
ABSTRACT
Reminiscence-based interventions focus on recalling autobiographical memories and reflective reasoning to develop a healthy and adaptive view of oneself and one’s life. This study aimed to replicate the effects of a three-session, group-based, positive-memory version of cognitive-reminiscence therapy (CRT) on psychological resources and mental well-being and extend the findings to anticipated pleasure. The participants (N = 75, Mage = 43.7 (SD = 16.7), 60% females) were randomised to CRT or control group. Anticipated pleasure, psychological resources (schemas of positive self-esteem, self-efficacy, meaning in life, optimism), mental well-being (depression, anxiety, and stress symptoms) and theorised change processes (automatic negative thoughts, awareness of narrative identity) were assessed. Relative to the control group, the CRT group reported significantly higher anticipated pleasure (d = 0.76–0.93) and psychological resources of self-esteem, self-efficacy, and optimism (d’s = 0.58–0.99) at post-CRT and follow-up, and lower depressive symptoms post-CRT and at follow-up (d = 0.56–0.67). Findings on meaning in life and negative automatic thinking were partially replicated. This study replicates findings of the effectiveness of this intervention for improving psychological resources such as self-worth, confidence and optimism and depressive symptoms, and indicates additional effects on anticipated pleasure. CRT may serve as a standalone intervention, or as an adjunct “memory booster” for interventions focused on future thinking and related anticipated reward.
Reminiscence-based interventions focus on the remembering and reviewing of autobiographical memories to improve mental health and well-being. In reminiscence-based interventions, specific events, life periods, and one’s life in general are reflected on and interpreted in ways that foster healthy and adaptive beliefs and attitudes (Webster et al., Citation2010; Westerhof et al., Citation2010). Reminiscence-based interventions have been shown to be effective in alleviating depressive symptoms and improving psychological resources, including meaning in life, self-efficacy, positive well-being, and cognitive functioning (Pinquart & Forstmeier, Citation2012) both in community populations and in clinical populations with depression (Westerhof & Slatman, Citation2019), dementia (Park et al., Citation2019), and chronic physical disease (Pinquart & Forstmeier, Citation2012).
One particular form of reminiscence-based therapy known as cognitive-reminiscence therapy (CRT; Watt & Cappeliez, Citation2000) incorporates cognitive therapy (Beck et al., Citation1997) and stress and coping models and techniques (Billings & Moos, Citation1981) to produce healthy and positive beliefs about oneself and one’s experiences and develop more adaptive interpretations of life events (Watt & Cappeliez, Citation1995, Citation2000). Theoretically, the aim is to recall and/or interpret past experiences in a way that is consistent with strengthening adaptive schemas about the self, others, and the world. These include being self-efficacious, having a sense of personal worth and being valued by others, having a sense of meaning and purpose in life, and to healthily integrate experiences of disappointment and loss in narratives about one’s life and self. These beliefs are reinforced with examples across the lifetime, a process aimed to improve the causal and thematic coherence of one’s experiences. Consistent with this theory, basic research has shown that a higher frequency of adaptive reminiscence improves mental well-being through increases in self-efficacy, self-esteem, meaning in life, and optimism (Hallford & Mellor, Citation2016ba). Experimentally, CRT has been shown to decrease depressive symptoms in several studies amongst older adults (Cappeliez, Citation2002; Karimi et al., Citation2010; Watt & Cappeliez, Citation2000). CRT has also been proposed as relevant for young adults (Hallford & Mellor, Citation2013), and has been shown to significantly improve psychological resources and reduce depressive symptoms in a six-session format in a help-seeking sample of young adults with clinical depression symptoms (Hallford & Mellor, Citation2016b) and in a three-session format focusing on positive memories in a community sample of young adults (Hallford, Hardgrove et al., Citation2022).
A yet unanswered question is whether reminiscence-based interventions also improve the anticipation of pleasure. Several studies have shown that remembering specific details of recent memory leads to increases in detail and imagery when attention is then turned to imagining future events (Madore & Schacter, Citation2016; Schacter & Madore, Citation2016). This finding is also observed when the recalled past experiences are personally relevant and not limited to recent experiences (Hallford, Farrell, et al., Citation2020). That is, more richly detailed future thinking is associated with significantly stronger anticipated pleasure and increased positive affect related to future events, an emotional response that can be both rewarding and motivating. Imagining past events in specific and detailed ways may “prime” an individual to then imagine potential future self-relevant events in similarly specific ways, which, in turn, evokes a stronger emotional response. It could also be that increasing access to positive past experiences or making them more salient, leads to an update of predictive models about future experiences so that they are perceived as more likely to involve pleasure and reward. This seems to be borne out by findings of increased optimism as a result of cognitive-reminiscence intervention in clinical and non-clinical samples (see above).
Should this be demonstrated, then a reminiscence-based intervention approach might then have particular relevance in the context of disorders characterised by negatively biased predictions of future events, such as major depression (Hallford, Barry, et al., Citation2020; Hallford & Sharma, Citation2019; Kube et al., Citation2020). A recent trend in research has been to focus on improving the up-regulation of positive affect for those with emotional disturbances such as elevated depression or anxiety symptoms (Craske et al., Citation2019, Citation2023). The guided recall of past, rewarding experiences may be a method of disrupting pathological deficits in the expectation of reward, such as that typically associated with anhedonia. Indeed, during CRT, participants are taught to savour the positive emotions and experiences of past events, potentially altering their expectations that future events will also be pleasurable and rewarding. This may improve a person’s ability to focus on specific information that will increase reward value when imagining future events (Kube et al., Citation2019). Although CRT has been shown to be effective in reducing depressive symptoms, specific effects on the anticipation of pleasure have not yet been assessed.
