
Abstract
Squamous cell carcinoma (SCC) in situ can occur on any skin or mucus surface and is more commonly found in elderly patients on areas of skin that have been sunburnt. Most previous case reports are from dermatologists, with few published reports from pathologists. In this study, three patients underwent pathological routine and auxiliary immunohistochemical (IHC) examination and were ultimately diagnosed with pagetoid SCC in situ – a different diagnosis from the initial clinical assessment. All three patients received a complete resection of the skin mass. After follow-up, as of June 2023, the patients had no tumour recurrence or metastasis. Pagetoid SCC in situ is a particular type of SCC in situ that has no specific features in clinical manifestations, gross diagnosis or histopathological sections. The final diagnosis depends on IHC staining. Pagetoid SCC in situ expresses EMA, CK5/6 and p63 but not CEA, CK8 or S-100, which are expressed in extramammary Paget’s disease. Pagetoid SCC in situ is usually only locally invasive, and the main treatment is complete surgical resection. The prognosis is related to human papillomavirus infection, surgical margin closure, disease location, tumour thickness and other factors.
Introduction
Squamous cell carcinoma (SCC) of the skin is a type of cancer that originates from the keratinocytes of the epidermis or its appendages and is the second most common skin cancer after basal cell carcinoma, accounting for approximately 20% of all cutaneous malignancies.Citation1 Squamous cell carcinoma in situ refers to the cancer tissue that does not break through the basement membrane and has no lymph node or distant metastasis. It can develop into SCC, corresponding to high-grade squamous intraepithelial neoplasia.Citation2 Pagetoid SCC in situ is a particular type of SCC in situ and is rare; with it being most common in those aged 40–50 years of age.Citation3 The integration of high-risk human papillomavirus (HPV) has emerged in some pagetoid SCC in situ, which may be associated with its pathogenesis, but it must be studied further.Citation4 It mainly occurs in elderly patients on areas of skin that have been sunburnt. Rarely, it can also occur at the vulvar anatomical district.Citation5 It may initially appear in the form of a rash, sometimes accompanied by itching, and may be mistaken for eczema in dermatology. Following hormone therapy, the tumour slowly expands until a skin mass excision can be performed.Citation6 One of the diagnostic challenges of SCC is to differentiate it from Paget’s disease of the skin, which is a rare intraepithelial adenocarcinoma that usually affects the skin of the nipple, areola, vulva or perianal region. Paget’s disease can mimic the clinical and histological features of SCC, as both can show hyperkeratosis, acanthosis and pagetoid cells in the epidermis. However, Paget’s disease is usually associated with an underlying malignancy, such as breast cancer, and has a different immunohistochemical (IHC) profile from SCC.Citation7 Breast atypical SCC in situ is a particular type of SCC in situ. The cytoplasm of tumour cells is bright, and it is difficult to distinguish this disease from extramammary Paget’s disease (EMPD) in morphology, leading to misdiagnosis.Citation8 The diagnosis of SCC in situ must be clarified by physicians based on the patient’s condition and multiple test results. For the treatment of SCC in situ, surgical resection is the most effective option, with the use of local antibiotics and ophthalmic corticosteroids. The diagnosis should be confirmed through a set of markers, including cytokeratin (CK) 5/6, p63, epithelial membrane antigen (EMA), carcinoembryonic antigen (CEA), CK8 and S-100.Citation2 Differentiation between pagetoid SCC and Paget’s disease can be timely identified by pathological findings. According to the results of a pathological biopsy, early and accurate disease diagnosis is helpful for the development of treatment options, improving the cure rate of patients while contributing to the prognosis of patients. Most previous case reports are from dermatologists, with few published reports from pathologists. In this study, we report three cases of patients who were initially diagnosed with Paget’s disease of the skin but were later confirmed through IHC to have SCC in situ. Written informed consent was obtained from each of the patients.
