
Abstract
This review evaluates the strength of evidence for school-based mental health and suicide prevention programs that meet the legal eligibility criteria of the Suicide Training and Awareness Nationally Delivered for Universal Prevention Act of 2021 (STANDUP Act). Included studies were aggregated by program and a program’s overall body of evidence was evaluated using the LEGEND system. Requirements for implementation were also documented. We identified 29 studies, which, when aggregated, encompassed 12 unique programs that meet the statute’s evidence-based criteria. All four outcomes described in the statute were measured, with help-seeking being the most commonly measured. Two programs were assigned a high level of evidence in decreasing suicidal thoughts and behaviors. The findings serve as a resource for school officials in identifying evidence-based mental health and suicide prevention programs and understanding the resources needed for implementation.
INTRODUCTION
Adolescent suicide and related mental and behavioral health disorders are growing concerns in the United States (U.S.) and across the world. Suicide is the second leading cause of death for youth aged 10-18 in the U.S. (Centers for Disease Control and Prevention [CDC], Citation2022) and the second leading cause of death worldwide in 15-29 year olds (World Health Organization, Citation2018). In 2021, 22% of adolescents in the U.S. reported seriously considering suicide in the last 12 months and 10% reported attempting suicide, a 25% increase from reported attempts in 2011 (CDC, Citation2021).
The U.S. Surgeon General recently issued a health advisory that American youth were experiencing a national mental health crisis exacerbated by the COVID-19 pandemic (Health & Human Services Press Office, 2021). That same year, adolescent girls aged 12-17 visited an emergency department for a suspected suicide attempt at a rate 1.5 times higher than before the pandemic (Jones et al., Citation2022; Yard et al., Citation2021). Between 2019 and 2020, suicide deaths increased by 13% for males aged 10-14 and by 4% for females aged 15-24 (Curtin, Hedegaard, & Ahmad, Citation2021). Current school-based mental health and suicide prevention legislation can be leveraged to address the national mental health crisis in youth.
Existing Evidence for School-Based Suicide Prevention
Schools provide an opportune setting for universal suicide prevention efforts targeting adolescents as youth spend most of their day in the school environment, and schools allow for a structured context to deliver such content (Brann, Baker, Mills, Watt, & Diorio, Citation2021). Brann et al. (Citation2021) performed a meta-analysis on school-based suicide prevention programs, noting an improvement in suicide knowledge and awareness, a decrease in suicidal thoughts and behaviors (STBs), and an increase in help-seeking skills after implementation of such programs, with the strongest effects in increasing suicide awareness and knowledge. Specifically looking at STBs, another review found school-based suicide prevention programs to decrease STBs three months after implementation, with slightly larger effects on reducing suicidal behaviors than reducing suicidal thoughts (Gijzen, Rasing, Creemers, Engels, & Smit, Citation2022).
School-based mental health and suicide prevention programs vary widely in their scope, content, costs, target audience, duration, and method of delivery. A recent systematic review on suicide prevention strategies from Mann, Michel, and Auerbach (Citation2021) found that universal school-based suicide prevention programs directed at students reduced suicide attempts, whereas programs directed at only training adults in schools showed weaker and inconsistent benefits. Walsh, McMahon, and Herring (Citation2022) found that students who received such programming had 13-15% and 28-34% lower odds of suicidal ideation and suicide attempts, respectively. Number needed to treat analyses estimate that one less adolescent would have a suicide attempt for every 20-25 adolescents engaging in school-based suicide prevention programs.
To our knowledge, no review papers of universal school-based suicide prevention programs have limited their analyses to programs with implementation materials readily available for schools to easily access and use. Furthermore, when evaluating such programs, it is important to grade the entire body of evidence for each program, rather than just focusing on one or two seminal studies, in order to support program selection decisions by on-the-ground school officials and community stakeholders.
Current Policies and Legislation
According to the American Foundation for Suicide Prevention (AFSP) (Citation2022), 25 states in the U.S. require policies and programs on suicide prevention in schools, and 20 states specifically require the programs to include student education on suicide and/or mental health awareness. In response to the growing evidence on the benefits of student-directed training and awareness programs, multiple U.S. states have passed or introduced legislation in the last three years requiring mental health education and/or suicide prevention training in schools (Hopeful Futures Campaign, Citation2022).
On the federal level, the Suicide Training and Awareness Nationally Delivered for Universal Prevention (STANDUP) Act was unanimously passed by the U.S. Congress in March 2022 (STANDUP Act, 2022). It provides federal funding for such programs and “encourages states and tribes to implement and expand evidence-based suicide prevention training in schools” directly to students in 6th-12 grade (Sandy Hook Promise, n.d.). The Bipartisan Safer Communities Act (2022) allocated additional funds to Project AWARE for school-based mental health programs. This recent legislation demonstrates that government officials see mental health and suicide prevention in schools as priorities for our youth. The impact of the STANDUP Act rests on high quality implementation, which underscores the value of guidance designed for schools regarding evidence-based programs that meet the eligibility criteria for funding under the STANDUP Act.
Excellent resources have been developed such as the American Academy of Pediatrics (AAP) “Blueprint for Suicide Prevention,” which provides information on suicide prevention efforts in healthcare settings, the community, and schools (AAP, Citation2022), but does not provide evidence grading of programs. For state, local, and tribal agencies to leverage the funding allocated by state and federal legislation, there is a need for evidence grading along with implementation details for each program.
The Current Study
Our study has three objectives: (1) identify student-directed school-based mental health and suicide prevention programs with available implementation materials that meet the legal criteria of the STANDUP Act, (2) aggregate published studies by program and grade the body of evidence for each program, stratified by outcome, and (3) provide implementation guidance for schools when delivering such programs. Through these objectives, this paper provides a resource for schools in the U.S. to implement effective suicide prevention programming for youth.
