
ABSTRACT
Despite the influence of the integrated motivational-volitional (IMV)1 model on research and practice, the supporting literature has not been systematically synthesised. This systematic review aims to synthesise the literature testing the IMV model of suicidal behaviour. Using citation and database searching, PsycINFO, EMBASE, PubMed, Web of Science, and Google Scholar were searched for studies referencing the IMV model (last searched on 28th March 2023). Included studies empirically tested the hypotheses of the model. Quality assessment was conducted using the National Institute of Health tool. Findings from 98 records (100 studies, 138,365 participants) were narratively synthesised. Results from studies directly testing the hypothesised pathways of the model supported the defeat-entrapment-suicidal ideation pathway of the IMV model. Case–control studies comparing differences between control, ideation, and enactment groups were consistent with hypotheses in univariate and cross-sectional analyses. However, support for the model was mixed for case–control multivariate and prospective studies. Due to low overlap in variables studied, the role of specific pre-motivational phase variables and stage-specific moderators was inconclusive. The studies received overall good quality ratings. The IMV model presents a promising framework for understanding and preventing suicide. Defeat, entrapment, and key variables may be useful in informing suicide prevention measures.
Suicide results in 703,000 deaths every year globally and is the sixth leading cause of death worldwide between the ages of 15–49 (Ritchie et al., Citation2018; World Health Organisation, Citation2021). Despite significant improvements in preventing other leading causes of death, our ability to predict and prevent suicide has shown little improvement over the past five decades (Franklin et al., Citation2017; Naghavi et al., Citation2017). This is largely due to individual risk factors being limited in explaining the processes giving rise to suicidal ideation (thoughts about taking one’s life), and how they result in suicidal behaviours (any self-directed harm irrespective of intent to die as a result) (Franklin et al., Citation2017; Millner et al., Citation2020). Recent research on suicide has highlighted that suicidal behaviours are likely influenced by interrelationships between hundreds of biological, psychological, social, and cultural factors (Chu et al., Citation2017; Levi-Belz et al., Citation2019; O’Connor & Nock, Citation2014). Understanding how different risk factors interact to give rise to suicidal thoughts and behaviours using theoretical frameworks is key to the effective identification and prevention of suicide (Klonsky et al., Citation2018; Stanley et al., Citation2016). Thus, it is important that theoretical frameworks aiming to explain suicide account for a range of distal and proximal, contextual, and individual factors. It is also crucial that suicide theories explain the processes that influence individuals with suicidal thoughts to act upon those thoughts (Klonsky et al., Citation2018; Nock et al., Citation2016).
The integrated motivational-volitional (IMV) model of suicidal behaviour (O’Connor, Citation2011a; O’Connor & Kirtley, Citation2018) draws from a range of established theoretical models in suicide, health psychology literature, and empirical evidence to identify a common modifiable pathway giving rise to suicidal thoughts and behaviour (Barzilay & Apter, Citation2014; Gilbert & Allan, Citation1998; Joiner, Citation2005; Schotte & Clum, Citation1987; Van Orden et al., Citation2010; Williams, Citation2001). It highlights biological, psychological, and environmental variables at each stage of this pathway, illuminating potential targets for intervention. The IMV model also extends variables facilitating the transition from suicidal ideation to behaviour to include a more comprehensive set of variables consistent with the empirical literature (Klonsky et al., Citation2018).
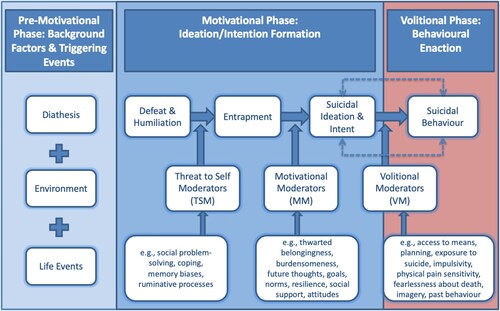
Fundamentally, the IMV model describes suicidal behaviour as arising out of three distinct phases (). First, the pre-motivational phase consists of the distal predisposing factors characterised by biological vulnerabilities (e.g., genetics), psychological vulnerabilities (e.g., perfectionism), life events (e.g., childhood experiences) and environmental or contextual variables (e.g., socio-economic status) (O’Connor & Kirtley, Citation2018). Such vulnerabilities confer an increased likelihood of feeling defeated or humiliated in the presence of stressors. Second, the motivational phase outlines the process by which suicidal ideation develops. Here, defeat and humiliation are feelings of failure and rejection while entrapment entails an inescapable sense of being trapped either within oneself (internal entrapment) or within circumstance (external entrapment). It is hypothesised that feelings of defeat and humiliation result in increased feelings of entrapment (Gilbert & Allan, Citation1998; Williams, Citation2001). Furthermore, individuals are more or less likely to experience entrapment depending on the presence of specific threat-to-self moderators (e.g., problem-solving, memory biases, coping). As such, the defeat-entrapment association is moderated by threat-to-self moderators. Individuals that are feeling trapped could thus begin to view suicide as way to escape. The likelihood of this may depend on the presence or absence of specific motivational moderators (e.g., thwarted belongingness, perceived burdensomeness, resilience). As such, the IMV model hypothesises that defeat indirectly leads to suicidal ideation through entrapment and the entrapment-suicidal ideation link is moderated by motivational moderators. Finally, the volitional phase describes the association between suicidal ideation and intent and suicidal behaviour. Specifically, it is hypothesised that thinking about suicide may lead to suicidal behaviour. Volitional moderators (e.g., access to means, past behaviour) determine whether the transition from thinking about suicide to acting upon these thoughts could occur (O’Connor & Kirtley, Citation2018).
Figure 1. The integrated motivational-volitional model of suicidal behaviour (O’Connor, 2011a; O’Connor & Kirtley, Citation2018).
Since the IMV model was first proposed (O’Connor, Citation2011a, Citation2011b), a growing body of literature has aimed to test its predictions (e.g., del Carpio et al., Citation2020; Dhingra et al., Citation2015; Dhingra et al., Citation2016b; Forkmann & Teismann, Citation2017; Ordóñez-Carrasco et al., Citation2020a, Citation2021a; Russell et al., Citation2020c; Tucker et al., Citation2016). The IMV model has also played a key role in informing local and national suicide prevention policy (e.g., Scottish Government, Citation2022), risk screening (de Sousa et al., Citation2020; Sandford et al., Citation2022), and intervention development (Nuij et al., Citation2018; O’Connor et al., Citation2017).
Despite its influence on research, practice and policy, the extent to which the hypotheses of the IMV model are empirically supported is unclear. For instance, the list of pre-motivational phase variables, motivational phase moderators (threat-to-self and motivational moderators), and volitional phase moderators (volitional moderators) are not exhaustive. As a result, Individual studies often test a sub-set of these variables. For example, a majority of studies have tested components of the model such as the motivational or volitional phase alone (Lucht et al., Citation2020, p. 17; McClelland et al., Citation2021; Ribiero et al., Citation2021). While these studies have provided useful results for specific aspects and variables in the model, they provide limited evidence regarding the interplay of different variables across the entire model. Additionally, individual studies are conducted among certain populations, with specific methodological characteristics such as design and measures used. For example, studies conducted among school children may not generalise to other populations. Similarly, some studies examined the hypothesised pathways in the IMV model while others compared differences in IMV model variables among groups of individuals with no history of suicidal thoughts or behaviours (control group), individuals with a history of suicidal thoughts but no behaviours (ideation group), and individuals with a history of behaviours (enactment group). Comparing the findings of studies in different populations and study designs would be useful in understanding the applicability of the IMV model. However, these studies testing the hypotheses of the IMV model have yet to be systematically reviewed.
The present review aims to systematically review and synthesise the evidence for the hypothesised relationships in the Integrated Motivational – Volitional model of suicidal behaviour. Specifically, we aim to address the following research questions: 1. To what extent have all components in the IMV model been tested in a single study? 2. What is the evidence for the association between pre-motivational phase variables (diathesis, environment, and life events) and variables in the motivational phase (defeat and humiliation, entrapment, and suicidal ideation)? 3. What is the evidence for associations between defeat, entrapment, and suicidal ideation? 4. To what extent is the association between defeat and entrapment moderated by threat-to-self moderators? 5. To what extent is the association between entrapment and suicidal ideation/intent moderated by motivational moderators? 6. What is the evidence for the association between suicidal ideation and suicidal behaviour and how is this association influenced by volitional moderators? 7. Do the associations in the IMV model vary across study characteristics?
Systematically reviewing the studies testing the IMV model would provide an understanding of which variables and pathways of the model are well supported by evidence. It would also highlight the generalisability of the findings, identify gaps in research, and present directions for future research. This would also be useful in advancing theory and inform evidence-based policy and interventions (Impellizzeri & Bizzini, Citation2012).
Methods
Screening and inclusion
The current systematic review adopted forward citation mining as the primary method used to find documents that reference the article that proposed this model (O’Connor, 2011a) and the updated the model (O’Connor & Kirtley, Citation2018). As studies aiming to test the IMV model will be expected to reference the articles that proposed the original and updated the model, forward citation mining was determined as the best strategy to identify these studies. The following sources were searched using citation mining: PsycINFO, EMBASE, PubMed, Web of Science, and google scholar (https://scholar.google.com/), between 8th July 2021 and 6th August 2021. The searches were last updated on March 28th, 2023. Based on feedback during the peer-review process, additional forward citation mining was undertaken using the same databases specified above to identify any studies citing the book chapter on the IMV model published in the International Handbook of suicide prevention (O’Connor, Citation2011b) on 20th July 2023. Four papers were identified and included as a result.
