
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
Physical activity is the most important lifestyle factor to contribute to a healthy early life. International recommendations are that children should be vigorously physically active for at least 1 h per day, and in Greenland, authorities have claimed a goal of being the world’s most active population. Since 1994, the Health Behaviour in School-aged Children (HBSC) has measured physical activity among school-children in Greenland by questionnaire data, but the measurement properties of self-reported data in comparison to more objectively measured accelerometer data are unknown. The present paper describes the first study using clinical measures of physical activity among Greenlandic youth. Seventy-two school-children (56% girls) with a mean age of 12 years (range 25%; 75% was 11.5; 12.25) wore accelerometers for seven consecutive days, and data produced significant and informative findings for both practice and future research. Fifty-two per cent of the school-children met the international recommendations of being physically active >1 h per day, when measured by accelerometers, but self-reported data reported a prevalence of 10% meeting the recommendations. A majority of this sample of Greenlandic school-children lives up to international recommendations, which indicates that the goal of being the world’s most active population is within reach.
Introduction
Physical activity (PA) is the most important lifestyle factor, which contributes to a healthy life. PA contributes to the prevention and treatment of numerous diseases, e.g. diabetes and obesity [Citation1] and but also to enhance psychological and social health outcomes [Citation2]. The rapid pace of economic development is affecting human functioning to such a degree that the need for physical activity, which has always been recognised as a biological and natural need, has been significantly reduced. Over the past generations, societal developments have supported an increasingly sedentary lifestyle, and obesity as well as many other health-related diseases are increasing consequently for both adults and children [Citation3–5]. Among children and adolescents, the health benefits of PA are numerous and well documented. Earlier studies have shown that an active life has a positive impact on children and adolescents’ heart, circulation, muscle strength, motor skills, balance and on the hormonal and immune systems, and likewise PA leads to better fitness, stronger bones, less fat in the blood and less risk of precursors to diabetes [Citation6,Citation7]. PA has also shown to have a positive impact on the well-being and mental health of children and adolescents [Citation8]. Finally, PA has been shown to have a positive effect in relation to learning [Citation2,Citation9].
To promote the focus on PA in the general population, The Greenlandic Sports Federation has set the goal of Greenland being the most active country in the world by 2030 [Citation10].
Since 1994, the Greenlandic contribution to the Health Behaviour in School-aged Children (HBSC) has collected questionnaire data on school school-children’ PA level. HBSC Greenland is the Greenlandic contribution to the international research collaboration on monitoring the health and well-being of schoolchildren, Health Behaviour in School-aged Children. HBSC Greenland is Greenland’s only nationwide survey among children and young people and has collected data every 4 years since 1994, and invited all schools with school-children from 5th to 10th grade to participate. In 2022, the 8th consecutive data collection was performed. Data from HBSC Greenland are included in international reports, and national data is widely used to describe the health and well-being of Greenlandic school-children, as well as to monitor the public health programme Inuuneritta [Citation11,Citation12]. The area of PA and sedentary behaviour is of great research and public health interest, and the researchers behind HBSC have for many years wanted to upgrade the knowledge obtained through the questionnaire by learning more about the validity of the questions used in the HBSC questionnaire. The HBSC question resembles the first PACE+ item, which asks respondents to report the number of days (0–7) they were physically active for at least 60 min per day in the past week (more detailed information is given in the Methods section).
Cross-sectional surveys collecting data from questionnaires are an easy way to attain representative knowledge about a population. Questionnaire data are considered suitable for obtaining information about the types and places of PA, but questionnaire data has been shown to underestimate the proportion of children meeting the PA requirements [Citation13,Citation14]. When relying on self-reports in the estimation of intensity and duration of PA, it is important to include the potential bias of recalling the information, and the subjective assessment of when something counts as vigorous PA [Citation15]. The relevance of examining potential bias is especially true for children and young people, who typically have a more sporadic activity behaviour with many different types of play and movement activities in different contexts spread out throughout the day in combination with more organised sports activity in school and leisure [Citation16]. Furthermore, self-reports of PA are limited by social desirability, and cognitive complexity of recalling PA levels [Citation14].
Since data from HBSC has been used to assess the proportion of Greenlandic school-children who adhering to the international recommendations on PA, it is relevant to assess the accuracy of the self-reported data.
No previous studies have conducted objective measurements of PA among Greenlandic children, so the present study both aims to report first results from objective data collected from accelerometers and also examines the association between the objective data and self-reports from the same respondents.