METHODS
A rapid evidence synthesis of the existing literature, including of recent systematic reviews and meta-analyses, was conducted to verify what programs meet the legal criteria of the STANDUP Act. In line with rapid review methodology (Garritty et al., Citation2021; Tricco et al., Citation2015), the search process included only published literature and articles written in the English language. The references of 11 recent systematic reviews and meta-analyses on this topic were searched in parallel with a broad database search to help verify and update the existing published reviews. Thus, the chance of missing a relevant study is low. Our evidence synthesis aims to leverage and build upon other systematic reviews in a timely and concise manner so that the results are more actionable by state, local, and tribal educational agencies.
Search Strategy
A literature search was conducted in PsycInfo, ERIC, CINAHL, and PubMed on July 28, 2022, that included the following search terms: (Suicid*)[all fields] AND (“School*”[tiab] or “School Health Services”[MeSH] or “School Mental health Services”[MeSH] or “Schools”[MeSH] OR “school-based”[tiab] or “school health service”[tiab] or “school mental health”[tiab]). The search’s date range was from January 1, 1970 to July 28, 2022. The search was filtered by age of the study participants (Child [6-12 years old] and Adolescent [13-18 years old]). Additional studies were identified through searching references of systematic reviews, meta-analyses, and school-based suicide prevention book chapters (Supplemental Table 1). Brann et al. (Citation2021) had similar inclusion criteria and outcomes as the STANDUP Act. That search strategy was duplicated on August 3, 2022, and updated from the date of its search (excluding the term “college”). Those results were then added to the search results for this review. The searching strategy was in line with Cochrane Rapid Review methods recommendations (Garritty et al., Citation2021).
Study Selection
Inclusion and exclusion criteria for study selection were mapped to the legal definitions utilized in the STANDUP Act. Accordingly, study participants included students in grades 6 through 12. Studies needed to evaluate program interventions that deliver universal suicide awareness and/or prevention training directly to students in the school setting. The STANDUP Act specifically focuses on universal prevention programs. We followed the Institute of Medicine (IOM) definition for universal interventions as “targeted to the general public or a whole population group” (IOM, 1994, p. 24). In this study, the population group is an entire school or grade. Included studies were available in the English language. To support implementation of our findings, included studies evaluated programs with readily available training and implementation materials in the English language so that they would be useable by U.S. schools. Study authors and program coordinators were directly contacted by the study team regarding the availability of implementation materials.
Studies were excluded if they did not meet the definition of “evidence-based” as written in section 8101 of the Elementary and Secondary Education Act of 1965 (2022), which is referenced within the STANDUP Act as a requirement for program funding (). As the third evidence-based option listed in the statute was ambiguous (i.e., an intervention that demonstrated statistically significant effects based on a “well-designed correlational study with controls for selection bias”), studies with a control group—along with bias assessment as part of the evaluation criteria—were used as a surrogate for “correlational (studies) with controls for selection bias.” This limited our search to studies with a control group. However, if a program was found to have at least one study with a control group, additional non-controlled studies evaluating that program were included to provide a more holistic assessment of the full evidence base for the program.
FIGURE 1. Definition of Evidence-Based per the Elementary and Secondary Education Act of 1965.

Articles were identified through searching the references of 11 recent systematic reviews, two book chapters on school-based suicide prevention, and the broad database search described above. New articles identified by the database search were screened for inclusion by one reviewer (LK) and uncertainty about inclusion was resolved by two further reviewers (MK, HW).
Outcomes
Outcome measures were derived from the language and goals of the STANDUP Act. These included (1) STBs (i.e., suicidal ideation, plan, and/or attempts), (2) help-seeking behaviors or help-seeking intentions for self or others, (3) suicide knowledge and awareness (including mental health risk factors), and (4) awareness of resources for mental health and suicide prevention. These constructs are typically measured prior to the program and at various time points after program implementation with a variety of surveys and validated measures.
Data Analysis and Grading of Evidence
Following the screening of titles and abstracts and full text reviews, included studies were independently evaluated by two methodologists (LK, DSL) using evidence appraisal forms from the LEGEND (Let Evidence Guide Every New Decision) evidence evaluation system (Clark, Burkett, & Stanko-Lopp, Citation2009). For each study, based on study design and study domain (i.e., intervention), evidence appraisal forms were completed to assess risk of bias, internal validity, reliability, and applicability. Appraisal forms also included evaluations of clinical significance based on the findings’ descriptions, effect sizes, and external validity of each study for each outcome. Based on the study design and overall quality of the study, each article was assigned a quality level per the LEGEND system (). Some studies received multiple quality levels if they measured more than one of the stated outcomes. Quality levels could vary between outcomes within a single study if one outcome had stronger effect sizes than another or was measured through a different study method.
TABLE 1. Quality levels and body of evidence recommendations based on the LEGEND system.
Following the determination of quality levels for each study by outcome, the individual studies were then aggregated by program. The two methodologists independently assigned an overall evidence grade for each program and outcome using the LEGEND Evidence Grading tool (). This tool includes guidance on aggregating individual studies into a Grade for the Body of Evidence, informing the overall evidence quality for recommendations that each program achieved the targeted outcomes (Clark et al., Citation2009). The two reviewers then convened to compare results and any differences in grading were resolved by consensus after reviewing the evidence appraisal forms. In the absence of statistical significance for an outcome, the two reviewers judged an outcome’s public health significance based on the study authors’ conclusions and the clinical significance factors described above (i.e., effect size, precision, external validity). All included studies had at least one outcome with a reported statistical or clinical benefit. In addition to the evidence grade assigned to each program by outcome, other dimensions for judging the strength of the recommendations were explicitly discussed by the two reviewers and the authors (e.g. feasibility, scalability, and cost-effectiveness).