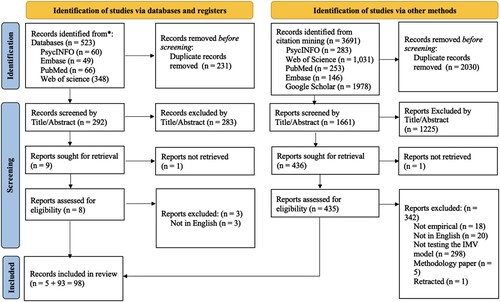
The updates were conducted by executing the original searches again and manually comparing the new set of records to the original set of records and including newly identified records. As recommended by Bramer and Bain (Citation2017), the total number of unique records identified from each search are reported in a flow diagram in . An additional search strategy was also included in an update using the same databases: PsycINFO, EMBASE, PubMed, and Web of Science (Core collection, Current Contents connect, BIOSIS Previews, BIOSIS Citation Index, Data Citation Index, SciELO Citation Index). For this, all searches were filtered by language (English) and year of publication (After 2011). The following search strings were used for each database: PsycINFO: ‘Integrated Motivational-Volitional Model OR (integrated N2 motivational N2 volitional) OR IMV model’, Embase: ‘Integrated Motivational-Volitional Model OR (integrated adj2 motivational adj2 volitional) OR IMV model’, Web of Science: ‘Integrated Motivational-Volitional Model OR (integrated NEAR/2 motivational Near/2 volitional) OR IMV model’, Pubmed: ‘Integrated Motivational-Volitional Model OR (integrated AND motivational AND volitional) OR IMV model’. Duplicate removal and screening were conducted manually using the Endnote referencing software by the first reviewer. Based on previous literature (Moore et al., Citation2022), 10% (n = 29) of the papers were originally randomly selected using an online random sequence generator (https://www.random.org/) and independently screened by a second reviewer. However, due to the addition of papers during updates to the original search and during the peer review process, this proportion is 6.54% (n = 29) of all records selected for full-text screening. The interrater reliability was (78.79%; Kappa = 0.53). Any disagreements were resolved by discussion with the review team and did not result in changes to the review protocol.
Figure 2. PRISMA Flowchart illustrating the screening and inclusion process.
Studies were included or excluded based on the following eligibility criteria:
Studies empirically testing at least one of the following associations within the IMV model were included:
The association between pre-motivational phase variables including diathesis, environment, life events and vulnerability to defeat and humiliation.
The association between defeat and humiliation and entrapment, or entrapment and suicidal ideation, or suicidal ideation and behaviour.
Moderators influencing the relationship between defeat and entrapment, entrapment and suicidal ideation, or suicidal ideation and action.
Differences in theoretically relevant variables between individuals with no history of suicidal ideation or behaviour on the one hand, versus individuals with a history of suicidal ideation but not behaviour, and individuals with suicidal behaviour.
Studies published in English were included.
Review articles and book chapters only providing overviews of literature and/or recommendations for practice were excluded.
A total of 98 records (100 studies as two doctoral theses reported 2 eligible studies each) that met the inclusion criteria were included in the systematic review (See Appendix A & B for included studies and study characteristics). Several papers appeared to meet the inclusion criteria but were excluded on closer inspection. In four of these papers, the writing suggested that suicide-related outcomes were being investigated. However, the measures used were not valid measures of suicidal thoughts or behaviours. Studies were also excluded if none of the associations outlined in the inclusion criteria (such as pre-motivational phase variables and defeat, or defeat and entrapment) were being tested. Three cited the IMV model in the introduction but were primarily informed by other models, two studies observed suicidal thoughts as covariates while examining associations between other variables and suicidal behaviour, and one study tested the ability of various psychometric measures in predicting suicidal behaviour. Finally, one study observed entrapment as a mediator of the relationship between attachment styles and suicidal behaviour and one observed the relationship between defeat and suicidal ideation directly. As this does not meet the conditions set out in the inclusion criteria, it was excluded.
Data extraction and synthesis
A piloted data extraction form was used to collect data manually from the records by the first reviewer. The data extracted included the following information specific to analyses aimed at testing the IMV model: Publication details (title, type of document, authors, and year of publication), study characteristics (research question/aims, hypotheses, study design, length of follow up, attrition rate, risk/protective factors and outcomes, moderators/mediators, covariates/confounding variables, and conclusions), data collection (sample size, demographic data, time frames, population, eligibility criteria, method of recruitment, participant grouping, measures used), method of analysis (descriptive statistics, statistical analyses used including missing data analyses), results related to presence and direction of effects. All information relevant to the outcome variables within the IMV model were collected. Specifically, data were sought for the following outcome variables: Defeat and humiliation, internal and external entrapment, suicidal/self-harm ideation (thoughts about harming oneself), suicidal behaviour including self-harm, non-suicidal, self-injury, parasuicide, or suicide attempts (any acts of intentionally harming oneself whether intent to die was present or not).
Studies and analyses were included in each synthesis if the evidence on the relevant association was being tested. Upon careful consideration, a narrative synthesis reported according to the PRISMA guidelines (Page et al., Citation2021) was deemed most appropriate for this review (See Appendix C & D for PRISMA Checklists). This was because the theoretical model under review is a comprehensive integrated model accounting for the role of a wide range of contextual factors, risk and protective factors, outcome variables, and moderators. Due to this nature of the model, studies testing the theory often test various aspects of it with a range of study designs and variables. The studies meeting the eligibility criteria also show large clinical and methodological heterogeneity arising from participants (various countries, populations, age groups), independent and dependant variables, measures, study designs, and moderators. Thus, the findings were narratively synthesised with a focus on the IMV model associations being tested.
Quality assessment
Quality Assessment was conducted using the National Institutes of Health (NIH4) tool for observational cohort and cross-sectional studies as well as the NIH tool for case–control studies by the first reviewer (National Institutes of Health, Citation2014). These quality assessment tools can be consistently applied to a range of different study designs and ask specific questions regarding the methodology of the study. The questions included in both tools also required little subjectivity to assess. These tools have the following possible ratings for each question (Yes, No, Not reported, Not applicable, and Can’t determine). The quality assessment tool for cross-sectional and cohort studies considered research aims, participant characteristics, sampling, time frame, characteristics and consistency of measures, blinding, attrition, statistical power, and confounding variables. For case–control studies, the quality assessment tool considered clarity of research aims, recruitment and participant characteristics, statistical power, sampling, measurement, use of concurrent controls, time frame and confounding variables. Studies were considered to account for relevant confounding variables if an adequate description of methods employed to select control variables was provided. The percentage of affirmative ratings was used to assess quality as follows (Maass et al., Citation2015): Poor (0%–24.99%), fair (25%–49.99%), good (50%–74.99%) or excellent (75%–100%).
Results
In order to aid readability, the references to the included studies are numbered in the results section (See Appendix A for the reference list of included studies). A total of 98 records (reporting 100 studies) with 138,365 (M = 1471.97; SD = 4332.06) participants were included in the current systematic review after accounting for overlap. As represented in , the included studies were primarily cross-sectional and conducted in the United Kingdom, Germany, and the United States of America. The location of data collection was not reported for four studies (Studies: 1, 2, 3, 4) and three studies were conducted online with international samples (Studies: 5, 6, 7). Nearly half the participants (45.45%) were recruited from the general population followed by university/college students (17%), hospitals (17%), school students (10%), and military (2%).
Table 1. Design, location, and sample characteristics of included studies.
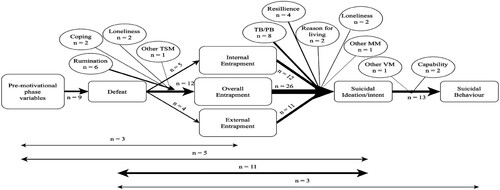
Only two studies tested all three phases of the IMV model (Studies: 7, 8) and one of these was a network analysis that included variables derived from the IMV model. The remaining included studies only tested specific aspects of the IMV model. illustrates the associations within the IMV model that were most frequently tested (Studies testing each pathway are outlined in Appendix E). These included studies testing multiple pathways of the model separately. However, this does not include studies investigating group differences as they were not testing these pathways within the model. Among studies testing longer pathways in the model, three studies investigated defeat as a mediator between pre-motivational phase variables and entrapment (Studies: 2, 9, 10). Five studies reported on defeat and entrapment as mediators between pre-motivational phase variables (impulsivity, stress, childhood trauma, nightmares, insomnia, and wellbeing) and suicidal ideation (Studies: 8, 11, 12, 13, 14). Eleven studies reported on entrapment (overall, internal, or external) as a mediator between defeat and suicidal ideation (9, 10, 15, 16, 17, 18, 19, 20, 21, 22, 23). Finally, three studies examined entrapment and suicidal ideation as mediators between defeat and suicidal behaviour (Studies: 24, 25, 26).
Figure 3. Frequency of IMV model pathways tested in included studies. Note. TSM = Threat-to-self moderators, TB = Thwarted Belongingness, PB = Perceived Burdensomeness, MM = Motivational moderators, VM = Volitional Moderators. This figure demonstrates the pathways in the IMV model that were investigated within the included studies. The thickness of the arrows represents the number of studies that tested the relevant association. Similarly, the arrows at the bottom represent the number of studies that tested pathways using mediation models. N provides the actual number of studies testing the pathway.
Evidence for associations between pre-motivational phase variables and motivational phase variables
Fourteen studies tested the association between pre-motivational variables and defeat (Studies: 2, 8, 9, 10, 11, 12, 13, 14a&b, 27, 28, 29, 30) or defeat/entrapment as one variable (Study: 7). Nine out of these studies were cross-sectional (64.29%), three were prospective studies (21.43%), and two were ecological momentary assessments (14.29%). A majority of these studies were conducted among students or the general population. illustrates the pre-motivational phase variables, mediators, and direction of effects for these variables.
Table 2. Relationship between pre-motivational variables and mediators and defeat.
Two studies investigated the role of childhood experiences and parenting on motivational phase variables. After controlling for depressive symptoms, one study found that the presence of parental care in the first 16 years of life was associated with lower defeat scores in a general population sample and this association was partially mediated by insecure attachment (Study: 9). They also reported that paternal overprotection was indirectly related to increased feelings of defeat through attachment avoidance while maternal overprotection was indirectly linked to defeat through attachment anxiety. Attachment anxiety and avoidance was subsequently associated with increased entrapment indirectly through defeat. In contrast, one study reported that childhood trauma was not significantly related to defeat among a group of men with alcohol use disorder (Study: 11). A network analysis of IMV model variables also found that physical, emotional, and sexual abuse trauma and value strain was indirectly positively associated with defeat/entrapment conceptualised as one variable through thwarted belongingness and coping strain was directly associated with defeat (Study: 7).
Various psychological factors were also related to motivational phase variables. For instance, higher psychological distress (Study: 27) and poorer sleep quality (Study: 14) was associated with higher feelings of defeat. In contrast, individuals reporting greater mental wellbeing were more likely to report lower suicidal ideation (Study: 8). This association was also mediated by defeat and internal and external entrapment. Self-compassion subscales (self-judgement and isolation) were positively linked to defeat cross-sectionally and prospectively (Study: 29). However, this effect did not remain significant in the prospective analysis after accounting for depressive symptoms. In contrast, the mindfulness subscale was cross-sectionally negatively associated with defeat. Finally, the self-kindness and common humanity subscales were not significantly associated with defeat. Additionally, variables including nightmares and insomnia (Studies: 12, 13, 14), and stress and impulsivity (Study: 11) were also associated with increased suicidal ideation through defeat and entrapment.