Methods
Objective measures: accelerometer data
In this study, the objective physical activity levels were measured for seven consecutive days using an Axivity A×3triaxial accelerometers placed on the right thigh with surgical tape. The participating school-children received the accelerometers when they were at school, and were instructed to wear the accelerometer 24 h/day also during shower, swimming or sleeping. All school-children were given extra surgical tape to take home to re-attach the accelerometer should it fall off. Periods with non-wear were identified by a combination of minimal activity and temperature and those data were excluded from the analysis.
Accelerometer measurements from the thigh have proven to make robust classification of different types of activity, e.g. sitting, standing, walking, cycling, and running. In addition, it has previously been found that Axivity A×3measurement using adhesive patch at thigh 24 h/day have high compliance among children [Citation17]. Furthermore, data from the Axivity A×3accelerometers can produce accurate measures of activity types using algorithms developed in adults [Citation18] and adapted to children and adolescents [Citation19]. The cut-off points used in the present study were 0–100 counts/minute=sedentary, 101–4822 counts/min=light, 4823–9143 counts/min=moderate, and > 9143=vigorous.
Subjective measures: questionnaire data
The researchers filled out a questionnaire together with the respondent to ensure complete and most accurate information. The questionnaire included information on age and gender of the respondent, height & weight, number of adults co-habiting with the respondent and self-rated health. The questionnaire also contained the question used on PA in the HBSC, an item which is like the widely used item in Global School-based Student Health Survey (GSHS) and Patient-Centered Assessment and Counselling for Exercise Plus Nutrition (PACE+); For the past 7 days, how many days were the child physically active at least 60 minutes per day? With 8 response categories from 0 (zero) to 7 days.
Study population
The target group for the study was school school-children in grades 6 to 10, as they are the HBSC study population. Two schools in Nuuk and Qaqortoq respectively were invited to participate via a visit to the school principal. The principal was asked to appoint classes to ask in person, and when their teacher had given consent, the researchers visited the class in an allocated time. Thorough oral information was provided to all school-children present, and information leaflets and consent forms were handed out in the classes. The survey was conducted voluntarily when consent had been given from the parents, and the study was performed with confidential treatment of the data of the schools and participating school-children. Prior to the data collection, the school-children were given information leaflets with a thorough explanation of the purpose and scope of the study. A total of 86 school-children participated in the study.
Informed consent
School-children could only participate in the survey if their parent/guardian had signed the consent form provided. The declaration of consent was prepared by the project’s researchers in collaboration with legal advisors from University of Southern Denmark. Following an inquiry, the Research Ethics Committee considered that due to the design of the study (with non-invasive measurements and anonymous questionnaire survey based on voluntary consent), a notification to the Danish Data Protection Agency was not necessary.
Criteria for data handling
A key aspect of analyses with accelerometers is setting criteria for legitimate data. This applies decisions on how many hours the school-children must have worn the accelerometer to constitute a valid day (number of hours carried), as well as how many valid days and which days (weekday/weekend) are required for each school-children to be included in the overall analysis. For the present paper, a minimum requirement of 3 days was selected, and each day corresponded to at least 8 h of recorded data. Following these criteria, a total of 72 school-children aged 11–16 years were included in the study. shows the distribution of the number of days school-children wore the accelerometer on weekdays and weekends, respectively.
Table 1. Descriptive statistics for all 72 school-children – mean and SD (for normally distributed data), and median with range (for not normally distributed data) as well as minimum and maximum values.
Analysis
Data for analyses constituted a datafile including the accelerometer data with school-children’s average daily PA levels. The accelerometer data were coupled with the questionnaire data, from the same school-children into an SPSS and STATA -file.
The data was used to assess the proportion of Greenlandic schoolchildren, who lived up to the WHO recommendations of a minimum of 60 minutes of PA per day on average over a week. Cross tabulations were generated to compare the results from the accelerometer measurements and the self-reports, and identification of the inconsistencies were initially examined graphically and by comparing frequency tables. A 2 × 2 table were constructed to identify true and false positives and negatives, and the test performance was examined by calculating sensitivity, specificity, and positive and negative predictive values. The accelerometer measures were considered the golden standard.
Results
Seventy-two school-children had valid accelerometer data and were included in the study. The school-children were 12 (11.6; 16.0) years old, whereof 56% were girls (). also shows the distribution of height and weight as well as the data on objective measured sedentary time and PA. Mean sedentary time was 382 min per day or 6 h and 22 min. The mean time of light PA was 271 min, or 4 h 31 min per day, mean time of moderate PA was 52 min per day, and the mean time of vigorous PA was 13 min per day ().