RESULTS
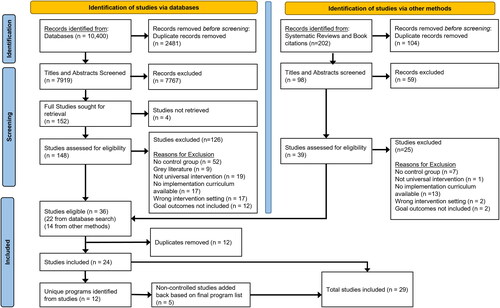
The reference search resulted in 202 articles with an additional 10,400 articles identified through the database search (). A total of 24 studies were included after removing duplicates and applying exclusion criteria, which resulted in 12 unique mental health and suicide prevention programs. All 12 programs had at least one study with a control group to meet the inclusion threshold. To evaluate the totality of evidence for these 12 included programs, five additional studies evaluating those programs that did not utilize a control group were added into the sample for a total of 29 studies ().
FIGURE 2. Flow diagram for searches of databases, books, and other sources.
Study Features
As seen in , studies varied in location and sample population demographics. More studies were conducted in urban or suburban populations (55%) than in rural populations (28%); 24% of studies included both an urban and rural group. 62% were conducted in the U.S., improving their generalizability for the STANDUP Act. Studies primarily focused on high school students; 90% of studies included students in 9th grade or older and only 17% included students younger than 9th grade. Every program except one had at least one study conducted with high school students, while only a third of programs had studies that included middle school students. One study did not specify the age of the participants.
TABLE 2. Study features listed by program.
At the program level, 50% of the programs had at least one study with an identified urban or suburban population and 42% had at least one study with a rural population. Not all studies identified their locations as rural, urban, or suburban. Three programs had both rural and urban populations studied. 75% of the programs had at least one study conducted in the U.S. Among the other 25% of programs without a published study completed in the U.S., one program (Teen Mental Health First Aid) studied in Australia also has a U.S.-based study under review.
Amongst the studies that collected race and ethnicity demographics, 80% had a study location with mostly non-Hispanic white students and 33% included a study location with mostly minority students. There is overlap in these data because two studies (Aseltine, James, Schilling, & Glanovsky, Citation2007; Wyman et al., Citation2010) had multiple locations with varied demographics. Only one program (American Indian Life Skills) was designed for an indigenous population (LaFromboise & Howard-Pitney, Citation1994), although the Adolescent Depression Awareness Program also included indigenous youth in one of its study locations (Swartz et al., Citation2017; Townsend et al., Citation2019).
Program Features
provides factors to consider for implementation of these programs. Program delivery is most often carried out by trained facilitators or by health teachers who are certified after specific training. Programs differ in scope and goals. Some programs seek to change the norms of the school environment. Sources of Strength, for example, trains and supervises diverse peer leaders to support students and encourage help-seeking (Wyman et al., Citation2010), and the South Elgin program uses existing school mental health resources by empowering school social workers to use their training to deliver the program (Ciffone, Citation1993). This strategy indirectly introduces students to the school social worker and intends to create a welcoming environment if a student needs mental health intervention.
TABLE 3. Program features and contextual factors for implementation.
Three of the identified programs are not designed primarily for suicide prevention, but still meet STANDUP Act criteria and achieve relevant outcomes. The Adolescent Depression Awareness Program, for example, targets improving depression literacy while reducing mental health stigma. Headstrong aims to improve mental health literacy while also addressing suicide risk factor awareness. Teen Mental Health First Aid trains students to identify, understand, and respond to signs of mental illness among peers, including mental health crises and substance use.
Some studies expanded on programs by testing new additions and features. For example, Bockhoff et al. (2022) added teacher training components to Signs of Suicide and Petrova, Wyman, Schmeelk-Cone, and Pisani (Citation2015) added specific peer messaging to enhance Sources of Strength. These studies highlight the feasibility and potential effectiveness for schools to adapt programs to better fit the needs of their students.
Evidence Grading of Programs
provides each study’s individual quality level per the LEGEND system as well as the overall evidence GRADE for each program’s strength of evidence stratified by the four STANDUP Act outcomes. Two programs studied and achieved all four outcomes—Adapt for Life and Youth Aware of Mental Health. The Youth Aware of Mental Health program measured all, but its primary objective was to prevent STBs (Wasserman et al., Citation2015). The high grade for the body of evidence indicates a strong recommendation that the program is effective at preventing STBs. The scope, objectives, and effects of the program differ between outcomes, thus individual evidence grades for each STANDUP Act outcome are provided.
TABLE 4. Grading for program body of evidence stratified by outcome.
Signs of Suicide also has a high evidence grade in decreasing STBs among teens. It was also one of few programs that evaluated STBs in middle schools, although the European Youth Aware of Mental Health trial did include children under age 14 (Wasserman et al., Citation2015). In a sample of middle schoolers with suicidal ideation at time of enrollment, Schilling, Lawless, Buchanan, and Aseltine (Citation2014) showed a decrease in STBs through the Signs of Suicide program. For students who did not report suicidal ideation prior to program implementation, the effects were not statistically significant.
Other programs had success in non-STB measures, which may be of interest to schools trying to target a broader range of mental health outcomes. Sources of Strength was the only program with a moderate or high body of evidence grade in increasing resource awareness, though its outcomes varied by population. Improvements in help-seeking intentions and engaging a trusted adult were more pronounced in peer leaders than in the general student population, and the most significant increases were observed in urban schools.
The most common outcome measured by these programs was help-seeking behaviors and help-seeking intentions, with 11 of the 12 programs measuring help-seeking in some way. Help-seeking is a common barrier to adolescents in mental health crisis, and efforts to increase help-seeking behaviors are likely to result in positive outcomes for a population (Pisani et al., Citation2012). Evidence for help-seeking effectiveness ranged from very low to moderate grades, with no programs having a high grade for the body of evidence. Most programs (9 of 12) evaluated suicide awareness, depression knowledge, and/or mental health literacy. Resource awareness was the least-studied outcome, with only 50% of programs measuring this outcome.