Studies have also demonstrated the role of social and personality factors as pre-motivational phase variables. Two studies reported that higher levels of perfectionism were linked to higher defeat scores and this effect was mediated by social comparison (Studies: 2, 10). Negative social comparison and rejection sensitivity were also positively related to increased feelings of defeat and subsequently entrapment. Furthermore, social comparison in the online context was also associated with defeat and mediated the effect of time on social media on defeat (Study: 2). This effect was further heightened in the presence of problematic social media use. A cross-sectional study also reported that workplace bullying was associated with greater feelings of defeat. This association was moderated by rumination. However, personality variables such as extraversion and conscientiousness were related to lower defeat scores while lower emotional stability was related to higher defeat (Study: 27). Finally, openness and agreeableness were not significantly associated with defeat.
Evidence for hypothesised associations within the motivational phase
Defeat-entrapment association
Sixteen studies examined the association between defeat and either entrapment or it’s subcomponents, internal and external entrapment (see Appendix F; Studies: 24, 26, 29, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43). Eleven of these studies were cross-sectional in design (68.75%), while the remaining were cohort (n = 3, 18.75%) and ecological momentary assessment (n = 2, 12.50%). Among these, twelve studies investigated the relationship between defeat and overall entrapment among 5,021 participants (M = 418.42, SD = 348.64). All studies reported that higher defeat was significantly associated with higher entrapment in the cross-sectional analyses in both univariate and multivariate analyses (Studies: 26, 29, 31, 32, 33, 34, 35, 36, 37, 38, 41). One study further reported that baseline defeat prospectively predicted entrapment over 2.5 months (Study: 29). However, an ecological momentary assessment study over 7 days reported that defeat did not prospectively predict entrapment when accounting for autocorrelative effects (Study: 32) while another found bidirectional effects between defeat and entrapment at 3 h but not 6, 9, or 12 h (Study: 42).
Five studies examined the relationship between defeat and internal or external entrapment. Two cross-sectional studies (Study: 24, 38) reported that defeat was significantly associated with both internal and external entrapment. Similarly, defeat was directly connected to internal and external entrapment in a network analysis (Study: 43). A 1-year cohort study also reported that defeat was associated with internal and external entrapment and change in internal and external entrapment cross-sectionally among a sample of inpatients admitted to a psychiatric ward following a suicide attempt or suicidal crisis (Study: 39). However, defeat also prospectively predicted change in internal entrapment but not internal/external entrapment or change in external entrapment. One study did not report results on external entrapment and overall entrapment due to non-significant findings but reported a positive association between defeat and internal entrapment in cross-sectional analyses when rumination and problem-solving were accounted for (Study: 40).
Threat-to-self moderators. Threat-to-self moderators are variables that may enhance or buffer the relationship between defeat and entrapment. A number of variables were investigated as threat-to-self moderators. The findings are presented below.
Rumination. Investigations of the influence of rumination on the relationship between defeat and entrapment yielded mixed results. Six studies tested rumination as a moderator between defeat and entrapment among adolescent and adult students, general population, and prison populations (Studies: 20, 21, 24, 26, 34, 40). Among these, two studies found that the association between defeat and overall entrapment was stronger among individuals scoring higher in rumination (Studies: 24, 34) while another reported that brooding but not the reflection components of rumination strengthened the defeat-entrapment relationship (Study: 20). The remaining studies did not report a significant influence of rumination (brooding or reflection) on the relationship between defeat and entrapment or internal entrapment (Studies: 21, 26, 40).
Coping. There was limited evidence for the role of coping as a threat-to-self moderator. Two cross-sectional studies investigated the role of maladaptive coping (Study: 9) and coping flexibility (Study: 34) on the relationship between defeat and entrapment. Maladaptive coping was not found to significantly affect the defeat-entrapment relationship (Study: 9) while coping flexibility significantly buffered this relationship.
Loneliness. Two studies investigated the effects of loneliness on the defeat-entrapment relationship and found mixed results. One study reported that loneliness strengthened the relationship between defeat and entrapment (Study: 31) while another found that loneliness and its sub-facets (global, romantic, social or family) did not moderate this relationship (Study: 41).
Other moderators. The effects of a wide range of other variables on the defeat-entrapment relationship were also investigated. None of the moderators in this section were included in more than one study, limiting the ability to draw conclusions. Among these, resilience (Study: 10), experiential avoidance (Study: 35), and rational problem solving (Study: 40) moderated the defeat-entrapment association. In these models, rational problem-solving and experiential avoidance (tendency to avoid internal experiences) strengthened these associations while resilience was protective against entrapment in the presence of defeat. Other variables including desire for control sub-facets – leadership and destiny control (Study: 33), gender role conflict and androgyny (Study: 34), race-based rejection sensitivity (Study: 16), problem-solving variables (positive, negative, impulsive-careless, avoidance style; Study: 40) and post-traumatic growth (Study: 37) did not affect the defeat-entrapment relationship. Finally, one study reported that a variable comprised of items from threat-to-self moderator scales including rumination, catastrophising, self-blame, and other-blame weakened the relationship between defeat and entrapment (Study: 22).
Entrapment-suicidal ideation association
Thirty-three papers aimed to investigate the relationship between entrapment or its subcomponents and suicidal ideation (See Appendix G). These studies included data from 24, 244 participants (M = 738.06, SD = 775.88). Twenty-four (72.73%) out of these studies were cross-sectional, eight (24.24%) were prospective analyses, and one was an ecological momentary assessment (3.03%). The association between overall entrapment and suicidal ideation was investigated by twenty-three studies among 13,020 participants (M = 542.5, SD = 383.93; Studies: 17, 18, 23, 26, 29, 30, 31, 33, 36, 37, 38, 42, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54). Eighteen of these studies reported a positive association between entrapment and suicidal ideation among 9,143 participants from the student, clinical, military, and the general populations while controlling for a range of suicide risk factors (M = 507.94, SD = 347.60; Studies: 17, 18, 23, 26, 29, 30, 37, 38, 42, 46, 47, 48, 49, 50, 51, 53, 54, 55). Four cross-sectional studies (2,463 participants, M = 615.75, SD = 511.20) from the general population (Studies: 31, 33, 36, 52) reported that overall entrapment was not significantly related to suicidal ideation in multivariate analyses. Two studies showed mixed results. One reported that entrapment was cross-sectionally linked to suicidal ideation in female students but not males while controlling for demographic variables (Study: 45). Entrapment also prospectively predicted suicidal intent but not ideation among a sample of students (Study: 44).
Eleven studies reported on the sub-facets of entrapment and suicidal ideation (Studies: 1, 14, 15, 17, 24, 38, 39, 40, 43, 56, 57). Both internal and external entrapment were significantly related to suicidal ideation in five cross-sectional studies in 1,780 participants among students, general, clinical and prison populations (M = 356, SD = 281.43; Studies: 1, 17, 24, 30, 38, 55, 56). The remaining studies indicated that internal but not external entrapment were associated with suicidal ideation cross-sectionally among 9,468 participants (M = 1,893.60; SD = 1388.48) from general, military, student and clinical samples (Studies: 40, 43, 57) and prospectively (Studies: 14, 15, 39). In addition, one of these reported that internal but not external entrapment was associated with an increase in suicidal ideation cross-sectionally but a decrease prospectively when accounting for defeat as participants scored lower on all IMV model variables over the course of the study (Study: 39). Four studies further investigated the predictive ability of defeat/entrapment characterised as one variable among the general population and students (Studies: 7, 58, 59, 60). One of these reported that defeat/entrapment predicted suicidal ideation at three months but not six months follow up and this effect was non-significant after controlling for depressive symptoms (Study: 60). The remainder reported that defeat/entrapment was cross-sectionally associated with suicidal ideation. Finally, based on a network analysis of qualitative data from online posts, one study reported that defeat/entrapment was not directly linked to suicide plans in the network (Study: 7).
Motivational moderators. Motivational moderators are hypothesised to influence the relationship between entrapment and suicidal ideation. The findings with relation to motivational moderators are presented below.
Thwarted belongingness (TB2). TB alone was generally not found to enhance or buffer the relationship between entrapment and suicidal ideation. Four studies examined thwarted belongingness as a moderator of the entrapment-suicidal ideation relationship. TB was found to enhance the entrapment-suicidal ideation relationship in two of these (Studies: 26, 47). However, one of these only found a significant effect after including the three-way interaction effect between Entrapment, Perceived Burdensomeness, and TB (Study: 47). The remaining studies did not report a significant effect (Studies: 15, 46).
Perceived burdensomeness (PB3). The included studies generally supported the effects of PB on the entrapment-suicidal ideation relationship. Seven studies investigated the moderating role of perceived burdensomeness on Entrapment-SI (Studies: 15, 17, 21, 24, 26, 46, 47). Four of these reported that perceived burdensomeness enhanced the relationship between entrapment and suicidal ideation (Studies: 21, 26, 47) and internal entrapment (Study: 24). Interestingly, one of these reported that perceived burdensomeness weakened the relationship between entrapment and suicidal ideation among a sample of African American students (Study: 21). Furthermore, two studies reported significant three-way interactions between TB, PB and entrapment with suicidal ideation as outcome. One study reported that TB*PB strengthened this association (Study: 47) while the other found that it decreased the effect of entrapment on suicidal ideation (Study: 17). This three-way interaction remained significant for internal and external entrapment as well (Study: 17). Finally, one study conceptualised interpersonal variables (TB and PB) as a single variable and reported that it increased the effect of entrapment on suicidal ideation (Study: 22).
Resilience. The role of resilience as a motivational moderator in the IMV model was supported by the evidence. The effect of resilience on the relationship between entrapment/internal entrapment and suicidal ideation was examined by four studies (Studies: 9, 10, 24, 26). All 4 of these studies found that resilience was protective against suicidal ideation in the presence of entrapment.
Reasons for living. Studies reporting on the moderating role of reasons for living found promising results. The results of two studies that included reasons for living as a motivational moderator indicated a significant attenuating effect of reasons for living with overall entrapment (Study: 50) and internalised and externalised entrapment (Study: 1). This paper further reported that presence of life meaning influenced the effects of both internalised and externalised entrapment on suicide, and the three-way interactions of both internal and external entrapment with ReasonsForLiving*PresenceOfLifeMeaning and ReasonsForLiving*SearchforLifeMeaning were significantly associated with suicidal ideation.
Loneliness. Two studies investigated loneliness as a motivational moderator in the entrapment-suicidal ideation relationship. Both studies found that individuals with higher entrapment and higher loneliness were likely to have higher suicidal ideation scores (Studies: 31, 41). Additionally, one of these reported that this was only true for family, romantic, and global loneliness but not social loneliness (Study: 41).
