour supports: a standards-based guide to practices in schools and community settings. Baltimore (MD): Paul H. Brookes Publishing Co Inc; 2015.
- Tate RL, Perdices M, Rosenkoetter U, et al. The single-case reporting guideline in behavioural interventions (SCRIBE) 2016: explanation and elaboration. Arch Sci Psychol. 2016;4(1):10–31. doi:10.1037/arc0000027.
- Krasny-Pacini A, Evans J. Single-case experimental designs to assess intervention effectiveness in rehabilitation: a practical guide. Ann Phys Rehabil Med. 2018;61(3):164–179. doi:10.1016/j.rehab.2017.12.002.
- Ponsford J. Sexual changes associated with traumatic brain injury. NeuroRehabilitation. 2013;13:273–289.
- Kelly G, Todd J, Simpson G, et al. The overt behaviour scale (OBS): a tool for measuring challenging behaviours following ABI in community settings. Brain Inj. 2006;20(3):307–319. doi:10.1080/02699050500488074.
- Ogles BM, Lambert M, Masters KS. Assessing outcome in clinical practice. Allyn and Bacon; 1996.
- Turner-Stokes L. Goal attainment scaling (GAS) in rehabilitation: a practical guide. Clin Rehabil. 2009;23(4):362–370. doi:10.1177/0269215508101742.
- Tennant A. Goal attainment scaling: current methodological challenges. Disabil Rehabil. 2007;29(20–21):1583–1588. doi:10.1080/09638280701618828.
- Ledford J, Lane J, Severini K. Systematic use of visual analysis for assessing outcomes in single case design studies. Brain Impair. 2017;19(1):4–17. doi:10.1017/BrImp.2017.16.
- Manolov J, Solanas A. Analytical options for single case experimental designs: review and application to brain impairment. Brain Impair. 2017;19(1):18–32. doi:10.1017/BrImp.2017.17.
- Lane J, Gast D. Visual analysis in single case experimental design studies: brief review and guidelines. Neuropsychol Rehabil. 2014;24(3–4):445–463. doi:10.1080/09602011.2013.815636.
- Perdices M. Null hypothesis significance testing, p-values, effect sizes, and confidence intervals. Brain Impair. 2017;19(1):70–80. doi:10.1017/BrImp.2017.28.
- Morley S, Edited Masterson C, Main CJ. Single-case methods in clinical psychology: a practical guide. Oxford: Routledge; 2018.
- Shadish WR, Sullivan KJ. Characteristics of single-case designs used to assess intervention effects in 2008. Behav Res Methods. 2011;43(4):971–980. doi:10.3758/s13428-011-0111-y.
- Levin J, Ferron J, Gafurov B. Comparison of randomization-test procedures for single-case multiple-baseline designs. Dev Neurorehabil. 2018;21(5):290–311. doi:10.1080/17518423.2016.1197708.