Case Report
Essential Information
Case 1
A 70-year-old man with a rash on his left thigh for >2 years. The patient developed a soybean-sized erythema on his left thigh >2 years ago without obvious cause, and slight pruritus appeared later, which was not significantly relieved by self-applied 999 Pi Yan Ping ointment (a compound dexamethasone acetate cream with anti-inflammatory, anti-allergic and skin-itching relief properties). In the past 2 years, the erythema had gradually increased, forming plaque with a maximum diameter of 14.7 mm. The patient experienced some minor pain, occasional pruritus and no surface ulceration. He was previously healthy and has denied having any history of exposure to radioactive substances or arsenic-containing pesticides, bad habits or a family history of similar diseases. The general pathological description was as follows: An area of fusiform skin tissue, 20×15 × 7 mm in size, with a grey–yellow and grey–brown rough surface, a maximum diameter of 14.7 mm and a section of grey.
Case 2
An 83-year-old man with a rash on the left side of his back for >3 years. The patient developed pruritus on the left side of his back without obvious cause >3 years ago and then developed erythema. Without treatment, the plaque had gradually enlarged, reaching a maximum diameter of 12.7 mm. The patient was previously healthy and has denied having a history of exposure to radioactive substances or arsenic-containing pesticides, bad habits or a family history of similar diseases.
Case 3
An 88-year-old man with a rash on his left calf for >2 years. The patient developed a pea-sized rash on his left calf >2 years ago without obvious cause, and the rash had recently increased to a maximum diameter of 13.0 mm. The patient was previously healthy and has denied having a history of exposure to radioactive substances or arsenic-containing pesticides, bad habits or a family history of similar diseases.
Morphological and immunohistochemical observation
The resected specimens were fixed with 10% neutral formalin, dehydrated routinely, embedded in paraffin, sectioned, stained with haematoxylin and eosin (HE) and observed under a light microscope. Immunohistochemical staining was performed using the EnVision two-step method, with antibodies including CK5/6, p63, CK7, p16, CEA, S-100 and HMB45. The antibodies were purchased from Beijing Zhongshan Jinqiao Biotechnology (Beijing, China). Immunohistochemical and in situ hybridisation staining were performed following the reagent instructions, and positive and negative controls were set. The sections were also stained with periodic acid-Schiff stain, with reagents purchased from Beijing Zhongshan Jinqiao Biotechnology.Citation9 The sections were re-read by two senior doctors.
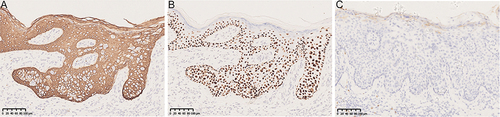
The microscope examination revealed hyperkeratosis in the epidermis, partial keratosis, hypertrophy in the spine and numerous nested pagetoid cells in the whole layer. The cell arrangement was disordered, the cytoplasm was rich, transparent and vacuolar, and the nuclei were large, deeply stained and atypically shaped; in addition, the nucleolus was clearly visible and pathological mitosis was occasionally observed. The basement membrane was intact, and a large number of lymph and plasma cells were infiltrated at the epidermal–dermal junction (). Immunohistochemical EnVision staining showed that the pagetoid cells expressed CK5/6, p63 and EMA but not CEA, CK8 or S-100. The final pathological diagnosis was pagetoid SCC in situ ().
Figure 1 HE staining: A large number of nested Paget-like cells were found throughout the epidermis. The cytoplasm of tumor cells is rich, transparent and vacuolar. The basement membrane was intact, and a large number of lymph and plasma cells were infiltrated at the epidermal dermal junction. (A) Case1 (200X), (B) Case2 (200X), (C) Case3 (200X).
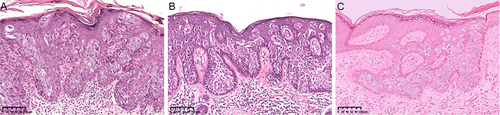
Figure 2 Immunohistochemical stain: We highlight the immunohistochemical staining of case 3. CK5/6 was positive for intact membrane, P63 was positive for nucleation, and CEA was negative. (A) CK5/6+ (200X), (B) P63+ (200X), (C) CEA- (200X).