The aim of the current study was to replicate the effects of CRT on psychological resources and mental well-being in a community sample (Hallford, Hardgrove et al., Citation2022), and assess whether there are also effects on anticipated pleasure. Given the acknowledged importance of replication of findings in psychology (Nosek et al., Citation2022), a key aim was simply to repeat this experiment to establish if similar outcomes were found and therefore whether they are reliable. A further consideration is that the study being replicated was completed in the context of the COVID-19 pandemic in Australia and stay-at-home restrictions. This may have affected the results, for example, by participants being more sensitive to the effects of an intervention for mental well-being during a time of poorer mental health (Butterworth et al., Citation2022). The current study, which was completed following the lifting of these restrictions, can therefore test if these effects also occurduring a time of relative “normalcy”. Once again, the sessions were conducted using videoconference, a format which has high accessibility. Notably, the participants were not recruited based on poor mental well-being, that is, they were not assessed as experiencing clinically significant levels of mental illness or issues. The primary aim of this particular study was to assess changes in psychological resources, not treat mental health issues. However, as previous studies have shown improvements in indices of psychological distress within non-indicated community samples, such as the one in the current study, we opted to assess it. The study also aimed to replicate the effects on some putative change processes. Negative automatic thoughts were assessed, given that reviewing positive past experiences should activate schemas about the self, the world, and the future, and integrate positive information into these schemas. Awareness of narrative identity was also assessed, given the aim of CRT was to meaningfully connect and integrate past experiences into an overarching sense of continuity and meaning, giving rise to the perception of “life stories”.
It was hypothesised that the CRT group would report higher self-esteem, self-efficacy, meaning in life, and optimism than the control group immediately after the CRT sessions and at follow-up. It was also hypothesised that the CRT group would report a significantly lower frequency of negative automatic thoughts and a higher awareness of life stories. Lastly, it was hypothesised that the CRT group would report lower depressive, anxiety and stress symptoms than the control group immediately after and at follow-up of CRT, and higher anticipated pleasure.
Methods
Design
A randomised controlled trial design was used, with two arms (CRT; no CRT control) and three time-points (baseline; immediately post-CRT; two-week follow-up). The primary outcomes were anticipated pleasure and psychological resources of self-schemas of self-esteem, self-efficacy, meaning in life, and optimism. The secondary outcomes were negative automatic thoughts, awareness of narrative identity, and mental well-being assessed with symptoms of depression, anxiety, and stress symptoms. The study design was pre-registered online at https://aspredicted.org/am2gj.pdf. Data are available on request due to privacy/ethical restrictions.
Participants
A community sample was recruited between June and August 2022 using advertisements on social media and snowball sampling. The inclusion criteria were fluency in English, currently living in Australia, and having internet access in the home. G*Power V3.1.9.4 (Faul et al., Citation2007) was used to calculate an a priori power analysis based on a previous study of this same protocol, which showed moderate to large effects on the variables of interest (Hallford, Hardgrove et al., Citation2022). It was unclear what magnitude of the effect would be found on anticipated pleasure, so a more conservative small to moderate effect size was estimated. In pre-registration the sample size was calculated in error, using an independent samples t-test rather than the ANCOVA at each time-point controlling for baseline (one covariate) as set out in the pre-registration. In the erroneous t-test estimate, we planned for 100 participants, allowing us power (1 − β = .80, α = .05) to detect a group difference of d = 0.35. This was considered feasible with the resources available for the project, however, as noted below, we were unable to collect this sample due to dropout and lack of additional time in which researchers were available to collect more data. The post-hoc power analysis for the correct planned ANCOVA indicated that the final sample of 75 participants would allow us to detect a moderate to large effect size (f = 0.327, 1 − β = .80, α = .05).
A total of 108 adults registered interest in the study and 89 completed the baseline measures and were randomised to a condition. Of these, 11 dropped out of the CRT condition and 3 of the control condition leaving a total of 75 participants (34 CRT; 41 control) who completed the study and were included in the final analysis (see ). These numbers were too small to conduct meaningful inferential tests of differences between completers and non-completers within groups. Although the reason for this uneven dropout is unclear, it may pertain to issues of burden or availability in having to attend three, weekly sessions in addition to completing surveys, relative to only completing surveys in the control group. As indicated in , the average age was mid-40s, with just over half being women, most had university-level education and were in paid employment and almost all identified as Caucasian. There were no differences found between groups on age or gender. Education and ethnicity were not analysed with inferential tests given the inadequate cell sizes, but inspection of the descriptive statistics did not indicate any notable differences.
Figure 1. Participant flowchart.
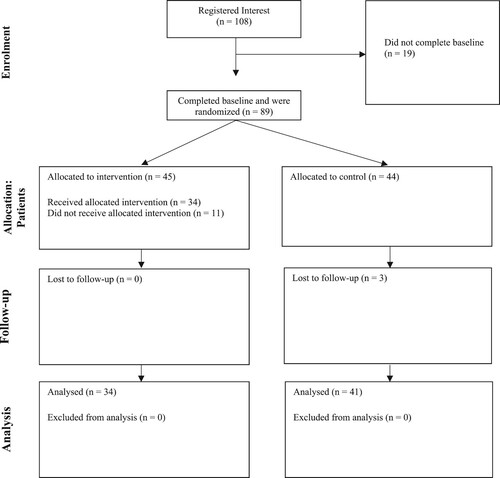
Table 1. Characteristics of participants.
Materials
Self-esteem
A five-item, positively worded version of the Rosenberg Self-Esteem Scale was used (Rosenberg, Citation2015). This shorter form retains the properties of the full scale, with good convergent and divergent validity, and internal reliability (Hallford et al., Citation2013; Hallford & Mellor, Citation2016a). For each item participants responded using an 11-point, end-defined self-report scale ranging from 0 (do not agree at all) to 10 (agree completely). The responses were averaged, with higher scores indicating higher self-esteem. In this current study, internal reliability was good (MacDonald’s ω = .89).
Self-efficacy
The New General Self-Efficacy Scale (NGSE; Chen et al., Citation2001) was used to assess the perception of personal competence in coping effectively with a variety of stressful situations. Participants responded to eight items using a self-report scale ranging from 1 (strongly disagree) to 5 (strongly agree). The responses were averaged together, with higher scores indicating higher general self-efficacy. The NGSE has good psychometric properties (Chen et al., Citation2001; Scherbaum et al., Citation2006). In this current study, internal reliability was good (MacDonald’s ω = .86).