Other moderators. Various other potential moderators were identified as motivational moderators. As with threat-to-self moderators, the variables included in different studies were diverse. Individuals with high entrapment were more likely to report suicidal ideation in the presence of higher psychological pain (Study: 23, 48), and attitude to suicide i.e., feeling like suicide is an option for them (Study: 24). Alternatively, individuals with high entrapment were less likely to report suicidal ideation if they reported goal re-engagement (Study: 40), positive mental health, overall positive wellbeing, and the positive wellbeing subfacet – self-acceptance (Study: 61), better sleep quality (Study: 62), hope (Study: 20), and desire for control subscale – decision avoidance (Study: 33). Positive wellbeing sub-facets (autonomy, environmental mastery, personal growth, positive relations, and purpose in life; Study: 61), sub-facets of desire for control (destiny control and leadership; Study: 33), race-based rejection sensitivity (Study: 16), Rumination, post-traumatic growth (Study: 37) and wellbeing (Study: 8) did not moderate this relationship. Additionally, fearlessness about death increased the relationship between internal and external entrapment and self-rated likelihood of attempt but not past month suicidal ideation or plan (Study: 57). Furthermore, a study among sexual minority adults found that family belongingness but not belongingness with sexual minority friends or community or straight friends buffered the relationship between entrapment and suicidal ideation (Study: 49).
When defeat/entrapment was conceptualised as one variable, ethnic identity subfacet – exploration and commitment (Study: 58) buffered the effect of defeat/entrapment on suicidal ideation while positive future thinking (Study: 60) strengthened it. However, the subfacets of ethnic identity (belonging and affirmation) did not moderate this relationship. Further, positive future thinking moderated this relationship at three months follow up but not at baseline or six months.
Entrapment as mediator between defeat and suicidal ideation
Eleven studies investigated the indirect effects of defeat on suicidal ideation through overall entrapment (See Appendix H). Five of these reported a significant mediating role of entrapment in the cross-sectional analyses among 1,919 participants (M = 383.80, SD = 151.36) from the general population, student, and clinical samples between defeat and suicidal ideation after accounting for a range of variables including depressive symptoms, racial rejection sensitivity, and demographic characteristics (Studies: 9, 10, 16, 17, 18). One study did not find a significant effect cross-sectionally or prospectively (23). Two studies also reported that entrapment mediated the relationship between defeat and suicidal ideation prospectively at 1 and 4 months respectively among participants from general and clinical populations (Studies: 18, 19). However, one of these did not find this effect at 6-month follow-up (Study: 18). Three studies reported that defeat was positively linked to entrapment cross-sectionally but the association between entrapment and suicidal ideation was not significant in the general population and university students (Studies: 20, 21, 22). No trends were observed across studies with relation to the inclusion of additional covariates in these models.
Additionally, three studies operationalised entrapment into internal/external entrapment. Internal entrapment was found to mediate the relationship between defeat and suicidal ideation in two of these among 2,758 participants both cross-sectionally (Study: 17) and prospectively over 4 and 12 months upon accounting for depression and other variables (Studies: 15, 19). Only one study found that external entrapment mediated the relationship between defeat and entrapment cross-sectionally (Study: 17).
Evidence for hypothesised associations within the volitional phase
Suicidal ideation-suicidal behaviour association
Twelve studies investigated the relationship between suicidal ideation and behaviour among 13,324 participants (M = 1332.4, SD = 2414.06; See Appendix I). Nine reported a positive association between suicidal ideation or plan and behaviour in the cross sectional (Studies: 24, 26, 59, 63, 64) and prospective analyses (Studies: 5, 6, 65, 66). One of these reported that detailed suicide plan and past week plan were univariately associated with suicidal behaviour while plan involving methods and lifetime plan were not (Study: 5). Additionally, one study reported that suicidal ideation was predictive of suicidal behaviour during a four-year follow up in the univariate but not multivariate analyses (Study: 67). Two network analyses investigated the relationship between duration and frequency of suicidal ideation or plans on suicidal behaviour. One of these investigated this association over 15 months (Study: 68) while the other qualitatively coded online posts based on themes associated with IMV model variables (Study: 7). The resulting networks indicated that these independent variables were not directly linked to suicidal behaviour.
Volitional moderators. Volitional moderators are variables that facilitate the transition from suicidal ideation to behaviour. This section presents findings of studies investigating volitional phase variables.
Acquired Capability. Acquired capability, consisting of fearlessness about death and pain tolerance were not supported by the included studies as volitional moderators. Two studies reported the role of acquired capability in the transition from suicidal ideation to behaviour. Both fear of dying and pain tolerance did not significantly influence the suicidal ideation-attempts relationship cross-sectionally (Study: 26), or prospectively (Study: 6).
Exposure to suicide. One study reported the role of exposure to suicide in facilitating the transition from suicidal ideation to behaviour. Exposure variables including familial suicide attempts, number of familial attempts, non-familial attempts, number of non-familial suicide attempts were also not found to influence the suicidal ideation-attempts relationship (Study: 68).
Other moderators. One study reported that disinhibition enhanced the relationship between suicidal thoughts and behaviours while academic grades buffered the relationship between suicidal thoughts and behaviour (Study: 64).
Evidence for the central pathway of the IMV model
Three studies also investigated the relationship between defeat and suicidal behaviour with entrapment and suicidal ideation as mediators in schools, universities, and prisons. Two of these studies reported that entrapment and suicidal ideation mediated the relationship between defeat and suicidal behaviour among 3,048 participants (Studies: 25, 26). The remaining study found that internal but not external entrapment and suicidal ideation mediated this association after controlling for hopelessness (Study: 24).
Case–control studies investigating group differences based on suicide-related outcome group
Thirty-six studies investigated a range of theoretically relevant variables in distinguishing between individuals reporting no suicidal ideation or behaviour (control group), suicidal ideation but not behaviour (ideation group), and the presence of suicidal behaviour (enactment group). Based on the hypotheses of the IMV model, it is expected that pre-motivational and motivational phase variables would differentiate between control and ideation groups while volitional phase variables would differentiate between ideation and enactment groups. Given the wide range of variables, their sub-facets investigated, and the heterogeneity in conceptualising and measuring these, only findings relevant to the variables explicitly described by the IMV model are discussed here. Additionally, the findings presented here are focussed on the group differences based on the predictions of the IMV model. More specifically, differences between control and ideation groups in pre-motivational and motivational phase variables are presented and differences between ideation and enactment groups in volitional phase variables are presented. The findings are synthesised based on whether the analysis was univariate (examining differences in one variable) or multivariate (examining differences in one construct while accounting for other IMV model variables) and the timeframe (cross-sectional or prospective). However, the full table of results alongside information about statistical analyses and controlled variables for all model comparisons and analyses is presented in Appendix N.
Premotivational phase variables
Socially Prescribed Perfectionism. Two cross-sectional studies investigating whether socially prescribed perfectionism differentiated between control, ideation, and enactment groups reported that individuals in the control group reported lower perfectionism compared to the ideation and enactment groups in univariate analyses (Study: 18, 70). However, the individuals in the ideation and enactment groups did not differ in perfectionism scores.
Childhood adversity. Overall adversity was significantly higher in the enactment compared to the ideation group in multivariate analyses in a cross-sectional study controlling for demographic and health-related factors (Study: 71) but not in a univariate prospective study (Study: 72). Emotional abuse, physical abuse, and physical neglect were higher in the enactment compared to the ideation group in the cross-sectional multivariate analyses accounting for other forms of childhood abuse (Study: 4) However, emotional neglect and sexual abuse did not significantly differentiate these groups. A longitudinal study also reported that sexual abuse did not differentiate between the ideation and enactment groups (Study: 73). This study also reported that individuals from the control group were less likely to report experiencing bullying and household cruelty compared to ideation and enactment groups while controlling for sex and socioeconomic status (Study: 73).
Motivational phase variables
Defeat/humiliation. Eight out of nine studies found that individuals in the ideation group were more likely to report defeat compared to the control group in cross-sectional univariate analyses (Study: 18, 29, 23, 60, 74, 75, 76, 77a). Findings were mixed in the multivariate analyses where multiple suicide risk factors were compared in a single analysis. Specifically, two out of four studies found that the control group scored lower in defeat than the ideation group accounting for a range of motivational and volitional phase variables (Study: 74, 76). However, study 74 only found a significant difference after including volitional phase variables in the model.
Two studies out of three also reported that defeat was lower in the ideation compared to the control groups prospectively over several weeks in the univariate analyses accounting for baseline suicidal ideation (Study: 23, 29). This difference was non-significant in the multivariate analysis with baseline suicidal ideation, depressive symptoms, self-compassion, mindfulness stress, and resilience in the model (Study: 29). One study did not report any differences in defeat between control and ideation groups both cross-sectionally or prospectively (Study:79). Only two studies reported that defeat was higher in the enactment groups compared to the ideation group in the cross-sectional univariate analyses. This effect was not significant in the multivariate analyses after including demographic variables and motivational and volitional variables in the IMV model (Study: 74, 76). Studies examining humiliation reported that humiliation did not differentiate the control and ideation groups or ideation and enactment groups in cross-sectional univariate analyses (Study: 77a, 78).
Entrapment. Seven out of ten studies reported that individuals in the control group reported lower overall entrapment than the ideation group cross-sectionally (Study: 23, 29, 60, 74, 75, 76, 79). Among five studies that conducted multivariate analyses, only two of these were significant (Study: 29, 74). Specifically, study 29 reported that the control group reported lower entrapment than the ideation group after accounting for depressive symptoms, sexual orientation, self-compassion and self-criticism, defeat, and mindfulness and resilience. Study 74 also reported that the control group had lower entrapment after accounting for mood variables, demographic variables, and a range of motivational and volitional risk factors. Three studies that examined these differences prospectively reported mixed results. Specifically, one of these reported that entrapment was significantly lower in the control group in the univariate analyses (Study: 23, 29) while the other reported no significant differences (79). This difference did not remain significant in the multivariate analyses after controlling for baseline suicidal ideation, depressive symptoms, defeat, stress, and self-compassion and self-criticism, mindfulness, and resilience (29).
Additionally, two out of three studies reported that internal and external entrapment were higher in the ideation compared to the control groups in the univariate cross-sectional (Study: 18, 29) and prospective analyses (Study: 29). Study 77a did not report any differences. Additionally, both internal and external entrapment did not differentiate the ideation and enactment groups.
Rumination. Two cross-sectional studies reported that rumination was higher in the ideation compared to the control group in the univariate analyses (Study: 70, 74) while one study reported no differences (Study: 80). This difference remained significant in study 74 in multivariate analyses after accounting for a range of motivational and volitional phase variables. Rumination was also higher in the enactment group in two out of three studies (Study: 74, 80). This difference was not significant in the multivariate analyses in study 74.