Of the included school-children, 90% of the girls and 62% of the boys wore the accelerometer on all weekdays, and 95% of girls and 81% of boys wore the accelerometer on both days of the weekend ().
Table 2. Valid days with accelerometer data (numbers and column %).
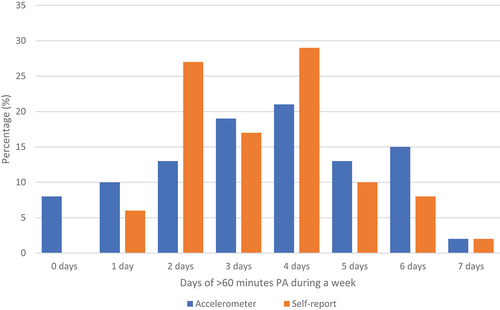
The association between the self-reported PA and the accelerometer-measured PA is illustrated by . The figure only includes school-children with accelerometry data for 7 days (n = 48). As shown, no school-children reported that they do >60 min of PA for 0 days during the week, however, 8% of the school-children with >60 min PA for 0 days during the week according to the accelerometer measurements. The discrepancy was the same for 1, 3, 5 and 6 days, respectively, where the underreporting of self-reports persisted. For 2 and 4 days, there was an overreporting. For 7 days, the accelerometer-measurement and self-reports matched.
Figure 1. Percentage of school-children (n = 48) with at least 60 min PA per day through the week.
shows the data examining the measurement properties of the self-reports of PA. 56% (40/72) of the school-children met the recommendations of >60 min of PA per day on average over the week according to the accelerometer measurements. Out of the 40 school-children, who met the WHO recommendations, only 10% (4/40) reported to meet the recommendations when asked in the questionnaire.
Table 3. Number of school-children adhering to WHO recommendations of >60 min PA per day on average.
Calculations were done to assess the measurement properties. The ability for the self-reports to classify the ones meeting the WHO recommendations correctly, denoted , was 4/40 = 10%. The ability for the self-reports to classify the ones not meeting the WHO recommendations correctly, the
, was 32/32 = 100%.
The predictive value of a positive test (in this case meeting the WHO recommendations on PA) was 4/4 = 100%, and the predictive value of a negative test (in this case not meeting the WHO recommendations)
was 32/68 = 47%.
Discussion
Main findings
The overall finding of the present study is that the HBSC questionnaire is not recommended to estimate the proportion of school-children adhering to the WHO recommendations on PA, due to substantial under-reporting of PA for the physically active school-children. Even though some studies point to a weakness in having a low proportion in their data meeting the recommendations and were therefore not able to calculate the agreement between self-reported and accelerometer-measured levels of PA, most other studies confirm this finding [Citation14,Citation15,Citation20–22].
The data collected from self-reports showed a sensitivity of 10%, which means that only 10% of the school-children adhering to the WHO recommendations, were identified by the self-reports. The predictive value of a negative test, in this case not meeting the recommendation were 47%, meaning that in less than half the cases, this result was correct. The conclusion to not consider data from HBSC Greenland as an accurate measure of proportions meeting international guidelines is based on the above calculations.
The important secondary finding from the present study is that 56% of the school-children are meeting the recommendations from the WHO, which is a high proportion. A Danish study from 2018 among 11- to 15-year-olds showed that 26% met the WHO recommendation [Citation23], and since the present study had copied the data collection method, it is reasonable to conclude that Greenlandic school-children is probably among the most active youth in the world.
The literature also points to the importance of considering the cultural context; Booth emphasises that findings are to be tested in other cultural contexts [Citation20], Hardie Murphy points out that questionnaires appraised in one population cannot be systematically transferred to other geographical regions or populations [Citation21], and Alkhraiji et al. recommended that studies needed to investigate comparable populations in different countries using the same method, to confirm any findings [Citation15]. Since the present study is the first of its kind in a Greenlandic population, the authors aim to replicate it among other age groups and in other geographical areas. Hopefully other research teams in the Arctic will collect similar data to examine whether the high levels of PA among Greenlandic school-children are also found in comparable populations.
Methodological considerations
Studies that collect data from accelerometers often experience problems when the measurement devices (in this case taped around the thigh of the respondent) are not worn correctly or are taken off during the period of data collection. The present study did not suffer from this bias, since very few measurement devices were worn incorrectly. The research assistants had also spent a substantial amount of time visiting the classrooms and asking the school-children if everything went well, and at these visits, small corrections could be made, to make sure that the measurement devices were worn correctly.