DISCUSSION AND IMPLEMENTATION GUIDANCE
We conducted a rapid review of existing literature on school-based suicide prevention programs focusing on evaluation of 29 published studies for 12 programs that coincide with the criteria of the STANDUP Act. Based on our results, included studies and programs often target suicide prevention by encouraging adolescents to a) identify signs of distress in themselves or in peers and b) actively seek help from the resources available to them. The universal suicide prevention programs included in this review teach students about mental health, increase awareness of the risk factors for suicide, introduce them to helpful resources, and promote help-seeking behaviors. Many of these programs are feasible to implement and have been implemented and disseminated in the U.S. and other countries (e.g., Headstrong, Signs of Suicide, Sources of Strength, teen Mental Health First Aid, and Youth Aware of Mental Health).
Implementation Guidance
When a school implements such a program, it is expected that there will be an increase in students needing resources and asking for help during a crisis. Prior to implementation of a program, schools should assess their capacity to handle an increase in students needing resources and establish formal policies for suicide prevention and postvention (WHO, Citation2018; ASFP et al., 2019).
Recent legislative efforts (Hopeful Futures Campaign, Citation2022) can be leveraged to implement, scale-up, and sustain coordinated and multipronged school-based suicide prevention efforts that include universal (programs directed at all youth in the classroom such as the ones in this review), selective (programs directed at youth at elevated risk for suicide), and indicated approaches (treatment interventions for youth experiencing suicidal ideation and attempts). The Whole School, Whole Community, Whole Child (WSCC) model, developed in 2015 by the CDC and Association for Supervision and Curriculum Development outlines a multi-tiered approach to enhance the social and emotional climate in schools as well as counseling, psychological, and social services (Lewallen, Hunt, Potts-Datema, Zaza, & Giles, Citation2015). Lever et al. (Citation2023) highlights a variety of approaches that schools can use to align with the WSCC model and advance mental health support in schools. High quality implementation and fidelity of school-based interventions is associated with better impact on student outcomes (Wilcox, Petras, Brown, & Kellam, Citation2022; Botvin, Baker, Dusenbury, Botvin, & Diaz, Citation1995; Dane & Schneider, Citation1998), and it can thus influence sustainment after the initial funding for a program ends (Brown et al., 2018). Attention to these issues is ideally done in the planning stages prior to implementation.
Similar guidance is seen at the international level with the WHO Live Life: an Implementation Guide for Suicide Prevention in Countries (2021), which prioritizes fostering socio-emotional life skills in adolescents using school-based interventions. The WHO guide recommends that programs for students not be implemented in isolation, but rather coordinated with training for staff on how to recognize risk factors and warning signs of suicidal behavior, how to provide support to distressed young people, and how to refer students for additional support.
Schools should have clear policies and protocols for when suicide risk is identified, and protocols for supporting students returning to school following a suicide attempt. Schools should facilitate a safe environment, partner with community resources, involve parents to increase awareness of mental health risk factors, and develop initiatives to address additional risk factors for young people such as trauma and substance use.
Gaps in Literature
We identified gaps in the existing literature related to application of student-directed suicide prevention programs. One limitation is the lack of replication studies performed for many of the programs as well as limited data on fidelity, iatrogenic effects, cultural relevance for students of color, and long-term impacts and sustainment of the programs. Few studies target middle school students—only 17% of included studies—even though there is a need for suicide awareness and prevention training for pre-adolescents. Ideally school systems would consider stacking different types of programs by developmental timing.
Historically, suicide rates amongst white adolescents have been higher than other races and ethnicities in the U.S. However, there has been a recent narrowing of rates of suicide between such groups in the U.S. with a reduction in rates in white adolescents and an acceleration in suicide rates in adolescents of color from 2015-2020 (Benghanem, Paik, Aslani-Amoli, Henry, & Howell, Citation2022). Broad implementation and program impact among youth of color has not been studied in response to the rapidly rising suicide rates in minority youth. The highest rates of suicide are seen in the U.S. indigenous population (Ramchand, Gordon, & Pearson, Citation2021), but only one program (LaFromboise & Howard-Pitney, Citation1994) was designed for indigenous schools in the U.S.
Study Limitations
One limitation to our evidence synthesis is having one reviewer screen the search results. However, this strategy was used in parallel with reviewing the references of 11 recent systematic reviews and meta-analyses. The database search helped to verify that eligible studies were not missed and to identify studies that were published after the review materials. Vital components of rigor were maintained, such as having multiple reviewers perform independent evidence grading and bias assessments of studies using a standardized evidence evaluation system, and having an evidence methodologist review the search strategy.
Rapid reviews have potential biases and “may miss relevant information” when compared to a systematic review (Ganann, Ciliska, & Thomas, Citation2010, p. 7). However, a study by Watt et al. (Citation2008) found that between rapid reviews and full systematic reviews, “the essential conclusions of the rapid and full reviews did not differ extensively” (p. 1037). Similar results were seen by Reynen et al. (Citation2018) who reported that while systematic reviews could provide more detail, conclusions were generally consistent between systematic and rapid reviews. Furthermore, as Khangura, Konnyu, Cushman, Grimshaw, and Moher (Citation2012) noted, rapid review methodology “deliver(s) evidence in both a timely manner and usable format […] to decision makers” (pp. 6-8), which was the most appropriate approach for our study considering the lack of guidance for school districts in school-based program selection. Thus, this rapid review has much to offer in spite of noted limitations.
We also limited our findings to programs with implementation materials available in English. There are multiple interventions in the literature that are shown to be effective but cannot be readily implemented in the U.S. Those can serve as frameworks for schools in the U.S. that want to adapt existing programs or design their own intervention, but that was out of the scope of this review. As our review was focused on implementation and rollout of the STANDUP Act, a U.S. statute, we limited ourselves to English language programs. Ideally, future program developers will adapt their programs to include implementation materials in other languages.