Meaning in life
The Presence subscale of the Meaning in Life Questionnaire (Steger et al., Citation2006) was used to assess how meaningful participants felt their lives to be. This five-item scale has good psychometric properties (Steger et al., Citation2006). Participants rated their responses on a scale ranging from 1 (absolutely untrue) to 7 (absolutely true). The response scores were averaged, with higher scores indicating a stronger sense of meaning in life. In this current study, internal reliability was good (MacDonald’s ω = .87).
Optimism
A three-item, short-form of The Life Orientation Test–Revised (LOT-R; Carver et al., Citation2010) measured optimism. This included only the positively worded items from the LOT. This short version has demonstrated good convergent and divergent validity, and good internal reliability (Hallford et al., Citation2013; Hallford & Mellor, Citation2016a). Participants responded using a self-report scale from 1 (I disagree a lot) to 5 (I agree a lot). The responses were averaged, with higher scores indicative of positive generalised outcome expectancies for the future. In the current study, internal reliability was acceptable (MacDonald’s ω = .77).
Negative automatic thoughts
The Automatic Thoughts Questionnaire (ATQ; Netemeyer et al., Citation2002) was used to assess the frequency of negative thoughts about oneself and one’s life over the last week using eight items, for example, “I’m no good” or “I’m so disappointed in myself”. Participants responded using a self-report scale from 1 (not at all) to 5 (all the time), and the responses were averaged with higher scores indicating more frequent negative automatic thoughts. This eight-item version of the ATQ has good psychometric properties consistent with the longer versions (Netemeyer et al., Citation2002). In the current study, internal reliability was good (MacDonald’s ω = .86).
Awareness of narrative identity
The five-item awareness subscale of the Awareness of Narrative Identity Questionnaire (Hallford & Mellor, Citation2017) was used to assess how strongly people perceived that there were stories about their life that could be derived from their past experiences (e.g., “when I think over my lifetime, I can observe how there is a story that tells me who I am”). This subscale has good psychometric properties and construct validity by correlating with various indices of the coherence of written narratives about people’s lives (Hallford & Mellor, Citation2017). Participants responded to the items with an 11-point, end-defined self-report scale from 0 (do not agree at all) to 10 (agree completely). In the current study, internal reliability was good (MacDonald’s ω = .92).
Depression, anxiety, and stress symptoms
The 21-item version of the Depression, Anxiety, and Stress Scale (DASS-21; Lovibond & Lovibond, Citation1995) assessed mental well-being via core symptoms of depression, anxiety, and stress. The subscales have seven self-report items each of which are rated on a four-point self-report scale from 0 (did not apply to me at all) to 3 (applied to me very much, or most of the time). The subscales possess good psychometric properties (Antony et al., Citation1998). In the current study, subscale internal reliabilities were acceptable to good (MacDonald’s ω: depression = .83, anxiety = .67, stress = .88).
Anticipated pleasure
The 14-item Snaith–Hamilton Pleasure Scale (SHAPS; Snaith et al., Citation1995) was used to assess the expectancy of pleasure from future events. The scale’s items consist of statements regarding the anticipation of pleasure at undertaking a given activity; for example, “I would enjoy being with family or close friends”, “I would enjoy a warm bath or refreshing shower”, “I would be able to enjoy a beautiful landscape or view”. Responses to the items are given on a four-point Likert scale, ranging from 1 (strongly disagree) to 4 (strongly agree). The scores were averaged to create an overall score from zero to four, with higher scores indicating greater anticipated pleasure, and lower scores indicating a lack of anticipated pleasure associated with anhedonia. The SHAPS has been demonstrated to have good reliability and validity in both clinical and non-clinical samples (Franken et al., Citation2007; Langvik & Borgen Austad, Citation2019). In this current study, the internal consistency was good (MacDonald’s ω = .87).
Cognitive-reminiscence therapy protocol
The same three-session version of CRT was used as in Hallford, Hardgrove et al. (Citation2022), which was adapted from a six-session, individual-format version for clinical depression. Both are manualised for standardised delivery and available through open access along with other CRT materials such as guides for implementation: https://osf.io/su2b4/. The CRT protocol is described in detail in the aforementioned places, however, in summary, participants engage in three, weekly 60–90-min sessions to discuss positive past experiences, using a different topic each week: positive relationships, coping and overcoming, and meaning in life. These topics are intended as springboards to elicit memories and enhance psychological resources through guided interviews. The facilitators provide some psychoeducation, then facilitate the recall and framing (or reframing) of memories to develop or enhance healthy beliefs towards oneself and one’s abilities, personal growth, and significance of experiences in the context of one’s life. Specific questions are asked with the aim of encouraging reflective reasoning to increase the perception of psychological resources. For example, participants are guided to describe how experiences made them feel about themselves, aspects of successful coping and adaptation and their associated outcomes, personally meaningful aspects of their experiences, and what they have learned. Each participant shared one or two memories per session and were individually guided by a facilitator/s to reflect on the experience. This was followed by group reflection on each memory and the process overall. Homework sheets were used to prompt memories and review memories for the following session.
Procedures
The study received ethical approval from the University Human Ethics Advisory Group (HEAG-H 82_2020). Participants registered through online advertisements on social media and after providing informed consent were randomised into a condition using a computer-based algorithm (www.randomizer.org) with a 1:1 ratio. Participants in the CRT condition were emailed homework sheets to complete prior to each session. Approximately one week after completing the baseline survey (estimated around 30 min to complete), CRT participants started group sessions delivered over three weeks using a teleconference platform. The groups ranged in size from 2 to 5. Several participants who were unable to attend their group session engaged in briefer one-to-one sessions following the same protocol. The sessions were facilitated by four students with completed undergraduate degrees in Psychology and who were completing their honours/graduate year thesis. The first author, a registered clinical psychologist, provided training and supervision in CRT. The participants were emailed links to complete surveys at each time-point. Those in the wait-list condition were offered the chance to participate in the CRT programme once data collection was finalised. No other incentives were offered to participate.