Coping. One study reported that maladaptive but not adaptive coping was higher in the ideation group cross-sectionally in the univariate and multivariate analyses but not prospectively over 6 months (Study: 79). This was after accounting for demographic, mood, and other motivational/volitional phase variables. Both adaptive and maladaptive coping did not differentiate the ideation and enactment groups. Two studies investigated further sub-facets of coping including active, avoidant, passive, problem-focussed, and emotion-focussed coping (Study: 81, 82).
Study 81 reported that in the sexual minority population, active coping was significantly higher in the control group compared to the ideation group, but this difference did not remain significant after including passive coping in the model. However, active coping remained significant when examining past-year ideation only. Similarly, in the gender minority group, active coping was only significantly higher in the control group than in the ideation group before including avoidant and passive coping. However, for past-year suicidal ideation, active coping in this sample was significantly higher after including avoidant coping but reduced to non-significance after including passive coping. In terms of avoidant coping, the control group reported lower avoidant coping than those reporting lifetime and past-year suicidal ideation in the sexual minority population. The control group also scored lower than the ideation group in avoidant coping in the gender minority population, only while accounting for past year ideation.
After including passive coping in the models, the ideation group in the sexual minority sample reported higher avoidant coping than the control group for lifetime ideation but no significant differences when compared to past year ideation. There were no significant differences in the gender minority population. In contrast, study 82 found that avoidant coping was higher in the ideation group in the univariate and multivariate analyses which accounted for demographic factors, interpersonal factors, coping factors, and resilience. In terms of passive coping, study 81 reported that passive coping was higher in the ideation compared to the control groups for both sexual and gender minority samples after the inclusion of avoidant and active coping. Finally, emotion-focussed coping but not problem focussed coping was significantly higher in the ideation group compared to the control group in both univariate and multivariate analyses (Study: 82).
Social support. Four out of six cross-sectional studies reported that individuals in the control groups reported higher social support than those in the ideation group (Study: 18, 76, 83, 84) while one reported that the ideation group scored higher (Study: 80) in the univariate analyses. Additionally, two of three studies also reported that the control group scored higher than the ideation group in multivariate analyses (Study: 84, 85). Here, study 84 accounted for variables including demographics, life events, alcohol or substance use, social support, wish to live, sleep quantity, aggression, and prior self-harm. This difference remained significant in the prospective multivariate analyses over 2 years upon accounting for demographic variables, mood, past ideation and behaviour, and exposure to suicidal behaviour (Study: 85).
Two studies also examined sub-facets of social support including family support, friend support, and significant other support. In the univariate cross-sectional analyses, family support was significantly higher in the control groups (79, 82). However, only one of these reported that friend and significant other support was significantly higher in the control group (82). These differences were not significant in the multivariate analyses upon accounting for demographic, interpersonal and motivational phase variables. None of these differences were significant in the prospective analyses.
Goal disengagement and re-engagement. Additionally, two cross-sectional studies examined differences in both goal disengagement and re-engagement among the control and ideation groups, in the univariate analyses (Study: 74, 76). Both studies found that goal disengagement was lower in the control group compared to the ideation group, but the ideation and enactment groups did not differ. Interestingly, study 74 reported that goal reengagement was highest in the control followed by the ideation and enactment groups, while study 76 reported that goal reengagement was the highest in the enactment group followed by the ideation and control groups. These differences were not significant in the multivariate analyses accounting for motivational and volitional phase variables (74, 76).
Burdensomeness and belongingness. Three cross-sectional studies examined group differences TB and PB between control and ideation groups. In the univariate analyses, PB was significantly lower in the control group compared to the ideation group in all studies (18, 74, 76). Two of these conducted multivariate analyses accounting for a range of motivational and volitional variables (74, 76). The results indicated that PB was significantly lower in the control group compared to the ideation group in both studies. With regard to TB, two studies found that control groups scored lower in belongingness in the univariate analyses (Study: 18, 76) while one study reported that control groups scored higher (Study: 74). Among the two studies that conducted multivariate analyses accounting for other motivational and volitional phase variables, one found that TB was higher in the control group while the other reported no differences (Study: 74, 76)
Resilience. Six out of seven studies comparing resilience among control and ideation groups reported that resilience was higher in the control group both cross-sectionally (Study: 18, 29, 76, 82, 86, 87) and prospectively (Study: 29). Two of the three studies that conducted cross-sectional multivariate analyses reported that resilience differentiated the control and ideation groups. One of these found that resilience was higher in the control group after accounting for demographic, interpersonal, and coping factors (82). The other study reported that resilience was higher in the control group after accounting for demographic, interpersonal, and self-compassion/criticism, mindfulness, resilience, and other motivational phase variables (29). The third study did not find significant differences between the groups (76). Additionally, one study examining the sub-facets of resilience reported that emotional control, family support, and interpersonal assistance but not goal focus or positive cognition were higher in the control group in the cross-sectional univariate analyses (86).
Norms. In terms of stigmatisation and norms, one study examining sub-facets of suicide stigmatisation (stigmatisation, isolation/depression, glorification/normalisation) reported largely no significant differences between control and ideation groups (79). However, glorification/normalisation alone was significantly higher in the ideation compared to the control group in the prospective multivariate analyses accounting for social support, stigmatisation, and baseline suicidal ideation. Additionally, a study on norms reported that the ideation and enactment groups were more likely to believe that their peers engaged in suicidal behaviour compared to the control group (70).
Volitional phase variables
Impulsivity. Consistent with the IMV model’s predictions, five cross-sectional studies reported that impulsivity was higher in the enactment group compared to the ideation group in the univariate analyses (Study: 18, 70, 74, 76, 77a). Three of these further reported that the differences remained significant in the multivariate analyses where two of these accounted for motivational and volitional variables (Study: 74, 76) and the remaining study accounted for social modelling of suicide (77a).
Of the three prospective studies investigating group differences in impulsivity using univariate analyses, only one reported that the enactment group scored higher in impulsivity compared to the ideation group over 6 years (Study: 73). A range of sub-facets of impulsivity were also compared between the ideation and enactment groups (Study: 83, 89, 90). This included response inhibition, positive urgency, negative urgency, and behavioural measures of impulsivity. Negative urgency was higher in the enactment group compared to the ideation group in univariate analyses in two out of three studies (83, 89). One of these further reported that the enactment group scored higher in negative urgency in the multivariate analyses controlling for demographic variables, alcohol-related volitional factors, and self-harm (83). One study further reported that lack of premeditation and lack of perseverance but not positive urgency were significantly higher in the enactment group compared to the ideation group in univariate cross-sectional analyses (90). This study further examined group differences in behavioural measures of impulsivity in but did not find any significant differences.
Acquired Capability for Suicide. Two out of three cross-sectional studies reported that the acquired capability of suicide was higher in the enactment group compared to the ideation group in the univariate analyses (Study: 18, 76). Study 76 further conducted multivariate analyses upon controlling for a range of motivational and volitional phase variables outlined by the IMV model and reported that the differences remained significant. Additionally, of the three cross-sectional studies investigating fearlessness about death, only one reported that the enactment group scored significantly higher than the ideation group in both univariate and multivariate analyses which accounted for motivational and volitional phase variables (Study: 74). Six studies compared differences in pain or discomfort tolerance among individuals reporting suicidal ideation and enactment using a range of measures including self-report questionnaires, algometer, cold and heat pressors, etc. (Study: 3, 74, 77a&c, 80, 91). Self-report measures largely showed mixed results with emotional pain sensitivity and physical pain distress being higher in the enactment group in univariate analyses (Study: 77c, 91). However, overall discomfort tolerance did not differentiate between the groups (74, 80). Among the behavioural measures, pain tolerance tasks generally showed non-significant results except for a cold pressor task (3) and physical pain tolerance under stress (77a).
Exposure to suicide. For overall exposure to suicide, enactment group reported higher exposure to suicide cross-sectionally compared to ideation group in four studies (Study: 18, 73, 76, 77a) while one reported no differences (Study: 79) in the univariate analyses. However, study 77a did not find significant differences in a subset of the original sample that were invited to the laboratory portion of the study. One out of two studies also reported that enactment was significantly higher in the multivariate analyses accounting for impulsivity (77a). However, no differences were found prospectively in both univariate (79) and multivariate analyses (69).
In terms of types of exposure, four out of five studies reported that individuals in the enactment group were more likely to report exposure to family suicidal behaviour compared to the ideation group in the cross-sectional univariate analyses (Study: 70, 73, 76, 79). However, studies investigating exposure to family behaviour in multivariate models accounting for a range of variables including past behaviour, motivational/volitional phase variables, life events, aggression, loneliness and other variables (Study: 74, 76, 84, 85) generally reported no significant differences with the exception of one study that found higher exposure in the enactment group (74). Additionally, prospective investigations of these studies also resulted in non-significant differences (Study: 72, 73, 79, 85). Finally, three cross-sectional studies reported that the enactment group reported higher exposure to friend suicidal behaviour in the univariate analyses (Study: 70, 73, 76), while one study reported no differences (Study: 79). Two studies also reported significant differences in multivariate analyses accounting for a range of motivational and volitional phase variables (Study: 74, 76), while one reported no differences (Study: 85). These findings were not significant prospectively (Study: 72, 79, 85).
Past self-harm. Two cross-sectional studies compared differences in self-harm and non-suicidal self-injury between individuals that thought about suicide and attempted suicide. One of these reported that self-harm while in prison was higher in the suicide attempt group (Study: 84), but only in the univariate analysis before adding variables including demographics, life events, aggression, substance abuse, wish to live, self-harm, sleep quantity, and aggression. The other study found that the presence of non-suicidal self-injury did not differentiate the groups. However, having more than five episodes was of self-harm was associated with past-year suicide attempts after accounting for hopelessness, prior self-harm, emotional regulation, borderline symptoms, and purpose in life (Study: 92). Among prospective studies, two studies reported that the presence of lifetime suicide was associated with suicide attempts prospectively over 6 weeks and 2 years respectively (Study: 85, 88). These findings were significant in the multivariate analyses as well, which accounted for clinical variables (e.g., treatment medication), mental & mood disorder symptoms, and insomnia. However, study 88 reported that the number of attempts did not predict the occurrence of suicide attempts during the 6-week follow-up period.
Mental Imagery. One cross-sectional study compared the group differences in mental imagery and found that mental imagery about suicide was higher in the ideation group compared to the control and enactment group compared to ideation in the univariate analyses (Study: 76). These effects remained significant in the multivariate analyses after accounting for other motivational and volitional phase variables. Another study reported that the ideation group alone reported suicidal flash-forwards compared to the control group. However, this was not compared between ideation and enactment groups (Study: 23).