Several promising programs have been excluded due to a lack of peer-reviewed data or a control group. The absence of this evidence does not equate with lack of effectiveness, but eligibility for inclusion in this review requires at least one controlled study. Two well-known programs (Hope Squad and SafeTALK) are actively conducting research that may add to the evidence base in the future. Evidence grades for programs that are not suicide-specific are limited in that those programs are less likely to measure all outcomes relevant to the STANDUP Act. Thus, their grades may be lower. However, we included three in this review (Adolescent Depression Awareness Program, Headstrong, and Teen Mental Health First Aid). These programs allow schools the opportunity to address suicide prevention by targeting depression directly or by targeting a broad range of youth mental health challenges through increasing mental health literacy, reducing mental health stigma, and enhancing student skills to help a peer in crisis.
CONCLUSIONS
The STANDUP Act provides an avenue for educational and tribal agencies to seek funding for student-directed suicide prevention and awareness training to prevent suicide, improve help-seeking behaviors, increase suicide knowledge, and increase awareness of available resources. While multiple systematic reviews and meta-analyses have examined school-based suicide prevention, no reviews to date have focused on programs eligible for funding under the STANDUP Act that have existing implementation materials readily available for U.S. schools. Our review is also the first to aggregate studies in order to grade the overall body of evidence for each program. Our review identified 29 applicable studies that met inclusion criteria, which represented 12 unique mental health school-based programs. The data presented here on program evidence and the details presented on program implementation requirements provide direct and useable guidance for local officials to select such programs and apply for associated funding.
Moving forward, this review can serve to enhance implementation guidance in response to suicide prevention legislation for public health workers, school health officials, and mental health professionals in the U.S. and across the globe. Ideally this review could also be the basis for a living resource that is periodically updated as the research and implementation evidence evolves. We encourage other mental health experts and researchers to engage in similar review processes to ensure that such funding for mental health programs is used to its greatest potential with evidence-based interventions.
ACKNOWLEDGEMENTS
The authors thank Aubrey DeVinney for her role in data collection.
DISCLOSURE STATEMENT
Landon Krantz and Danette Stanko-Lopp have no relevant financial or non-financial interests to declare.
Holly Wilcox received research support from the National Institute of Mental Health for a study of Youth Aware of Mental Health in urban middle school students (R34MH121639) and has received funding from the National Council for Mental Wellbeing for research evaluation of the teen Mental Health First Aid program in the U.S. Holly Wilcox is an unpaid member of the Mental Health First Aid Research Advisory Group and an unpaid member of the Maryland School Board. Holly Wilcox is a coauthor on three studies identified in our search.
Matt Kuntz’s NAMI Montana organization provides financial support to the Youth Aware of Mental Health program at Montana State University. Matt Kuntz’s NAMI Montana organization receives grant funding from the Oro y Plata Foundation and the Montana Healthcare Foundation.
Additional information
Funding
Notes on contributors
Landon B. Krantz
Landon Krantz, MD (Twitter @LandonKrantz_MD) (linkedin.com/in/landon-krantz/) is a general pediatrician with over five years of clinical experience caring for adolescents with mental illness. Dr. Krantz is currently an academic research fellow at Cincinnati Children’s Hospital Medical Center in the Division of General & Community Pediatrics and is completing a Masters of Health Sciences in maternal child health at the Johns Hopkins Bloomberg School of Public Health.
Danette Stanko-Lopp
Danette Stanko-Lopp, MA, MPH is a health policy and clinical effectiveness researcher at Cincinnati Children’s Hospital Medical Center with expertise in evidence evaluation. She has led teams in developing large-scale clinical guidelines and evidence recommendations in the field of pediatrics.
Matt Kuntz
Matt Kuntz, JD has been the executive director of the National Alliance on Mental Illness for Montana (NAMI Montana) since 2008, leading advocacy efforts for all Montanans suffering from serious mental illness and their families. He is also an accomplished author on PTSD and bipolar, and has been involved in legislative work to improve mental health care for veterans.
Holly C. Wilcox
Holly C. Wilcox, Ph.D (Twitter @DrHollyWilcox) is a professor at Johns Hopkins Bloomberg School of Public Health in the department of Mental Health with joint appointments in the Department of Health Policy and Management as well as the Johns Hopkins Schools of Medicine and Education. She leads a multidisciplinary, interdepartmental suicide prevention work group and public health-oriented program of suicide research and prevention at Johns Hopkins. Correspondence concerning this author should be addressed to Landon Krantz. Email: [email protected]
REFERENCES
- American Academy of Pediatrics. (2022, February 16). Blueprint for Youth Suicide Prevention. Retrieved October 1, from http://www.aap.org/suicideprevention.
- American Foundation for Suicide Prevention, American School Counselor Association, National Association of School Psychologists, & The Trevor Project. (2019). Model school district policy on suicide prevention: Model language, commentary, and resources (2nd ed.). American Foundation for Suicide Prevention. Retrieved October 1, 2022, from https://www.thetrevorproject.org/wp-content/uploads/2021/08/Model_School_Policy_Booklet.pdf.
- American Foundation for Suicide Prevention. (2022, February 18). State laws: Suicide prevention in schools (k-12). Retrieved December 1, from https://afsp.org/suicide-prevention-in-k-12-schools.
- Aseltine, R. H., Jr., & DeMartino, R. (2004). An outcome evaluation of the SOS Suicide Prevention Program. American Journal of Public Health, 94(3), 446–451. doi:10.2105/ajph.94.3.446
- Aseltine, R. H., Jr, James, A., Schilling, E. A., & Glanovsky, J. (2007). Evaluating the SOS suicide prevention program: A replication and extension. BMC Public Health, 7(1), 161. doi:10.1186/1471-2458-7-161
- Beaudry, M. B., Swartz, K., Miller, L., Schweizer, B., Glazer, K., & Wilcox, H. (2019). Effectiveness of the adolescent depression awareness program (ADAP) on depression literacy and mental health treatment. The Journal of School Health, 89(3), 165–172. doi:10.1111/josh.12725
- Benghanem, G., Paik, J., Aslani-Amoli, B., Henry, L., & Howell, J. (2022). 94 Adolescents’ suicide rates by ethnicity – Data from the National Vital Statistics System 2015–2020. Annals of Emergency Medicine, 80(4), S46–S47. doi:10.1016/j.annemergmed.2022.08.117
- Bipartisan Safer Communities Act. 20 U.S.C. §7906. (2022). Retrieved October 10, 2022, from https://www.congress.gov/bill/117th-congress/senate-bill/2938/text.