One of the weaknesses of performing a study as Danish researcher in a Greenlandic context is a language barrier. Some of the barriers were eliminated, since the work was with school-children, and the researchers managed to create a playful atmosphere, but the older school-children did not seem to enjoy the data collection as much as the younger ones. Future studies can benefit from including younger children and older age groups into studies of PA, since PA is incorporated into Greenlandic culture and leisure time. High-quality data of what seems to be a very active population can be collected relatively easily.
Another well-known weakness when collecting data on PA is the increased focus on PA that increases the level of PA in the study period. Even though there may be an increased level of PA in the specific period, the collected data is compared to other similar data collected, so any comparisons are done with studies, that suffer from the same type of bias. Since the levels of PA among Greenlandic school-children are substantially higher than that of e.g. Danish school-children, the conclusion(s) about higher levels of PA among Greenlandic children is indisputable. Ridgers and colleagues have pointed to a limitation in self-reports that youth overestimate their PA engagement [Citation14], which is a finding this study is contradicting fully.
The literature on PA among school-children generally report higher levels of PA among boys than girls, and as pointed to by Alkhraiji it may be misleading to combine the genders in analyses [Citation15]. Since the purpose of the present study mainly was to compare a questionnaire item used for both boys and girls, the data was combined. In most other situations, analyses would be more meaningful if stratified between boys and girls.
The present study did not replicate calculations on correlation (by e.g. Spearman or Pearson’s correlations), as only one other study suggests that a single-item measure provides a reliable and valid instrument [Citation24], whereas most other studies report of poor/low or moderate correlation [Citation14,Citation15,Citation20–22]. Hence, the authors found the usefulness of assessing the accuracy by sensitivity and specificity and positive and negative predictive values, to meet the purpose of the study; to assess the accuracy of the Greenlandic HBSC data to report the proportion of Greenlandic school-children meeting requirements.
Implications for the future
The present study is the first of its kind in Greenland, since no earlier studies have objectively measured PA among school-children. The researchers who collected data experienced how the school-children enjoyed wearing the devices and that the compliance was high. As the data collection went smooth, it seems that data collection of levels of PA is welcomed among school-children in Greenland. Future studies can benefit from this positive experience. As reliability and validity studies are population-specific, the knowledge gap should be narrowed even further by studies collecting data on other parts of the Greenlandic population, and in other age groups. The Greenlandic Sports Association is aiming to have the most physically active population by 2030, and with the results indicated from 72 school-children from Qaqortoq and Nuuk, the goal is within reach, but would benefit from being confirmed by other studies in the Arctic region for generalisation.
Acknowledgments
The results presented in the present paper are presented clearly, honestly and without fabrication, falsification, or inappropriate data manipulation. The results of the present study do not constitute endorsement by ACSM.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Czenczek-Lewandowska E, Grzegorczyk J, Mazur A. Physical activity in children and adolescents with type 1 diabetes and contemporary methods of its assessment. Pediatr Endocrinol Diabetes Metab. 2018;24(4):179–965. doi: 10.5114/pedm.2018.83364
- Eime RM, Young JA, Harvey JT, et al. A systematic review of the psychological and social benefits of participation in sport for children and adolescents: informing development of a conceptual model of health through sport. Int J Behav Nutr Phys Act. 2013;10(1):98. :
- Gray C, Gibbons R, Larouche R, et al. What is the relationship between outdoor time and physical activity, sedentary behaviour, and physical fitness in children? A systematic review. Int J Environ Res Public Health. 2015;12(6):6455–6474. doi: 10.3390/ijerph120606455
- Tremblay MS, Colley RC, Saunders TJ, et al. Physiological and health implications of a sedentary lifestyle. Appl Physiol Nutr Metab. 2010;35(6):725–740. doi: 10.1139/h10-079