Quality assessment and publication bias
Cross-sectional/Cohort studies. Sixty-seven of the included studies were included in this analysis. Four papers were rated excellent (n = 4, 5.97%) and nearly half were rated good quality (n = 33, 49.25%). The rest were fair (n = 25, 37.31%), and poor (n = 5; 7.46%). The decisions for each judgement according to the NIH quality assessment tool for observational cohort and cross-sectional studies are provided in Appendices J and K. Quality ratings were generally similar for studies investigating different pathways within the IMV model compared to studies testing single associations. Over half the studies testing longer pathways of the model were rated good (n = 10; 52.63%), and the remaining were rated fair (n = 6; 31.58%), and poor (n = 3; 15.79%). The study that investigated all three phases of the IMV model was also rated good (Study: 8). Among studies testing single associations of IMV model variables, ratings were excellent (n = 4; 8.33%), good (n = 23; 47.92%), fair (n = 19; 39.58%), and poor (n = 2; 4.17%). The reasons for lower quality ratings were primarily due to lack of blinding due to self-report instruments, low follow-up rates/cross-sectional design, participation rate not being reported, unclear approach for selecting confounding variables, and not measuring predictor variables more than once.
Case–control Studies. Of the thirty-three case–control studies, one study was rated excellent (n = 1, 3.03%), over half were rated good (n = 17, 51.52%), followed by those rated fair (n = 15, 45.45%). Decisions for each judgement based on the NIH tool for case–control studies are presented in Appendices L and M. Reasons for lower quality ratings were lack of blinding due to self-report measures, not using concurrent controls, non-random sampling, retrospective design, no justification for approach to selection of confounding factors, and non-reporting of power analysis or sample size justification.
Discussion
Main findings
The current review systematically selected, synthesised, and reviewed the evidence for the predictions of the integrated motivational-volitional model of suicide. The included studies generally tested different parts of the IMV model compared to the whole model. Only two investigated all three phases of the model, however, the entire pathway was not investigated in the same model. In addition to this, studies that investigated the motivational and volitional phase (i.e., the defeat-entrapment-suicidal ideation-suicidal behaviour pathway) and the pre-motivational and motivational phase also found support for the hypotheses of the IMV model.
Consistent with the IMV model, the results support the role of psychological, social, personality, and parental factors in conferring vulnerability to defeat. Specifically, specific pre-motivational phase variables (including past parenting, insecure attachment, and perfectionism) were found to be associated with defeat and entrapment within the included studies. These results are consistent with the summary provided by Zortea et al. (Citation2021a) which also found support for the association between pre-motivational variables and suicide risk overall. Variables like adverse childhood experiences, insecure attachment, and perfectionism have also displayed strong associations with suicide risk in other reviews (Angelakis et al., Citation2019; Angelakis et al., Citation2020; O’Connor, Citation2007; Zortea et al., Citation2021b). However, due to limited overlap between the variables included across studies, it is not possible to draw conclusive results on the effects of specific variables. Studies conducted in specific populations also raised concerns regarding generalizability to other populations (e.g., Hong & Shin, Citation2021). Furthermore, the mechanisms by which these variables increase feelings of defeat are also unclear. As such, evidence on the pre-motivational phase remains largely inconclusive.
The motivational phase of the IMV model was the most widely investigated. The results overwhelmingly supported the proposed defeat-entrapment-suicidal ideation pathway consistent with the IMV model in the cross-sectional analyses. Interestingly, although the IMV model proposes defeat and humiliation as predictors of entrapment, none of the included studies investigated the role of humiliation within the IMV model. Results also generally indicated that total entrapment and internal entrapment were found to significantly mediate the relationship between defeat and suicidal ideation. The results for external entrapment were largely not significant. These results are consistent with other literature and reviews discussing the IMV model (Barzilay & Apter, Citation2014; Klonsky et al., Citation2017, Citation2018; Zortea et al., Citation2021a).
A wide range of threat-to-self and motivational moderators were also tested within the included studies. The findings on the effects of threat-to-self moderators on the association between defeat and entrapment were largely inconclusive. However, motivational moderators including resilience (Branley-Bell et al., Citation2019; Cleare, Citation2019; Wetherall et al., Citation2018), PB, and its interaction with TB (Hollingsworth, Citation2012; Li et al., Citation2021; Lucht et al., Citation2020; Ordóñez-Carrasco et al., Citation2020a, Scowcroft, Citation2019) found support as a motivational moderator in multiple studies. There was little overlap between other stage-specific moderators being tested resulting in inconclusive findings. Thus, examining the role of the moderators with the central pathway would be useful to present a clearer understanding of the suicidal process.
With regard to the volitional phase, the included studies presented mixed results. While suicidal ideation was generally associated with suicidal behaviour, the evidence for the prospective association between these variables was limited. A small number of studies examined specific volitional moderators and reported non-significant findings. As with threat-to-self and motivational moderators, there was limited overlap in the moderators studied. Thus, it is not possible to draw conclusions from the literature.
In terms of study characteristics, studies whose findings were consistent with the IMV model were generally cross-sectional. Prospective analyses yielded mixed results. As a majority of included studies were cross-sectional, it was not possible to determine if the time period between measurements impacted the results. Studies that found support for the IMV model also recruited participants from different populations including general, student, and clinical samples. Additionally, studies that investigated different pathways within the model (i.e mediation) also found support for the model. Finally, the included analyses accounted for a wide range of demographic and psychosocial variables. However, there were no clear trends observed when comparing univariate and multivariate analyses.
With regard to studies comparing control, ideation and enactment groups, the included studies investigated group differences in a large set of variables at different stages of the IMV model. As a result, there was limited overlap in the variables investigated and differences in the conceptualisation and measurement of these variables. Among variables outlined by the IMV model, some evidence suggested that pre-motivational and motivational variables, including perfectionism, defeat, entrapment, rumination, social support, goal disengagement, goal re-engagement and resilience, may differentiate the control and ideation groups. However, these findings were not observed in multivariate and prospective analyses. Similarly, volitional phase variables including impulsivity, acquired capability, and exposure to suicide may be higher in enactment groups compared to ideation groups, but findings were mixed in multivariate or prospective analyses. Thus, the limited overlap in the variables measured and the heterogeneity in conceptualisation, measurement, control variables, analysis, and time frames limit our ability to draw conclusions. These results contrast with review literature on theories of suicide that supported the role of the motivational and volitional phase moderators (Stanley et al., Citation2016; Wetherall et al., Citation2020). It is possible that this may be due to prior reviews reporting on a limited number of studies or on studies conducted prior to the introduction of the IMV model. Further clarity on this is required in order to appropriately inform intervention strategies.
Directions for future research
The findings of the current review generally support the main assumptions of the IMV model. The findings indicated that certain aspects of the IMV model (e.g., the central pathway) are abundantly examined within the literature while other areas are less empirically evidenced. However, the current review identified several directions for future research based on the gaps in the current literature. Firstly, few studies conducted aimed to test all aspects of the model within the same analysis. Testing different phases of the model together would be useful in determining if there are specific combinations of predictors or ‘risk trajectories’ from different areas of the model that may significantly increase suicide risk (O’Connor & Kirtley, Citation2018). While this is understandable considering the methodological challenges of incorporating a complex model, it is important that wherever possible, future research aim to test different aspects of the model together in order to obtain a deeper understanding of how these variables are connected.
In addition, although there is considerable research aimed at testing the IMV model, conclusive results can be drawn only from select aspects. This is expected due to the large number of variables accounted for by the model. This is also expected as the IMV model provides a framework for understanding the emergence of suicidal thoughts and behaviour but does not provide an exhaustive set of pre-motivational phase variables or stage-specific moderators. While studies aimed at identifying other potential targets for intervention are very useful, further clarity and evidence is also required on variables already outlined and identified by the IMV model.
Another key limitation of the literature is the cross-sectional retrospective nature of the studies. Cross-sectional retrospective studies often limit the ability to identify causal relationships and results and may be limited by recall bias (Talari & Goyal, Citation2020). Establishing causal relationships could be key to identifying modifiable risk factors and targets for interventions. This is especially relevant since despite overwhelming support for the central pathway of the IMV model, the limited studies investigating the same prospectively found mixed results. One possible explanation for this could be that more accurate predictions could be achieved at certain timeframes rather than others. Indeed, it has been suggested that prospective studies of theoretical constructs over shorter periods of time such as weeks, days or hours may be particularly useful (Klonsky et al., Citation2018). Some authors have also suggested that ecological momentary assessments may be a method to address the issue with retrospective reporting (De Beurs et al., Citation2015). Thus, future work should employ prospective and ecological momentary analyses to measure real-time measures of theoretical variables.
Studies also often used single-item unvalidated measures for predictor or outcome variables. This was often the case where using a validated measure was not feasible or unavailable (e.g., exposure to suicide). Single-item dichotomised measures may not account for the differences in frequency, recency, or intensity of suicidal thoughts or behaviours and may misrepresent the strength of associations (Bernert et al., Citation2015; Russell et al., Citation2019). Thus, future research should aim to develop and utilise validated measures for measuring theoretical constructs.
Clinical implications
The implications of this review are limited by the disparity in the specific parts of the model that have been tested. Despite this, the key findings of this review can be useful in informing risk assessment and reduction strategies. For instance, clinical assessments should include feelings of perfectionism, defeat, internal entrapment, resilience, and perceived burdensomeness. As risk assessment tools have been largely inadequate (Carter et al., Citation2017), self-report measures should ideally be used in conjunction with clinical interviews. This would allow for a more nuanced understanding of the risk trajectories specific to the individual as well as information regarding their vulnerabilities, triggers, and resources.
This is also crucial in devising tailored treatment or safety plans. Specifically, a comprehensive understanding of not only how suicidal thoughts develop and result in behaviour but also the mechanisms by which an intervention is expected to impact these outcomes is key to effective intervention development (O’Connor et al., Citation2011). As such, intervention development should be informed by theory and supported by empirical evidence. For instance, based on the findings of this review, interventions addressing and reducing negative social comparisons through therapy among highly perfectionistic individuals may be useful in reducing feelings of defeat. Similarly, treatment for insecure attachment could also be useful in reducing defeat, especially among individuals that received parenting characterised by high overprotection and low care. Theoretical models such as the IMV model are also useful in developing interventions specific to the stage of suicidal thoughts or behaviour (O’Connor & Kirtley, Citation2018; Zortea et al., Citation2020b). For instance, interventions addressing defeat and entrapment could be targeted at individuals not experiencing suicidal thoughts, while interventions addressing volitional variables and safety planning could be developed in addition to reducing defeat and entrapment in individuals with active suicidal thoughts. A range of cognitive behavioural therapy techniques specific to addressing these risk factors could also be employed to address core beliefs that may be contributing to feelings of defeat and entrapment by understanding the events that trigger and maintain these feelings on an individual level and addressing them (Sandford et al., Citation2022).