Discussion
Pagetoid SCC in situ is a particular type of SCC, accounting for approximately 5% of SCC cases.Citation10 In combination with several relevant case reports similar to ours (), we concluded that the age of onset of pagetoid SCC in situ was middle-aged or older, there was no obvious sex preference and the incidence sites were generally non-illuminated.Citation11 These conclusions are similar to the description in the World Health Organization publication Pathology and Genetics of Skin Tumours.Citation12 The main complaint of the patient generally starts with erythema with pruritus, and after 1–2 years, the patient visits the doctor because the lesion has enlarged. As of June 2023, none of the three patients we followed had tumour recurrence or metastasis.
Table 1 Summary of Information and Immunohistochemical Stains of Patients with Pagetoid Squamous Cell Carcinoma
Combined with the preliminary clinical diagnosis, pagetoid SCC in situ is considered by dermatologists to be a benign skin tumour, seborrheic keratosis (SK) or basal cell carcinoma. Because the disease has no specific features in clinical manifestations or gross diagnosis, clinicians cannot provide an accurate diagnosis. Most cases are easy to diagnose through HE staining, and cases requiring IHC staining are typically exceptional. Specific information should also be provided, especially as the images only allow for focal histological visualisation. Without the relevant IHC markers, misdiagnosis is common. Pagetoid cells in pagetoid SCC in situ express EMA, CK5/6 and p63 but not CEA, CK8 or S-100. Moreover, HER2 and RANKL are markers that are expressed in pagetoid SCC in situ but not in EMPD or melanoma. In this study, microscopic examination showed epidermal hyperkeratosis, partial keratinisation, spinal hypertrophy and numerous nested pagetoid cells throughout the thickness, which resembled EMPD cell morphology, but pagetoid SCC in situ expressed CK5/6, p63 and EMA, as revealed by IHC staining. Therefore, the staining of these markers can confirm the diagnosis of pagetoid SCC in situ and guide the selection of the appropriate treatment. These IHC markers can help doctors achieve the correct diagnosis. Squamous cell carcinoma of the skin in situ is a precancerous condition that can progress to invasive SCC if left untreated and usually presents as erythematous, scaly patches or plaque on sun-exposed areas of the skin, such as the face, neck and limbs. However, SCC in situ can also occur in non-sun-exposed areas, such as the genitalia, anus and nipple–areola complex. In these locations, SCC in situ can mimic other skin diseases, such as EMPD, which is a rare malignancy of the apocrine glands. Extramammary Paget’s disease and SCC in situ can both show a pagetoid spread of atypical cells within the epidermis, which can cause diagnostic confusion. Therefore, it is important to distinguish these two entities by using IHC markers, such as CK7, CK5/6, EMA, CEA and p63.Citation2,Citation24 Pagetoid SCC in situ is an important differential diagnosis that should be distinguished from other skin diseases, such as EMPD, by using IHC markers. Human papillomavirus can play a role in promoting cancer, especially HPV16 and HPV18.Citation25–27 Infection with certain types of HPV appears to increase the risk of SCC but not basal cell carcinoma of the skin. However, the exact mechanism by which HPV contributes to the development of SCC is not fully understood. The prognosis of SCC depends on various factors, such as the stage of the cancer, size and location of the tumour, depth of invasion, presence of metastasis and the patient’s age and overall health; SCC that has not metastasised has a better prognosis than SCC that has metastasised.Citation28
We need to identify the following tumours:
1. Extramammary Paget Disease Accompanied by SCC in situ
2. Pagetoid Melanoma in situ
3. Clear Cell Acanthoma
4. Basal Cell Carcinoma
5. Seborrheic Keratosis
6. Intraepidermal Merkel Cell Carcinoma
Limitations
However, there are some limitations of this case report. In this study, there was a lack of long-term follow-ups; we only followed the patients until June 2023, which may not be enough to assess this tumour’s recurrence and metastasis rates. A longer follow-up period would be more informative. Furthermore, the case number was small, and monitoring additional similar cases in our clinical practice would be beneficial.
Conclusion
Pagetoid SCC in situ is a particular type of SCC. The initial clinical consideration and final pathological findings of the three cases in this report are inconsistent, indicating that the disease is non-specific in symptoms and gross manifestations, and the definitive diagnosis depends on histopathological and IHC staining. Therefore, diagnosis and treatment require special attention.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethical Approval
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of Affiliated Jinhua Hospital, Zhejiang University School of Medicine. Signed informed consent was obtained from three participants.