Data analysis plan
IBM SPSS Statistics Version 28 was used for statistical analyses. Descriptive statistics for variables at each time-point were generated, and Pearson correlations were used to examine the zero-order association of variables at baseline. MacDonald’s ω was used to assess the internal reliability of the measurement scale items. This has superior properties and performance than Cronbach’s alpha, such as not (erroneously) assuming that each item has equivalent precision in measuring the latent variable (see Hayes & Coutts, Citation2020). Consistent with the pre-registration, analysis of covariance (ANCOVA) tests were used to obtain a estimation of the intervention effect which was defined by differences between the groups at post-session and follow-up while adjusting for the baseline score (Frison & Pocock, Citation1992; Twisk & Proper, Citation2004; van Breukelen, Citation2013; Vickers & Altman, Citation2001). Estimation of the intervention effect through the means and standard errors adjusted for baseline scores reflected the group-by-time interaction. To control for Type 1 errors, with α set at .05, the ANCOVA analyses were subject to the false discovery rate procedure (Benjamini, Citation2010). This procedure provides good statistical power in correcting for Type 1 errors as it controls only the proportion of significant results that are Type I errors. This is in contrast to other approaches, such as the Bonferroni correction, that control the general familywise error rate to avoid a single Type I error. This more severe penalty would risk causing a Type II error in the context of this study which has a small sample and involves a number of tests. A corrected significance level is provided (q). For standardised mean difference scores, Cohen’s d was interpreted as follows: small = .2, medium = .5, large = .8 (Cohen, Citation1992). The SPSS script for analyses can be found in the Supplementary Materials.
Results
shows the baseline correlations of the study variables, and shows the descriptive statistics and results of the inferential tests. The study variables generally had significant correlations with each other, and the effect sizes ranged in magnitude. A series of independent samples t-tests indicated the groups did not differ significantly at baseline on the study variables (all t’s < 1.63, all p’s > .054). The exception was anticipated pleasure, on which the control group participants reported lower scores at baseline, albeit with uncorrected p-values, t(75) = 2.1, p = .033, d = .50. The ANCOVA analysis allowed for control of these differences in analyses of between-group effects.
Table 2. Correlations between study variables at baseline.
Table 3. Comparison of outcomes between control and CRT groups across time.
The ANCOVA analyses (see ), adjusting for baseline scores, indicated that the CRT group was significantly higher on psychological resources, with the exception of meaning in life, at post-intervention and follow-up relative to the control group. The effects, where significant, were generally moderate in size. There were group differences for negative automatic thoughts immediately post-CRT, but not follow-up, whereas there was a moderately sized significant effect for awareness of narrative identity at post-CRT and follow-up time-points. Depressive symptoms were significantly lower in the CRT group at post-CRT and follow-up, with moderate effect sizes, but there was no significant difference between the groups on anxiety or stress symptoms at either time-point. Lastly, anticipatory pleasure was significantly higher in the CRT group immediately post-CRT and at follow-up, with moderate to large effects.
Discussion
This study aimed to replicate previous outcomes (Hallford, Hardgrove, et al., Citation2022) of a brief intervention using the guided review of positive memories to improve psychological resources (i.e., positive self-schemas) and mental well-being, and some putative change processes, and to see if these findings extended to changes in anticipated pleasure. Across the psychological resources variables, the hypotheses were generally supported, with moderate to large effects at post-CRT and the two-week follow-up. Contrary to expectations, there were no significant differences between the groups on meaning in life, although there was a trend towards a small to moderate-sized effect at post-intervention. As predicted, there were less frequent negative automatic thoughts and a stronger awareness of narrative identity in the CRT group, but the group effects for negative automatic thoughts were not apparent at follow-up. For indices of psychological distress, there were clear, significant group differences for depressive symptoms at post-CRT and follow-up, but no differences for anxiety or stress symptoms. Supporting predictions on anticipated pleasure, engaging in CRT was associated with significantly higher anticipated pleasure for future events relative to the control group.
To the authors’ knowledge, this study is the first to show that a reminiscence-based intervention can increase anticipated pleasure. The finding is consistent with previous experimental findings in controlled laboratory studies (Hallford, Farrell, & Lynch, Citation2020), which also showed that remembering positive past events leads to increased positive emotional responses to self-relevant future events. However, this is the first to show effects that are maintained over time after a structured intervention, and on a measure that is commonly used to assess the clinical presence or absence of anhedonia (Trøstheim et al., Citation2020).
Increasingly, interventions that directly focus on thinking about possible self-relevant future events to increase anticipated and anticipatory pleasure are appearing in the literature. They have been shown to have effects on anticipatory and anticipated pleasure in community samples (Hallford, Yeow, et al., Citation2020), and to treat anhedonia, reduce other clinical symptoms, and improve functioning in people experiencing a major depressive episode (Hallford, Rusanov et al., Citation2023). Less commonly, reported studies incorporate elements of guided memory recall into these interventions (for an exception, see Pile, Smith, Leamy, Oliver, Bennett, et al., Citation2021; Pile, Smith, Leamy, Oliver, Blackwell, et al., Citation2021), and the unique effect of a memory component is not clear. The current findings suggest that the guided review of previous positive experiences, focusing on the psychological resources described previously, has an effect in improving anticipated pleasure without any concerted focus on future events. Further, this “memory booster” for anticipating pleasure from future events may have potential as a component for interventions that target future thinking. It is possible that it provides incremental increases in anticipated and anticipatory pleasure by helping to update prediction models of reward. Indeed, the effects of CRT on optimism and sell-efficacy support this notion, indicating that this “memory booster” enhances schemas to increase positive expectancies of the future as well as the sense of perceived control over future events. However, these specific pathways of action require further testing. Another mechanism for improving anticipated pleasure could relate to improvements in future thinking overall through priming or practice in specific episodic thinking (Madore & Schacter, Citation2016; Schacter & Madore, Citation2016). This might be studied further by examining phenomenological characteristics or processes in past and future thinking that might change in CRT, such as use of specificity, detail and imagery in simulating episodic thoughts, the use of spatial details (Hallford, Cheung, et al., Citation2023), repeated simulations (Szpunar & Schacter, Citation2013), and the temporal distance of past and future imagined events (Hallford, Carmichael, et al., Citation2022).