- Bockhoff, K., Ellermeier, W., & Bruder, S. (2023). Evaluation of a suicide prevention program encompassing both student and teacher training components. Crisis, 44(4), 276–284. doi:10.1027/0227-5910/a000862
- Botvin, G. J., Baker, E., Dusenbury, L., Botvin, E. M., & Diaz, T. (1995). Long-term follow-up results of a randomized drug abuse prevention trial in a white middle-class population. JAMA: The Journal of the American Medical Association, 273(14), 1106–1112. doi:10.1001/jama.1995.03520380042033
- Brann, K. L., Baker, D., Mills, K. S. M., Watt, S. J., & Diorio, C. (2021). A meta-analysis of suicide prevention programs for school-aged youth. Children and Youth Services Review, 121, 105826. doi:10.1016/j.childyouth.2020.105826
- Braun, M., Till, B., Pirkis, J., & Niederkrotenthaler, T. (2021a). Suicide prevention videos developed by and for adolescents. Crisis, 42(2), 114–120. doi:10.1027/0227-5910/a000696
- Braun, M., Till, B., Pirkis, J., & Niederkrotenthaler, T. (2021b). Effects of suicide prevention videos developed by and targeting adolescents: A randomized controlled trial. European Child & Adolescent Psychiatry, 32(5), 847–857. doi:10.1007/s00787-021-01911-6
- Brown, C. H., Curran, G., Palinkas, L. A., Aarons, G. A., Wells, K. B., Jones, L., … Cruden, G. (2017). An overview of research and evaluation designs for dissemination and implementation. Annual Review of Public Health, 38, 1–22. doi:10.1146/annurev-publhealth-031816-044215
- Calear, A. L., McCallum, S. M., Christensen, H., Mackinnon, A. J., Nicolopoulos, A., Brewer, J. L., … Batterham, P. J. (2022). The Sources of Strength Australia project: A cluster randomised controlled trial of a peer-connectedness school-based program to promote help-seeking in adolescents. Journal of Affective Disorders, 299, 435–443. doi:10.1016/j.jad.2021.12.043
- Centers for Disease Control and Prevention. (2022). Web-based injury statistics query and reporting system (WISQARS). National Center for Injury Prevention and Control, Centers for Disease Control and Prevention. Retrieved September 5, 2022, from http://www.cdc.gov/ncipc/wisqars.
- Centers for Disease Control and Prevention. (2021). Youth risk behavior survey data summary and trends report. Retrieved May 5, 2023, from www.cdc.gov/YRBSS.
- Ciffone, J. (1993). Suicide prevention: A classroom presentation to adolescents. Social Work, 38(2), 197–203.
- Ciffone, J. (2007). Suicide prevention: An analysis and replication of a curriculum-based high school program. Social Work, 52(1), 41–49. doi:10.1093/sw/52.1.41
- Clark, E., Burkett, K., & Stanko-Lopp, D. (2009). Let evidence guide every new decision (LEGEND): An evidence evaluation system for point-of-care clinicians and guideline development teams. Journal of Evaluation in Clinical Practice, 15(6), 1054–1060. doi:10.1111/j.1365-2753.2009.01314.x
- Curtin, S. C., Hedegaard, H., & Ahmad, F. B. (2021). (2020). Provisional numbers and rates of suicide by month and demographic characteristics: United States. Vital Statistics Rapid Release (Report No. 16, 43–49. National Center for Health Statistics. doi:10.1136/ip.2009.025502
- Dane, A. V., & Schneider, B. H. (1998). Program integrity in primary and early secondary prevention: Are implementation effects out of control? Clinical Psychology Review, 18(1), 23–45. doi:10.1016/s0272-7358(97)00043-3
- Elementary and Secondary Education Act of 1965, 20 U.S.C. §7112(6). (1965). Retrieved July 30, 2022, from https://www.congress.gov/congressional-report/114th-congress/house-report/354/1.
- Ganann, R., Ciliska, D., & Thomas, H. (2010). Expediting systematic reviews: Methods and implications of rapid reviews. Implementation Science, 5(1), 56. doi:10.1186/1748-5908-5-56
- Garritty, C., Gartlehner, G., Nussbaumer-Streit, B., King, V. J., Hamel, C., Kamel, C., … Stevens, A. (2021). Cochrane rapid reviews methods group offers evidence-informed guidance to conduct rapid reviews. Journal of Clinical Epidemiology, 130, 13–22. doi:10.1016/j.jclinepi.2020.10.007
- Gijzen, M. W. M., Rasing, S. P. A., Creemers, D. H. M., Engels, R. C. M. E., & Smit, F. (2022). Effectiveness of school-based preventive programs in suicidal thoughts and behaviors: A meta-analysis. Journal of Affective Disorders, 298(Pt A), 408–420. doi:10.1016/j.jad.2021.10.062
- Hart, L. M., Mason, R. J., Kelly, C. M., Cvetkovski, S., & Jorm, A. F. (2016). teen Mental Health First Aid’: A description of the program and an initial evaluation. International Journal of Mental Health Systems, 10(1), 3. doi:10.1186/s13033-016-0034-1
- Hart, L. M., Morgan, A. J., Rossetto, A., Kelly, C. M., Mackinnon, A., & Jorm, A. F. (2018). Helping adolescents to better support their peers with a mental health problem: A cluster-randomised crossover trial of teen Mental Health First Aid. The Australian and New Zealand Journal of Psychiatry, 52(7), 638–651. doi:10.1177/0004867417753552
- Hart, L. M., Cropper, P., Morgan, A. J., Kelly, C. M., & Jorm, A. F. (2020). teen Mental Health First Aid as a school-based intervention for improving peer support of adolescents at risk of suicide: Outcomes from a cluster randomised crossover trial. The Australian and New Zealand Journal of Psychiatry, 54(4), 382–392. doi:10.1177/0004867419885450
- Hart, L. M., Morgan, A. J., Rossetto, A., Kelly, C. M., Gregg, K., Gross, M., … Jorm, A. F. (2022). teen Mental Health First Aid: 12-month outcomes from a cluster crossover randomized controlled trial evaluation of a universal program to help adolescents better support peers with a mental health problem. BMC Public Health, 22(1), 1159. doi:10.1186/s12889-022-13554-6
- Health and Human Services Press Office. (2021, December 7). U.S. surgeon general issues advisory on youth mental health crisis further exposed by COVID-19 pandemic. HHS Press Release. Retrieved October 1, 2022, from https://www.hhs.gov/about/news/2021/12/07/us-surgeon-general-issues-advisory-on-youth-mental-health-crisis-further-exposed-by-covid-19-pandemic.html.