Strengths and limitations of the present review
An important strength of the current review is that this is the first review to systematically select and synthesise the findings on the hypotheses of all aspects of the IMV model among a wide range of countries, settings, samples, and study designs. The current review further included a broad range of search strategies by traditionally searching databases as well as employing forward citation mining via databases and a search engine. Furthermore, empirical investigations of the IMV model were not restricted by quality or publication status.
It is important to consider the findings presented within the context of its limitations. Firstly, it should be noted that a subset of the papers was identified from Google Scholar. Several authors have suggested potential reproducibility issues on account of results dropping in and out of relevance (Bramer & Bain, Citation2017; Gusenbauer & Haddaway, Citation2020). However, the current review conducted multiple search updates to include potentially relevant results at different times and used the search engine primarily for forward citation mining alone. This may result in fewer changes in the results retrieved over time. The search engine was also employed alongside other search strategies from traditional databases which offer more consistent results over time. It is also important to note that the screening and inclusion of records were primarily conducted by the first reviewer while some authors have recommended having multiple reviewers screen all records to reduce potential selection bias. However, based on other papers (Moore et al., Citation2022) a percentage of the papers at full text screening stage were screened by a second reviewer to account for this. Another limitation of the current review due to clinical and methodological heterogeneity within the included studies was that a meta-analysis was not appropriate. Additionally, we conducted a systematic review rather than a scoping review as our primary aim was to synthesise the evidence supporting clinically pertinent hypotheses with an aim to inform practice (Arksey & O’Malley, Citation2005; Munn et al., Citation2018). Finally, the included studies were limited to studies reported in English which might have resulted in missing relevant studies published in different languages.
Conclusion
The evidence on the IMV model lend support to the associations between defeat, entrapment, and suicidal ideation as predicted in the model. However, there are key limitations in the literature. Firstly, only two studies have investigated all three phases of the IMV model in the same analysis. Additionally, even the two studies testing all phases of the model did not test the full pathway within the same analysis. There is also minimal overlap in the pre-motivational phase variables and motivational moderators tested, as well as variables compared between suicide-related outcome groups, resulting in inconclusive findings. Furthermore, the research conducted is primarily cross-sectional analyses. Future research should aim to address these concerns to further the theoretical understanding of suicidal behaviour and the clinical and policy implications of the IMV model.
Supplemental Material
Download PDF (1.3 MB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Angelakis, I., Austin, J. L., & Gooding, P. (2020). Association of childhood maltreatment with suicide behaviors among young people: A systematic review and meta-analysis. JAMA Network Open, 3(8), e2012563. https://doi.org/10.1001/jamanetworkopen.2020.12563
- Angelakis, I., Gillespie, E. L., & Panagioti, M. (2019). Childhood maltreatment and adult suicidality: A comprehensive systematic review with meta-analysis. Psychological Medicine, 49(7), 1057–1078. https://doi.org/10.1017/S0033291718003823
- Arksey, H., & O’Malley, L. (2005). Scoping studies: Towards a methodological framework. International Journal of Social Research Methodology, 8(1), 19–32. https://doi.org/10.1080/1364557032000119616
- Barzilay, S., & Apter, A. (2014). Psychological models of suicide. Archives of Suicide Research, 18(4), 295–312. https://doi.org/10.1080/13811118.2013.824825
- Bernert, R. A., Kim, J. S., Iwata, N. G., & Perlis, M. L. (2015). Sleep disturbances as an evidence-based suicide risk factor. Current Psychiatry Reports, 17(3), 15. https://doi.org/10.1007/s11920-015-0554-4
- Bramer, W., & Bain, P. (2017). Updating search strategies for systematic reviews using EndNote. Journal of the Medical Library Association, 105(3), 285–289. https://doi.org/10.5195/jmla.2017.183
- Branley-Bell, D., O'Connor, D. B., Green, J. A., Ferguson, E., O'Carroll, R. E., & O'Connor, R. C. (2019). Distinguishing suicide ideation from suicide attempts: Further test of the Integrated Motivational-Volitional Model of Suicidal Behaviour. Journal of Psychiatric Research, 117, 100–107. http://doi.org/10.1016/j.jpsychires.2019.07.007
- Carter, G., Milner, A., McGill, K., Pirkis, J., Kapur, N., & Spittal, M. J. (2017). Predicting suicidal behaviours using clinical instruments: Systematic review and meta-analysis of positive predictive values for risk scales. British Journal of Psychiatry, 210(6), 387–395. https://doi.org/10.1192/bjp.bp.116.182717
- Chu, C., Buchman-Schmitt, J. M., Stanley, I. H., Hom, M. A., Tucker, R. P., Hagan, C. R., Rogers, M. L., Podlogar, M. C., Chiurliza, B., Ringer, F. B., Michaels, M. S., Patros, C. H. G., & Joiner, T. E. (2017). The interpersonal theory of suicide: A systematic review and meta-analysis of a decade of cross-national research. Psychological Bulletin, 143(12), 1313–1345. https://doi.org/10.1037/bul0000123
- Cleare, S. (2019). Exploring the role of self-compassion in self-harm and suicidal ideation [PhD thesis]. University of Glasgow. http://theses.gla.ac.uk/id/eprint/81292
- De Beurs, D., Kirtley, O., Kerkhof, A., Portzky, G., & O’Connor, R. C. (2015). The role of mobile phone technology in understanding and preventing suicidal behavior. Crisis, 36(2), 79–82. https://doi.org/10.1027/0227-5910/a000316
- del Carpio, L., Rasmussen, S., & Paul, S. (2020). A theory-based longitudinal investigation examining predictors of self-harm in adolescents with and without bereavement experiences [original research]. Frontiers in Psychology, 11, 1153. https://doi.org/10.3389/fpsyg.2020.01153
- de Sousa, G. S., Perrelli, J. G. A., de Oliveira Mangueira, S., de Oliveira Lopes, M. V., & Sougey, E. B. (2020). Clinical validation of the nursing diagnosis risk for suicide in the older adults. Archives of Psychiatric Nursing, 34(2), 21–28. https://doi.org/10.1016/j.apnu.2020.01.003
- Dhingra, K., Boduszek, D., & O’Connor, R. C. (2015). Differentiating suicide attempters from suicide ideators using the integrated motivational–volitional model of suicidal behaviour. Journal of Affective Disorders, 186, 211–218. https://doi.org/10.1016/j.jad.2015.07.007
- Dhingra, K., Boduszek, D., & O'Connor, R. C. (2016b). A structural test of the Integrated Motivational-Volitional model of suicidal behaviour. Psychiatry Research, 239, 169–178. http://doi.org/10.1016/j.psychres.2016.03.023
- Forkmann, T., & Teismann, T. (2017). Entrapment, perceived burdensomeness and thwarted belongingness as predictors of suicide ideation. Psychiatry Research, 257, 84–86. http://doi.org/10.1016/j.psychres.2017.07.031
- Franklin, J. C., Ribeiro, J. D., Fox, K. R., Bentley, K. H., Kleiman, E. M., Huang, X., Musacchio, K. M., Jaroszewski, A. C., Chang, B. P., & Nock, M. K. (2017). Risk factors for suicidal thoughts and behaviors: A meta-analysis of 50 years of research. Psychological Bulletin, 143(2), 187–232. https://doi.org/10.1037/bul0000084
- Gilbert, P., & Allan, S. (1998). The role of defeat and entrapment (arrested flight) in depression: An exploration of an evolutionary view. Psychological Medicine, 28(3), 585–598. https://doi.org/10.1017/S0033291798006710
- Gusenbauer, M., & Haddaway, N. R. (2020). Which academic search systems are suitable for systematic reviews or meta-analyses? Evaluating retrieval qualities of google scholar, PubMed, and 26 other resources. Research Synthesis Methods, 11(2), 181–217. https://doi.org/10.1002/jrsm.1378
- Hollingsworth, D. W. (2012). An examination of the motivational phase of the integrated motivational-volitional model of suicide in african americans [Doctoral Thesis, Oklahoma State University]. APA PsycInfo. https://hdl.handle.net/11244/299513
- Hong, H. J., & Shin, S. H. (2021). Suicidal ideation of men with alcohol use disorder in South Korea: A structural equation modeling analysis. International Journal of Environmental Research and Public Health, 18(7), 3353. http://doi.org/10.3390/ijerph18073353
- Impellizzeri, F. M., & Bizzini, M. (2012). Systematic review and meta-analysis: A primer. International Journal of Sports Physical Therapy, 7(5), 493–503.
- Joiner, T. (2005). Why people die by suicide. Harvard University Press.