The findings for self-esteem, self-efficacy and optimism are consistent with previous studies of CRT. This is further evidence that group-based, guided review of memories in CRT improves people’s self-concept, whereby they report feeling more worthwhile, more competent and able to deal with challenges and have more positive expectancies for their future. The lack of effect for meaning in life is inconsistent with these previous studies. however, the group differences observed were not trivial, and it may be that effects on meaning in life are only small-to-moderate; a magnitude that is common in reminiscence-based interventions (Pinquart & Forstmeier, Citation2012).
The findings for the psychological distress indices were mixed, with a moderate effect on depression symptom scores in the CRT group at post and follow-up, but no group differences for anxiety and stress. This is inconsistent with the previous study, in which changes in all three indices were found (Hallford, Hardgrove, et al., Citation2022). The relatively lower baseline scores on anxiety and stress measures in the current community sample (Crawford et al., Citation2011) will likely have reduced the potential for change. Again, this could possibly be accounted for by the no longer being in a pandemic lockdown context. That said, significant group differences were found for depressive symptoms, which is consistent, not only with previous effects but also the therapeutic model and aim of the intervention which is explicitly directed towards reducing depressive symptoms (Watt & Cappeliez, Citation2000). It is important to note, however, that when considering the absolute change in scores over time, the effects are numerically very small, and the clinical significance of such changes in depressive symptoms in the sample overall is unlikely to be very meaningful.
The findings for negative automatic thoughts were mixed, with a clear effect observed immediately after CRT, but no difference between the groups at follow-up due to an unexpected decrease in scores in the control group. This is in contrast to the original study, wherein the group difference was preserved at follow-up. It is unclear why this change in the control group occurred. Similar to some other measures, there were overall lower scores at baseline relative to the study being replicated, and so there is a possible floor effect for further reductions that were only previously observed at follow-up in the CRT group. Future replications should again test for effects on this variable to assess their reliability. In the case of awareness of narrative identity, the findings were replicated. Through CRT, people co-create understandings of the experiences in their lives, and the aim is to develop a stronger sense of their experiences as being meaningfully integrated and reflective of their identity (Watt & Cappeliez, Citation2000). A stronger awareness of narrative identity at baseline was correlated with stronger psychological resources, consistent with previous research (Hallford, Ricarte, et al., Citation2021; Hallford & Mellor, Citation2017; Sevim & Otrar, Citation2021). A novel finding was that awareness of narrative identity was positively correlated with anticipated pleasure. Having a clearer sense of positive, healthy stories about one’s life may facilitate the extension of these stories into the future so as to anticipate pleasure from future events. Potentially, self-defining events from the past that are salient may help with imagining similarly themed self-defining events in the future (D’Argembeau et al., Citation2012). Changes in the self-defining nature of past and future self-defining memories, and their valence and inter-correlations, could be empirically examined in future studies.
There were several limitations to the current study which are consistent with the study being replicated. Not having an active control group makes it challenging to untangle specific CRT processes from other, common processes in empathic and supportive group settings. The task of doing self-guided reminiscence activities may be adequate for at least some change to occur, although potentially not the magnitude of those observed here. We are currently completing another trial with an active control group with unguided reminiscence activities which may clarify this. Other active control groups such as neutral memory recall, or even mere attentional control tasks, might also help to account for non-specific processes implicated in CRT. On a related note, more measures are needed to better understand specific cognitive change mechanisms. It could be inferred that it was some component of the guided memory activities that produced the group differences (given this was done in one group and not in the control). However, whether participants experience changes in the way they use episodic thinking (e.g., increased detail, imagery, emotional intensity) and whether any changes are maintained after CRT, and predict changes in outcome variables, is currently unknown. A longer follow-up is needed to assess the maintenance of changes, which will also be implemented in a forthcoming trial, although previous research suggests the effects would be maintained (Hallford & Mellor, Citation2016b; Pinquart & Forstmeier, Citation2012). The study relied solely on self-report which gives rise to the possibility of demand characteristics and other such biases. The use of objectively coded narratives to assess change in understanding of memory and self-concept, as suggested above, may help mitigate this somewhat. Another point is the uncertainty about the generalisation of these results given the sample was relatively well-educated and predominantly Caucasian/White European ethnicity. Lastly, many statistical tests (i.e., 20 across post and follow-up group comparisons) were run for the primary analyses. Large numbers of tests increase the likelihood of Type I, false positive, findings. In the current study, this was somewhat mitigated against by controlling the false discovery rate using the false discovery procedure. However, we cannot rule out that some findings below the selected .05 alpha, particularly those with a corrected p-value approaching .05, were false discoveries.
In terms of the strengths of the study, this replication has bolstered confidence in the finding that, compared to a no-intervention control, CRT can lead to increased anticipated pleasure, higher psychological resources, and lower depressive symptoms. This replication was conducted with a different set of facilitators, again with no formal post-graduate training in psychological therapy. This provides evidence for generalisability and suggests that the intervention does not require specialised skill sets to implement, nor does it require a highly specific explanatory model for clients or skills-training. Given that this intervention has now been shown to have effects in two community samples and a help-seeking sample, it may be worthwhile to examine its effects in a wider range of clinical groups that may benefit from the increased psychological resources and improvements in depressive symptoms. Another possibility is to assess its use in relapse prevention in depression, given that these psychological resources may be prophylactic for the onset of clinically significant depressive symptoms (Holden, Citation1992; Mascaro & Rosen, Citation2008; Paradise & Kernis, Citation2002; Scheier & Carver, Citation1985; Sowislo & Orth, Citation2013; Steca et al., Citation2014).
In conclusion, this brief, positive-focused, teleconference-delivered version of cognitive-reminiscence therapy was effective in increasing anticipated pleasure and psychological resources and reducing depressive symptoms in adults. This largely replicates previous findings and increases confidence in the effects of this intervention. This is encouraging for further research to examine its effects and change processes in more detail, and to understand for which individuals, and which presented issues, it might be most useful for.