- Hopeful Futures Campaign. (2022, August). State legislative guide for school mental health. Hopeful Futures Campaign. Retrieved December 1, from https://hopefulfutures.us/.
- Institute of Medicine (US) Committee on Prevention of Mental Disorders. (1994). Mrazek, P. J., & Haggerty, R. J. (Eds.) Reducing risks for mental disorders: frontiers for preventive intervention research. Washington (DC): National Academies Press (US).
- Jones, S. E., Ethier, K. A., Hertz, M., DeGue, S., Le, V. D., Thornton, J., … Geda, S. (2022). Mental health, suicidality, and connectedness among high school students during the COVID-19 pandemic - adolescent behaviors and experiences survey, United States, January–June 2021. MMWR Supplements, 71(3), 16–21. doi:10.15585/mmwr.su7103a3
- Kalafat, J., & Elias, M. (1994). An evaluation of a school-based suicide awareness intervention. Suicide & Life-Threatening Behavior, 24(3), 224–233. doi:10.15585/mmwr.su7103a3
- Khangura, S., Konnyu, K., Cushman, R., Grimshaw, J., & Moher, D. (2012). Evidence summaries: The evolution of a rapid review approach. Systematic Reviews, 1(1), 10. doi:10.1186/2046-4053-1-10
- King, K. A., Strunk, C. M., & Sorter, M. T. (2011). Preliminary effectiveness of surviving the teens(®) suicide prevention and depression awareness program on adolescents’ suicidality and self-efficacy in performing help-seeking behaviors. The Journal of School Health, 81(9), 581–590. doi:10.1111/j.1746-1561.2011.00630.x
- LaFromboise, T. D., & Howard-Pitney, B. (1994). The Zuni Life Skills Development curriculum: A collaborative approach to curriculum development. American Indian and Alaska Native Mental Health Research (Monographic Series), 4, 98–121. doi:10.5820/aian.mono04.1994.98
- Lewallen, T. C., Hunt, H., Potts-Datema, W., Zaza, S., & Giles, W. (2015). The Whole School, Whole Community, Whole Child model: A new approach for improving educational attainment and healthy development for students. The Journal of School Health, 85(11), 729–739. doi:10.1111/josh.12310
- Lever, N., Orenstein, S., Jaspers, L., Bohnenkamp, J., Chung, J., & Hager, E. (2023). Using the whole school, whole community, whole child model to support mental health in schools. The Journal of School Health. Advance online publication. doi:10.1111/josh.13322.
- Lindow, J. C., Hughes, J. L., South, C., Minhajuddin, A., Gutierrez, L., Bannister, E., … Byerly, M. J. (2020). The Youth Aware of Mental Health intervention: Impact on help seeking, mental health knowledge, and stigma in U.S. adolescents. The Journal of Adolescent Health: Official Publication of the Society for Adolescent Medicine, 67(1), 101–107. doi:10.1016/j.jadohealth.2020.01.006
- Mann, J. J., Michel, C. A., & Auerbach, R. P. (2021). Improving suicide prevention through evidence-based strategies: A systematic review. The American Journal of Psychiatry, 178(7), 611–624. doi:10.1176/appi.ajp.2020.20060864
- McGillivray, L., Shand, F., Calear, A. L., Batterham, P. J., Rheinberger, D., Chen, N. A., … Torok, M. (2021). The Youth Aware of Mental Health program in Australian secondary schools: 3- and 6-month outcomes. International Journal of Mental Health Systems, 15(1), 79. doi:10.1186/s13033-021-00503-w
- Midgett, A., Doumas, D. M., Peralta, C., Bond, L., & Flay, B. (2020). Impact of a brief, bystander bullying prevention program on depressive symptoms and passive suicidal ideation: A program evaluation model for school personnel. Journal of Prevention and Health Promotion, 1(1), 80–103. doi:10.1177/2632077020942959
- Ogawa, S., Suzuki, H., Takahashi, T., Fujita, K., Murayama, Y., Sato, K., … Fujiwara, Y. (2022). Suicide prevention program with cooperation from senior volunteers, governments, and schools: A study of the intervention effects of “Educational lessons regarding SOS output” focusing on junior high school students. Children, 9(4), 541. doi:10.1080/02796015.2009.12087830
- Perry, Y., Petrie, K., Buckley, H., Cavanagh, L., Clarke, D., Winslade, M., … Christensen, H. (2014). Effects of a classroom-based educational resource on adolescent mental health literacy: A cluster randomized controlled trial. Journal of Adolescence, 37(7), 1143–1151. doi:10.1016/j.adolescence.2014.08.001
- Petrova, M., Wyman, P. A., Schmeelk-Cone, K., & Pisani, A. R. (2015). Positive-themed suicide prevention messages delivered by adolescent peer leaders: Proximal impact on classmates’ coping attitudes and perceptions of adult support. Suicide & Life-Threatening Behavior, 45(6), 651–663. doi:10.1111/sltb.12156
- Pisani, A. R., Schmeelk-Cone, K., Gunzler, D., Petrova, M., Goldston, D. B., Tu, X., & Wyman, P. A. (2012). Associations between suicidal high school students’ help-seeking and their attitudes and perceptions of social environment. Journal of Youth and Adolescence, 41(10), 1312–1324. doi:10.1007/s10964-012-9766-7
- Ramchand, R., Gordon, J. A., & Pearson, J. L. (2021). Trends in suicide rates by race and ethnicity in the United States. JAMA Network Open, 4(5), e2111563. doi:10.1001/jamanetworkopen.2021.11563
- Reynen, E., Robson, R., Ivory, J., Hwee, J., Straus, S. E., Pham, B., & Tricco, A. C. (2018). A retrospective comparison of systematic reviews with same-topic rapid reviews. Journal of Clinical Epidemiology, 96, 23–34. doi:10.1016/j.jclinepi.2017.12.001
- Sandy Hook Promise. (n.d). What is The STANDUP Act. Retrieved December 5, 2022, from https://actionfund.sandyhookpromise.org/issues/mental-health-and-wellness/prevent-youth-suicide/.