- Wu XY, Han LH, Zhang JH, et al. The influence of physical activity, sedentary behavior on health-related quality of life among the general population of children and adolescents: a systematic review. PLoS One. 2017;12(11):e0187668. doi: 10.1371/journal.pone.0187668
- Laure P, Leleu E, Mangin G. Physical activity health promotion for pre-school children: benefits and barriers. Sante Publique. 2008;20(3):239–248. doi: 10.3917/spub.083.0239
- Sothern MS, Loftin M, Suskind RM, et al. The health benefits of physical activity in children and adolescents: implications for chronic disease prevention. Eur J Pediatr. 1999;158(4):271–274. doi: 10.1007/s004310051070
- Dimitri P, Joshi K, Jones N. Moving more: physical activity and its positive effects on long term conditions in children and young people. Arch Dis Child. 2020;105(11):1035–1040. doi: 10.1136/archdischild-2019-318017
- Bidzan-Bluma I, Lipowska M. Physical activity and cognitive functioning of children: a systematic review. Int J Environ Res Public Health. 2018;15(4):800. doi: 10.3390/ijerph15040800
- Greenland Sports Federation. 2020. Greenland - The world’s most physically active country in 2030? Available from http://www.anguniakkavut.gl/en/nyheder/gr%C3%B8nland—verdens-mest-fysisk-aktive-land-i-2030
- Naalakkersuisut. 2012. Inuuneritta II - Naalakkersuisuts strategier og målsætninger for folkesundheden 2013-2019 [Inuuneritta II Naalakkersuisuts strategies and aims for public health 2013-2019, in Danish]. Available from https://www.yumpu.com/da/document/view/18316047/inuuneritta-ii-peqqikgl
- Naalakkersuisut. 2020. Inuuneritta III - Naalakkersuisuts Strategi For Samarbejdet Om Det Gode Børneliv 2020-2030 [Naalakkersuisut’s Strategy For The Jointed Effort For a Good Life For All Children 2020-2030, In Danish]. Available from Nuuk: https://paarisa.gl/nyheder/2020/09/2020_inuuneritta_iii?sc_lang=da
- Kyan A, Tanaka S, Takakura M, et al. Validity of Japanese version of a two-item 60-minute moderate-to-vigorous physical activity screening tool for compliance with WHO physical activity recommendations. J Phys Fitness Sports Med. 2021;10(2):99–107. doi: 10.7600/jpfsm.10.99
- Ridgers ND, Timperio A, Crawford D, et al. Validity of a brief self-report instrument for assessing compliance with physical activity guidelines amongst adolescents. J Sci Med Sport. 2012;15(2):136–141. doi: 10.1016/j.jsams.2011.09.003
- Alkhraiji MH, Barker AR, Williams CA. Reliability and validity of using the global school-based student health survey to assess 24 hour movement behaviours in adolescents from Saudi Arabia. J Sports Sci. 2022;40(14):1578–1586. doi: 10.1080/02640414.2022.2092982
- Staudenmayer J, Zhu W, Catellier DJ. Statistical considerations in the analysis of accelerometry-based activity monitor data. Med Sci Sports Exerc. 2012;44(Suppl 1S):S61–67. doi: 10.1249/MSS.0b013e3182399e0f
- Schneller MB, Bentsen P, Nielsen G, et al. Measuring children’s physical activity: compliance using skin-taped accelerometers. Med Sci Sports Exerc. 2017;49(6):1261–1269. doi: 10.1249/mss.0000000000001222
- Skotte J, Korshøj M, Kristiansen J, et al. Detection of physical activity types using triaxial accelerometers. J Phys Act Health. 2014;11(1):76–84. doi: 10.1123/jpah.2011-0347
- Brønd JC, Grøntved A, Andersen LB, et al. Simple method for the objective activity type assessment with preschoolers, children and adolescents. Children (Basel). 2020;7(7):72.
- Booth ML, Okely AD, Chey T, & Bauman A. The reliability and validity of the physical activity questions in the WHO health behaviour in schoolchildren (HBSC) survey: a population study. Br J Sports Med. 2001;35(4):263. doi: 10.1136/bjsm.35.4.263
- Hardie Murphy M, Rowe DA, Belton S, et al. Validity of a two-item physical activity questionnaire for assessing attainment of physical activity guidelines in youth. BMC Public Health. 2015;15(1):1080. doi: 10.1186/s12889-015-2418-6
- Rangul V, Holmen TL, Kurtze N, et al. Reliability and validity of two frequently used self-administered physical activity questionnaires in adolescents. BMC Med Res Methodol. 2008;8(1):47. doi: 10.1186/1471-2288-8-47
- Toftager M, Brønd JC. 2019. Fysisk aktivitet og stillesiddende adfærd blandt 11-15-årige: National monitorering med objektive målinger [Physical activity and sedentary behavior among 11-15 year olds: National monitoring with objective measures, in Danish] (8770141045). Available from https://www.sst.dk/da/Udgivelser/2019/Fysisk-aktivitet-og-stillesiddende-adfaerd-blandt-11-15-aarige
- Scott JJ, Morgan PJ, Plotnikoff RC, et al. Reliability and validity of a single-item physical activity measure for adolescents. J Paediatr Child Health. 2015;51(8):787–793. doi: 10.1111/jpc.12836