Supplemental Material
Download MS Word (288.2 KB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Antony, M. M., Cox, B. J., Enns, M. W., Bieling, P. J., & Swinson, R. P. (1998). Psychometric properties of the 42-item and 21-item versions of the depression anxiety stress scales in clinical groups and a community sample. Psychological Assessment, 10(2), 176–181. https://doi.org/10.1037/1040-3590.10.2.176
- Beck, A. T., Rush, A. J., Shaw, B. F., & Emery, G. (1997). Cognitive theory of depression. Guilford Press.
- Benjamini, Y. (2010). Discovering the false discovery rate. Journal of the Royal Statistical Society Series B: Statistical Methodology, 72(4), 405–416. https://doi.org/10.1111/j.1467-9868.2010.00746.x
- Billings, A. G., & Moos, R. H. (1981). The role of coping responses and social resources in attenuating the stress of life events. Journal of behavioral medicine, 4(2), 139–157. https://doi.org/10.1007/BF00844267
- Butterworth, P., Schurer, S., Trinh, T. A., Vera-Toscano, E., & Wooden, M. (2022). Effect of lockdown on mental health in Australia: Evidence from a natural experiment analysing a longitudinal probability sample survey. The Lancet Public Health, 7(5), e427–e436. https://doi.org/10.1016/S2468-2667(22)00082-2
- Cappeliez, P. (2002). Cognitive-reminiscence therapy for depressed older adults in day hospital and long-term care. In J. D. Webster & B. K. Haight (Eds.), Critical advances in reminiscence work: From theory to application (pp. 300–313). Springer Publishing Company.
- Carver, C. S., Scheier, M. F., & Segerstrom, S. C. (2010). Optimism. Clinical Psychology Review, 30(7), 879–889. https://doi.org/10.1016/j.cpr.2010.01.006
- Chen, G., Gully, S. M., & Eden, D. (2001). Validation of a new general self-efficacy scale. Organizational Research Methods, 4(1), 62–83. https://doi.org/10.1177/109442810141004
- Cohen, J. (1992). A power primer. Psychological Bulletin, 112(1), 155–159. https://doi.org/10.1037/0033-2909.112.1.155
- Craske, M. G., Meuret, A. E., Echiverri-Cohen, A., Rosenfield, D., & Ritz, T. (2023). Positive affect treatment targets reward sensitivity: A randomized controlled trial. Journal of Consulting and Clinical Psychology, 350–366. https://doi.org/10.1037/ccp0000805
- Craske, M. G., Treanor, M., Dour, H., Meuret, A., & Ritz, T. (2019). Positive affect treatment for depression and anxiety: A randomized clinical trial for a core feature of anhedonia. Journal of Consulting and Clinical Psychology, 87(5), 457–471. https://doi.org/10.1037/ccp0000396
- Crawford, J., Cayley, C., Lovibond, P. F., Wilson, P. H., & Hartley, C. (2011). Percentile norms and accompanying interval estimates from an Australian general adult population sample for self-report mood scales (BAI, BDI, CRSD, CES-D, DASS, DASS-21, STAI-X, STAI-Y, SRDS, and SRAS). Australian Psychologist, 46(1), 3–14. https://doi.org/10.1111/j.1742-9544.2010.00003.x
- D’Argembeau, A., Lardi, C., & van der Linden, M. (2012). Self-defining future projections: Exploring the identity function of thinking about the future. Memory (Hove, England), 20(2), 110–120. https://doi.org/10.1080/09658211.2011.647697
- Faul, F., Erdfelder, E., Lang, A.-G., & Buchner, A. (2007). G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods, 28, 1–11. https://doi.org/10.3758/BF03193146
- Franken, I. H. A., Rassin, E., & Muris, P. (2007). The assessment of anhedonia in clinical and non-clinical populations: Further validation of the Snaith-Hamilton pleasure scale (SHAPS). Journal of Affective Disorders, 99(1–3), 83–89. https://doi.org/10.1016/j.jad.2006.08.020
- Frison, L., & Pocock, S. J. (1992). Repeated measures in clinical trials: Analysis using mean summary statistics and its implications for design. Statistics in Medicine, 11(13), 1685–1704. https://doi.org/10.1002/sim.4780111304
- Hallford, D., & Mellor, D. (2013). Reminiscence-based therapies for depression: Should they be used only with older adults? Clinical Psychology: Science and Practice, 20(4), 452–468. https://doi.org/10.1111/cpsp.12043
- Hallford, D. J., Barry, T. J., Austin, D. W., Raes, F., Takano, K., & Klein, B. (2020). Impairments in episodic future thinking for positive events and anticipatory pleasure in major depression. Journal of Affective Disorders, 260, 536–543. https://doi.org/10.1016/j.jad.2019.09.039
- Hallford, D. J., Carmichael, A. M., Austin, D. W., Dax, S., Coulston, M. I., & Wong, A. (2022). Brief inductions in episodic past or future thinking: Effects on episodic detail and problem-solving. Cognitive Processing, 23(1), 15–25. https://doi.org/10.1007/s10339-021-01067-w
- Hallford, D. J., Cheung, S., Baothman, G., & Weel, J. (2023). Selective effects of focusing on spatial details in episodic future thinking for self-relevant positive events. Psychological Research, 87(2), 613–623. https://doi.org/10.1007/s00426-022-01668-w
- Hallford, D. J., Farrell, H., & Lynch, E. (2020). Increasing anticipated and anticipatory pleasure through episodic thinking. Emotion, 22(4), 690–700. https://doi.org/10.1037/emo0000765
- Hallford, D. J., Hardgrove, S., Sanam, M., Oliveira, S., Pilon, M., & Duran, T. (2022). Remembering for resilience: Brief cognitive-reminiscence therapy improves psychological resources and mental well-being in young adults. Applied Psychology: Health and Well-Being, 14(3), 1004–1021. https://doi.org/10.1111/aphw.12364
- Hallford, D. J., & Mellor, D. (2016a). Autobiographical memory and depression: Identity-continuity and problem-solving functions indirectly predict symptoms over time through psychological well-being. Applied Cognitive Psychology, 30(2), 152–159. https://doi.org/10.1002/acp.3169