- Schilling, E. A., Lawless, M., Buchanan, L., & Aseltine, R. H. Jr (2014). “Signs of Suicide” shows promise as a middle school suicide prevention program. Suicide & Life-Threatening Behavior, 44(6), 653–667. doi:10.1111/sltb.12097
- Schilling, E. A., Aseltine, R. H., Jr., & James, A. (2016). The SOS suicide prevention program: further evidence of efficacy and effectiveness. Prevention Science: The Official Journal of the Society for Prevention Research, 17(2), 157–166. doi:10.1007/s11121-015-0594-3
- STANDUP Act of 2021, 42 U.S.C. §290bb-32. (2022). Retrieved May 5, 2022, from https://www.congress.gov/bill/117th-congress/senate-bill/1543/text.
- Strunk, C. M., King, K. A., Vidourek, R. A., & Sorter, M. T. (2014). Effectiveness of the surviving the Teens® suicide prevention and depression awareness program: An impact evaluation utilizing a comparison group. Health Education & Behavior : The Official Publication of the Society for Public Health Education, 41(6), 605–613. doi:10.1177/1090198114531774
- Swartz, K. L., Kastelic, E. A., Hess, S. G., Cox, T. S., Gonzales, L. C., Mink, S. P., & DePaulo, J. R. Jr (2010). The effectiveness of a school-based adolescent depression education program. Health Education & Behavior: The Official Publication of the Society for Public Health Education, 37(1), 11–22. doi:10.1177/1090198107303313
- Swartz, K., Musci, R. J., Beaudry, M. B., Heley, K., Miller, L., Alfes, C., … Wilcox, H. C. (2017). School-based curriculum to improve depression literacy among US secondary school students: A randomized effectiveness trial. American Journal of Public Health, 107(12), 1970–1976. doi:10.2105/AJPH.2017.304088
- Townsend, L., Musci, R., Stuart, E., Heley, K., Beaudry, M. B., Schweizer, B., … Wilcox, H. (2019). Gender differences in depression literacy and stigma after a randomized controlled evaluation of a universal depression education program. The Journal of Adolescent Health : Official Publication of the Society for Adolescent Medicine, 64(4), 472–477. doi:10.1016/j.jadohealth.2018.10.298
- Tricco, A. C., Antony, J., Zarin, W., Strifler, L., Ghassemi, M., Ivory, J., … Straus, S. E. (2015). A scoping review of rapid review methods. BMC Medicine, 13(1), 224. doi:10.1186/s12916-015-0465-6
- Walsh, E. H., McMahon, J., & Herring, M. P. (2022). Research Review: The effect of school-based suicide prevention on suicidal ideation and suicide attempts and the role of intervention and contextual factors among adolescents: A meta-analysis and meta-regression. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 63(8), 836–845. doi:10.1111/jcpp.13598
- Wasserman, D., Hoven, C. W., Wasserman, C., Wall, M., Eisenberg, R., Hadlaczky, G., … Carli, V. (2015). School-based suicide prevention programmes: The SEYLE cluster-randomised, controlled trial. Lancet (London, England), 385(9977), 1536–1544. doi:10.1016/S0140-6736(14)61213-7
- Watt, A., Cameron, A., Sturm, L., Lathlean, T., Babidge, W., Blamey, S., … Maddern, G. (2008). Rapid versus full systematic reviews: Validity in clinical practice? ANZ Journal of Surgery, 78(11), 1037–1040. doi:10.1111/j.1445-2197.2008.04730.x
- Wilcox, H. C., Petras, H., Brown, H. C., & Kellam, S. G. (2022). Testing the impact of the whole-day Good Behavior Game on aggressive behavior: Results of a classroom-based randomized effectiveness trial. Prevention Science: The Official Journal of the Society for Prevention Research, 23(6), 907–921. doi:10.1007/s11121-022-01334-y
- World Health Organization. (2018). Preventing suicide: A community engagement toolkit. Retrieved May 5, 2023, from https://www.who.int/europe/publications/i/item/9789241513791.
- World Health Organization. (2021). Live life: An implementation guide for suicide prevention in countries. Retrieved May 5, 2023, from https://www.who.int/publications/i/item/9789240026629.
- Wyman, P. A., Brown, C. H., LoMurray, M., Schmeelk-Cone, K., Petrova, M., Yu, Q., … Wang, W. (2010). An outcome evaluation of the Sources of Strength suicide prevention program delivered by adolescent peer leaders in high schools. American Journal of Public Health, 100(9), 1653–1661. doi:10.2105/AJPH.2009.190025
- Yard, E., Radhakrishnan, L., Ballesteros, M. F., Sheppard, M., Gates, A., Stein, Z., … Stone, D. M. (2021). Emergency department visits for suspected suicide attempts among persons aged 12-25 years before and during the COVID-19 pandemic - United States, January 2019-May 2021. MMWR. Morbidity and Mortality Weekly Report, 70(24), 888–894. doi:10.15585/mmwr.mm7024e1