- Klonsky, E. D., Qiu, T., & Saffer, B. Y. (2017). Recent advances in differentiating suicide attempters from suicide ideators. Current Opinion in Psychiatry, 30(1), 15–20. https://doi.org/10.1097/YCO.0000000000000294
- Klonsky, E. D., Saffer, B. Y., & Bryan, C. J. (2018). Ideation-to-action theories of suicide: A conceptual and empirical update. Current Opinion in Psychology, 22, 38–43. https://doi.org/10.1016/j.copsyc.2017.07.020
- Levi-Belz, Y., Gvion, Y., & Apter, A. (2019). Editorial: The psychology of suicide: From research understandings to intervention and treatment [editorial]. Frontiers in Psychiatry, 10. https://doi.org/10.3389/fpsyt.2019.00214
- Li, X., Ren, Y., Zhang, X., Zhou, J., Su, B., Liu, S., Cai, H., Liu, J., & You, J. (2021). Testing the integrated motivational-volitional model of suicidal behavior in Chinese adolescents. Archives of Suicide Research, 25(3), 373–389. http://doi.org/10.1080/13811118.2019.1690607
- Lucht, L., Höller, I., Forkmann, T., Teismann, T., Schönfelder, A., Rath, D., Paashaus, L., Stengler, K., Juckel, G., & Glaesmer, H. (2020). Validation of the motivational phase of the integrated motivational–volitional model of suicidal behavior in a German high-risk sample. Journal of Affective Disorders, 274, 871–879. http://doi.org/10.1016/j.jad.2020.05.079
- Maass, S. W., Roorda, C., Berendsen, A. J., Verhaak, P. F., & de Bock, G. H. (2015). The prevalence of long-term symptoms of depression and anxiety after breast cancer treatment: A systematic review. Maturitas, 82(1), 100–108. https://doi.org/10.1016/j.maturitas.2015.04.010
- McClelland, H., Evans, J. J., & O'Connor, R. C. (2021). Exploring the role of loneliness in relation to self-injurious thoughts and behaviour in the context of the integrated motivational-volitional model. Journal of Psychiatric Research, 141, 309–317. http://doi.org/10.1016/j.jpsychires.2021.07.020
- Millner, A. J., Robinaugh, D. J., & Nock, M. K. (2020). Advancing the understanding of suicide: The need for formal theory and rigorous descriptive research. Trends in Cognitive Sciences, 24(9), 704–716. https://doi.org/10.1016/j.tics.2020.06.007
- Moore, F. R., Doughty, H., Neumann, T., McClelland, H., Allott, C., & O’Connor, R. C. (2022). Impulsivity, aggression, and suicidality relationship in adults: A systematic review and meta-analysis. EClinicalMedicine, 45, 101307. https://doi.org/10.1016/j.eclinm.2022.101307
- Munn, Z., Peters, M. D. J., Stern, C., Tufanaru, C., McArthur, A., & Aromataris, E. (2018). Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Medical Research Methodology, 18(1), 143. https://doi.org/10.1186/s12874-018-0611-x
- Naghavi, M., Abajobir, A. A., Abbafati, C., Abbas, K. M., Abd-Allah, F., Abera, S. F., Aboyans, V., Adetokunboh, O., Afshin, A., Agrawal, A., Ahmadi, A., Ahmed, M. B., Aichour, A. N., Aichour, M. T. E., Aichour, I., Aiyar, S., Alahdab, F., Al-Aly, Z., Alam, K., … Murray, C. J. L. (2017). Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: A systematic analysis for the global burden of disease study 2016. The Lancet, 390(10100), 1151–1210. https://doi.org/10.1016/S0140-6736(17)32152-9
- National Institutes of Health. (2014). Study quality assessment tools. https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools.
- Nock, M. K., Kessler, R. C., & Franklin, J. C. (2016). Risk factors for suicide ideation differ from those for the transition to suicide attempt: The importance of creativity, rigor, and urgency in suicide research. Clinical Psychology: Science and Practice, 23(1), 31–34. https://doi.org/10.1037/h0101734
- Nuij, C., van Ballegooijen, W., Ruwaard, J., de Beurs, D., Mokkenstorm, J., van Duijn, E., de Winter, R. F. P., O’Connor, R. C., Smit, J. H., Riper, H., & Kerkhof, A. (2018). Smartphone-based safety planning and self-monitoring for suicidal patients: Rationale and study protocol of the CASPAR (continuous assessment for suicide prevention And research) study. Internet Interventions, 13, 16–23. https://doi.org/10.1016/j.invent.2018.04.005
- O’Connor, R. C. (2007). The relations between perfectionism and suicidality: A systematic review. Suicide and Life-Threatening Behavior, 37(6), 698–714. https://doi.org/10.1521/suli.2007.37.6.698
- O’Connor, R. C. (2011a). The integrated motivational-volitional model of suicidal behavior [editorial]. Crisis: The Journal of Crisis Intervention and Suicide Prevention, 32(6), 295–298. https://doi.org/10.1027/0227-5910/a000120
- O’Connor, R. C. (2011b). Towards an integrated motivational–volitional model of suicidal behaviour. In R. C. O’Connor, S. Platt, & J. Gordon (Eds.), In international handbook of suicide prevention. https://doi.org/10.1002/9781119998556.ch11
- O’Connor, R. C., Ferguson, E., Scott, F., Smyth, R., McDaid, D., Park, A. L., Beautrais, A., & Armitage, C. J. (2017). A brief psychological intervention to reduce repetition of self-harm in patients admitted to hospital following a suicide attempt: A randomised controlled trial. The Lancet Psychiatry, 4(6), 451–460. https://doi.org/10.1016/S2215-0366(17)30129-3
- O’Connor, R. C., & Kirtley, O. J. (2018). The integrated motivational-volitional model of suicidal behaviour. Philosophical Transactions of the Royal Society B: Biological Sciences, 373(1754), 20170268. https://doi.org/10.1098/rstb.2017.0268
- O’Connor, R. C., & Nock, M. K. (2014). The psychology of suicidal behaviour. The Lancet Psychiatry, 1(1), 73–85. https://doi.org/10.1016/S2215-0366(14)70222-6
- O’Connor, R. C., Rasmussen, S., & Beautrais, A. (2011). Recognition of suicide risk, crisis helplines, and psychosocial interventions: A selective review. In R. C. O'Connor, S. Platt, & J. Gordon (Eds.), International handbook of suicide prevention. https://doi.org/10.1002/9781119998556
- Ordóñez-Carrasco, J. L., Cuadrado-Guirado, I., & Rojas-Tejada, A. J. (2020a). Frustrated interpersonal needs as a motivational moderator in the integrated motivational-volitional model. Death Studies, 46(4), 1003–1008. http://doi.org/10.1080/07481187.2020.1783031
- Ordóñez-Carrasco, J. L., Cuadrado-Guirado, I., & Rojas-Tejada, A. J. (2021a). Experiential avoidance in the context of the integrated motivational–volitional model of suicidal behavior. Crisis, 42(4), 284–291. http://doi.org/10.1027/0227-5910/a000721
- Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., Shamseer, L., Tetzlaff, J. M., Akl, E. A., Brennan, S. E., Chou, R., Glanville, J., Grimshaw, J. M., Hróbjartsson, A., Lalu, M. M., Li, T., Loder, E. W., Mayo-Wilson, E., McDonald, S., … Moher, D. (2021). The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ, 372, n71. https://doi.org/10.1136/bmj.n71
- Ribeiro, J. D., Linthicum, K. P., Joiner, T. E., Huang, X., Harris, L. M., & Bryen, C. P. (2021). Do suicidal desire and facets of capability for suicide predict future suicidal behavior? A longitudinal test of the desire–capability hypothesis. Journal of Abnormal Psychology, 130(3), 211–222. http://doi.org/10.1037/abn0000595
- Ritchie, H., Spooner, F., & Roser, M. (2018). Causes of death. Published online at OurWorldInData.org. https://ourworldindata.org/causes-of-death [Online Resource].
- Russell, K., Allan, S., Beattie, L., Bohan, J., MacMahon, K., & Rasmussen, S. (2019). Sleep problem, suicide and self-harm in university students: A systematic review. Sleep Medicine Reviews, 44, 58–69. https://doi.org/10.1016/j.smrv.2018.12.008
- Russell, K., Rasmussen, S., & Hunter, S. C. (2020c). Does mental well-being protect against self-harm thoughts and behaviors during adolescence? A six-month prospective investigation. International Journal of Environmental Research and Public Health, 17(18), 6771. http://doi.org/10.3390/ijerph17186771
- Sandford, D. M., Thwaites, R., Kirtley, O. J., & O’Connor, R. C. (2022). Utilising the integrated motivational volitional (IMV) model to guide CBT practitioners in the use of their core skills to assess, formulate and reduce suicide risk factors. The Cognitive Behaviour Therapist, 15, e36. https://doi.org/10.1017/S1754470X22000344
- Schotte, D. E., & Clum, G. A. (1987). Problem-solving skills in suicidal psychiatric patients. Journal of Consulting and Clinical Psychology, 55(1), 49–54. https://doi.org/10.1037/0022-006X.55.1.49
- Scowcroft, E. (2019). Exploring the effectiveness of Samaritans’ Listener Scheme and prisoner suicide through the lens of the IMV model of suicidal behaviour [Doctoral thesis]. Nottingham Trent University. https://doi.org/10.13140/RG.2.2.14957.92649.
- Stanley, I. H., Hom, M. A., Rogers, M. L., Hagan, C. R., & Joiner, T. E. (2016). Understanding suicide among older adults: A review of psychological and sociological theories of suicide. Aging & Mental Health, 20(2), 113–122. https://doi.org/10.1080/13607863.2015.1012045
- Talari, K., & Goyal, M. (2020). Retrospective studies – utility and caveats. Journal of the Royal College of Physicians of Edinburgh, 50(4), 398–402. https://doi.org/10.4997/jrcpe.2020.409
- The Scottish Government. (2022). Creating hope together Scotland’s suicide prevention strategy 2022–2032. https://www.gov.scot/publications/creating-hope-together-scotlands-suicide-prevention-strategy-2022-2032/documents/.
- Tucker, R. P., O’Connor, R. C., & Wingate, L. R. (2016). An investigation of the relationship between rumination styles, hope, and suicide ideation through the lens of the integrated motivational-volitional model of suicidal behavior. Archives of Suicide Research, 20(4), 553–566. http://doi.org/10.1080/13811118.2016.1158682
- Van Orden, K. A., Witte, T. K., Cukrowicz, K. C., Braithwaite, S. R., Selby, E. A., & Joiner, T. E., Jr. (2010). The interpersonal theory of suicide. Psychological Review, 117(2), 575–600. https://doi.org/10.1037/a0018697
- Wetherall, K., Cleare, S., Zortea, T., & O’Connor, R. (2020). Status of the integrated motivational-volitional model of suicidal behaviour. In D. De Leo & V. Poštuvan (Eds.), Reducing the toll of suicide: Resources for communities, groups, and individuals (pp. 169–184). Hogrefe.
- Wetherall, K., Robb, K. A., & O'Connor, R. C. (2018). An examination of social comparison and suicide ideation through the lens of the integrated motivational–volitional model of suicidal behavior. Suicide and Life-Threatening Behavior, 49(1), 167–182. http://doi.org/10.1111/sltb.2019.49.issue-1
- Williams, J. M. G (2001). Suicide and attempted suicide: Understanding the cry of pain. Penguin.
- World Health Organization. (2021). Suicide worldwide in 2019: Global health estimates.
- Zortea, T. C., Cleare, S., Melson, A. J., Wetherall, K., & O’Connor, R. C. (2020b). Understanding and managing suicide risk. British Medical Bulletin, 134(1), 73–84. https://doi.org/10.1093/bmb/ldaa013
- Zortea, T. C., Cleare, S., Wetherall, K., Melson, A., & O’Connor, R. (2021a). On suicide risk: From psychological processes to clinical assessment and intervention. https://doi.org/10.1016/B978-0-12-818697-8.00073-X
- Zortea, T. C., Gray, C. M., & O’Connor, R. C. (2021b). The relationship between adult attachment and suicidal thoughts and behaviors: A systematic review. Archives of Suicide Research, 25(1), 38–73. https://doi.org/10.1080/13811118.2019.1661893