- Hallford, D. J., & Mellor, D. (2016b). Autobiographical memory-based intervention for depressive symptoms in young adults: A randomized controlled trial of cognitive-reminiscence therapy. Psychotherapy and Psychosomatics, 85(4), 152–159. https://doi.org/10.1159/000444417
- Hallford, D. J., & Mellor, D. (2017). Development and validation of the awareness of narrative identity questionnaire (ANIQ). Assessment, 24(3), 399–413. https://doi.org/10.1177/1073191115607046
- Hallford, D. J., Mellor, D., & Cummins, R. A. (2013). Adaptive autobiographical memory in younger and older adults: The indirect association of integrative and instrumental reminiscence with depressive symptoms. Memory (Hove, England), 21(4), 444–457. https://doi.org/10.1080/09658211.2012.736523
- Hallford, D. J., Ricarte, J. J., & Hermans, D. (2021). Perceived autobiographical coherence predicts depressive symptoms over time through positive self-concept. Frontiers in Psychology, 12, 625429. https://doi.org/10.3389/fpsyg.2021.625429
- Hallford, D. J., Rusanov, D., Yeow, J. J. E., Austin, D. W., D’Argembeau, A., Fuller-Tyszkiewicz, M., & Raes, F. (2023). Reducing anhedonia in major depressive disorder with future event specificity training (FEST): A randomized controlled trial. Cognitive Therapy and Research, 47(1), 20–37. https://doi.org/10.1007/s10608-022-10330-z
- Hallford, D. J., & Sharma, M. K. (2019). Anticipatory pleasure for future experiences in schizophrenia spectrum disorders and major depression: A systematic review and meta-analysis. British Journal of Clinical Psychology, 58(4), 357–383. https://doi.org/10.1111/bjc.12218
- Hallford, D. J., Yeow, J. J. E., Fountas, G., Herrick, C. A., Raes, F., & D’Argembeau, A. (2020). Changing the future: An initial test of future specificity training (FeST). Behaviour Research and Therapy, 131, 103638. https://doi.org/10.1016/j.brat.2020.103638
- Hayes, A. F., & Coutts, J. J. (2020). Use omega rather than Cronbach’s alpha for estimating reliability. But … . Communication Methods and Measures, 14(1), 1–24. https://doi.org/10.1080/19312458.2020.1718629
- Holden, G. (1992). The relationship of self-efficacy appraisals to subsequent health related outcomes. Social Work in Health Care, 16(1), 53–93. https://doi.org/10.1300/j010v16n01_05
- Karimi, H., Dolatshahee, B., Momeni, K., Khodabakhshi, A., Rezaei, M., & Kamrani, A. A. (2010). Effectiveness of integrative and instrumental reminiscence therapies on depression symptoms reduction in institutionalized older adults: An empirical study. Aging & Mental Health, 14(7), 881–887. https://doi.org/10.1080/13607861003801037
- Kube, T., Glombiewski, J. A., Gall, J., Touissant, L., Gärtner, T., & Rief, W. (2019). How to modify persisting negative expectations in major depression? An experimental study comparing three strategies to inhibit cognitive immunization against novel positive experiences. Journal of Affective Disorders, 250, 231–240. https://doi.org/10.1016/j.jad.2019.03.027
- Kube, T., Schwarting, R., Rozenkrantz, L., Glombiewski, J. A., & Rief, W. (2020). Distorted cognitive processes in major depression: A predictive processing perspective. Biological Psychiatry, 87(5), 388–398. https://doi.org/10.1016/j.biopsych.2019.07.017
- Langvik, E., & Borgen Austad, S. (2019). Psychometric properties of the Snaith–Hamilton pleasure scale and a facet-level analysis of the relationship between anhedonia and extraversion in a nonclinical sample. Psychological Reports, 122(1), 360–375. https://doi.org/10.1177/0033294118756336
- Lovibond, P. F., & Lovibond, S. H. (1995). The structure of negative emotional states: Comparison of the depression anxiety stress scales (DASS) with the beck depression and anxiety inventories. Behaviour Research and Therapy, 33(3), 335–343. https://doi.org/10.1016/0005-7967(94)00075-U
- Madore, K. P., & Schacter, D. L. (2016). Remembering the past and imagining the future: Selective effects of an episodic specificity induction on detail generation. Quarterly Journal of Experimental Psychology, 69(2), 285–298. https://doi.org/10.1080/17470218.2014.999097
- Mascaro, N., & Rosen, D. H. (2008). Assessment of existential meaning and its longitudinal relations with depressive symptoms. Journal of Social and Clinical Psychology, 27(6), 576–599. https://doi.org/10.1521/jscp.2008.27.6.576
- Netemeyer, R. G., Williamson, D. A., Burton, S., Biswas, D., Jindal, S., Landreth, S., Mills, G., & Primeaux, S. (2002). Psychometric properties of shortened versions of the automatic thoughts questionnaire. Educational and Psychological Measurement, 62(1), 111–129. https://doi.org/10.1177/0013164402062001008
- Nosek, B. A., Hardwicke, T. E., Moshontz, H., Allard, A., Corker, K. S., Dreber, A., Fidler, F., Hilgard, J., Kline Struhl, M., Nuijten, M. B., Rohrer, J. M., Romero, F., Scheel, A. M., Scherer, L. D., Schönbrodt, F. D., & Vazire, S. (2022). Replicability, robustness, and reproducibility in psychological science. Annual Review of Psychology, 73(1), 719–748. https://doi.org/10.1146/annurev-psych-020821-114157
- Paradise, A. W., & Kernis, M. H. (2002). Self-esteem and psychological well-being: Implications of fragile self-esteem. Journal of Social and Clinical Psychology, 21(4), 345–361. https://doi.org/10.1521/jscp.21.4.345.22598
- Park, K., Lee, S., Yang, J., Song, T., & Hong, G. R. S. (2019). A systematic review and meta-analysis on the effect of reminiscence therapy for people with dementia. International Psychogeriatrics, 31(11), 1581–1597. https://doi.org/10.1017/S1041610218002168
- Pile, V., Smith, P., Leamy, M., Oliver, A., Bennett, E., Blackwell, S. E., Meiser-Stedman, R., Stringer, D., Dunn, B. D., Holmes, E. A., & Lau, J. Y. F. (2021). A feasibility randomised controlled trial of a brief early intervention for adolescent depression that targets emotional mental images and memory specificity (IMAGINE). Behaviour Research and Therapy, 143, 103876. https://doi.org/10.1016/j.brat.2021.103876
- Pile, V., Smith, P., Leamy, M., Oliver, A., Blackwell, S. E., Meiser-Stedman, R., Dunn, B. D., Holmes, E. A., & Lau, J. Y. F. (2021). Harnessing mental imagery and enhancing memory specificity: Developing a brief early intervention for depressive symptoms in adolescence. Cognitive Therapy and Research, 45(5), 885–901. https://doi.org/10.1007/s10608-020-10130-3
- Pinquart, M., & Forstmeier, S. (2012). Effects of reminiscence interventions on psychosocial outcomes: A meta-analysis. Aging & Mental Health, 16(5), 541–558. https://doi.org/10.1080/13607863.2011.651434
- Rosenberg, M. (2015). Society and the adolescent self-image. In Society and the Adolescent Self-Image. Princeton University Press. https://doi.org/10.1177/003803856900300250
- Schacter, D. L., & Madore, K. P. (2016). Remembering the past and imagining the future: Identifying and enhancing the contribution of episodic memory. Memory Studies, 9(3), 245–255. https://doi.org/10.1177/1750698016645230
- Scheier, M. F., & Carver, C. S. (1985). Optimism, coping, and health: Assessment and implications of generalized outcome expectancies. Health Psychology : Official Journal of the Division of Health Psychology, American Psychological Association, 4(3), 219–247. https://doi.org/10.1037/0278-6133.4.3.219
- Scherbaum, C. A., Cohen-Charash, Y., & Kern, M. J. (2006). Measuring general self-efficacy: A comparison of three measures using item response theory. Educational and Psychological Measurement, 66(6), 1047–1063. https://doi.org/10.1177/0013164406288171
- Sevim, E., & Otrar, M. (2021). The validity and reliability of Turkish version of awareness of narrative identity questionnaire (ANIQ). Kastamonu Eğitim Dergisi, 29(3), 769–777. https://doi.org/10.24106/kefdergi.882170
- Snaith, R. P., Hamilton, M., Morley, S., Humayan, A., Hargreaves, D., & Trigwell, P. (1995). A scale for the assessment of hedonic tone the Snaith-Hamilton Pleasure Scale. The British Journal of Psychiatry, 167(1), 99–103. https://doi.org/10.1192/bjp.167.1.99
- Sowislo, J. F., & Orth, U. (2013). Does low self-esteem predict depression and anxiety? A meta-analysis of longitudinal studies. Psychological Bulletin, 139(1), 213–240. https://doi.org/10.1037/a0028931
- Steca, P., Abela, J. R. Z., Monzani, D., Greco, A., Hazel, N. A., & Hankin, B. L. (2014). Cognitive vulnerability to depressive symptoms in children: The protective role of self-efficacy beliefs in a multi-wave longitudinal study. Journal of Abnormal Child Psychology, 42(1), 137–148. https://doi.org/10.1007/s10802-013-9765-5
- Steger, M. F., Frazier, P., Kaler, M., & Oishi, S. (2006). The meaning in life questionnaire: Assessing the presence of and search for meaning in life. Journal of Counseling Psychology, 53(1), 80–93. https://doi.org/10.1037/0022-0167.53.1.80
- Szpunar, K. K., & Schacter, D. L. (2013). Get real: Effects of repeated simulation and emotion on the perceived plausibility of future experiences. Journal of Experimental Psychology: General, 142(2), 323–327. https://doi.org/10.1037/a0028877
- Trøstheim, M., Eikemo, M., Meir, R., Hansen, I., Paul, E., Kroll, S. L., Garland, E. L., & Leknes, S. (2020). Assessment of anhedonia in adults with and without mental illness: A systematic review and meta-analysis. JAMA Network Open, 3(8), e2013233–e2013233. https://doi.org/10.1001/jamanetworkopen.2020.13233
- Twisk, J., & Proper, K. (2004). Evaluation of the results of a randomized controlled trial: How to define changes between baseline and follow-up. Journal of Clinical Epidemiology, 57(3), 223–228. https://doi.org/10.1016/j.jclinepi.2003.07.009
- van Breukelen, G. J. P. (2013). ANCOVA versus CHANGE from baseline in nonrandomized studies: The difference. Multivariate Behavioral Research, 48(6), 895–922. https://doi.org/10.1080/00273171.2013.831743
- Vickers, A. J., & Altman, D. G. (2001). Analysing controlled trials with baseline and follow up measurements. British Medical Journal, 323(7321), 1123–1124. https://doi.org/10.1136/bmj.323.7321.1123
- Watt, L M, & Cappeliez, P. (1995). Reminiscence interventions for the treatment of depression in older adults. In B. K. Haight & J. D. Webster (Eds.), The art and science of reminiscing: Theory, methods, and applications (pp. 221–232). Washington, DC: Taylor and Francais.
- Watt, L. M., & Cappeliez, P. (2000). Integrative and instrumental reminiscence therapies for depression in older adults: Intervention strategies and treatment effectiveness. Aging & Mental Health, 4(2), 166–177. https://doi.org/10.1080/13607860050008691
- Webster, J. D., Bohlmeijer, E. T., & Westerhof, G. J. (2010). Mapping the future of reminiscence: A conceptual guide for research and practice. Research on Aging, 32(4), 527–564. https://doi.org/10.1177/0164027510364122
- Westerhof, G. J., Bohlmeijer, E., & Webster, J. D. (2010). Reminiscence and mental health: A review of recent progress in theory, research and interventions. Ageing and Society, 30(4), 697–721. https://doi.org/10.1017/S0144686X09990328
- Westerhof, G. J., & Slatman, S. (2019). In search of the best evidence for life review therapy to reduce depressive symptoms in older adults: A meta-analysis of randomized controlled trials. Clinical Psychology: Science and Practice, 26(4), e12301. https://doi.org/10.1111/cpsp.12301