Consent Statement
Informed consent was provided by the patients for publication of the case.
Disclosure
The authors declare no competing interests in this work.
Additional information
Funding
References
- Matsumoto AJ, Schmitt AR, Skelley LM, et al. Factors influencing squamous cell carcinoma in situ recurrence and implications for treatment choice. Dermatol Surg. 2018;44(5):613–620. doi:10.1097/DSS.0000000000001400
- Stewart JR, Lang ME, Brewer JD. Efficacy of nonexcisional treatment modalities for superficially invasive and in situ squamous cell carcinoma: a systematic review and meta-analysis. J Am Acad Dermatol. 2022;87(1):131–137. doi:10.1016/j.jaad.2021.07.067
- Wieland R, Adhikari P, North J. The utility of p63, CK7, and CAM5.2 staining in differentiating pagetoid intraepidermal carcinomas. J Cutan Pathol. 2023;50(12):1110–1115. doi:10.1111/cup.14446
- Armes JE, Lourie R, Bowlay G, Tabrizi S. Pagetoid squamous cell carcinoma in situ of the vulva: comparison with extramammary paget disease and nonpagetoid squamous cell neoplasia. Int J Gynecol Pathol. 2008;27(1):118–124. doi:10.1097/pgp.0b013e318142acf0
- Wong J, Pina A, Mayrand M-H, Rahimi K. Pagetoid squamous intraepithelial neoplasia of the vulva as a mimicker of vulvar extramammary paget disease: two cases with basal layer sparing. Int J Surg Pathol. 2023;31(7):1302–1307.
- Chen IY, Bartell N, Ettel MG. Diffuse pagetoid squamous cell carcinoma in situ of the esophagus: a rare case report and review of literature. Int J Surg Pathol. 2022;30(3):326–330. doi:10.1177/10668969211046814
- Ishizuki S, Nakamura Y. Extramammary paget’s disease: diagnosis, pathogenesis, and treatment with focus on recent developments. Curr Oncol. 2021;28(4):2969–2986. (). doi:10.3390/curroncol28040260
- Firnhaber JM. Basal cell and cutaneous squamous cell carcinomas: diagnosis and treatment. Am Fam Physician. 2020;102(6):339–346.
- Cho WC, Ding Q, Wang W-L, et al. Immunohistochemical expression of TRPS1 in mammary Paget disease, extramammary Paget disease, and their close histopathologic mimics. J Cutan Pathol. 2023;50(5):434–440. doi:10.1111/cup.14414
- Ricci C, Dika E, Di Nanni DD, et al. Could EMA and cytokeratin 7 be useful in distinguishing tricholemmal carcinoma from clear-cell squamous cell carcinoma? A case series from our department and a brief review of the literature. Acta Histochem. 2019;121(6):765–767. doi:10.1016/j.acthis.2019.06.002
- Nasimi M, Azizpour A, Nikoo A, et al. Acantholytic and pagetoid variant of bowen’s disease with microinvasion on the scalp of a young female patient: a case report. Iran J Med Sci. 2019;44(6):511–514. doi:10.30476/ijms.2019.45771
- Vallacchi V, Vergani E, Cossa M, et al. Multistep tumor genetic evolution and changes in immunogenicity trigger immune-mediated disease eradication in stage IV melanoma: lessons from a single case. J Immuno Therap Canc. 2024;12(1):e007612. doi:10.1136/jitc-2023-007612
- Jae-Ho L, Soo-Kyung L, Joong-Ho K, et al. Focal CK7 positivity in pagetoid Bowen’s Disease: a mimic of extramammary Paget’s Disease. Dermatol. 2021;33(5):470–472.
- Ting W, Meng X, Yonghua T, et al. A case of clear cell Bowen’s disease. J Dermatol Venereol. 2019;26(4):236–237, 246.
- Jaewon L, Minwoo K, Jungyoon M, et al. Pagetoid Bowen Disease initially misdiagnosed as ectopic extramammary Paget’s Disease. Ann Dermatol. 2018;30:218–221. doi:10.5021/ad.2018.30.2.218
- Wang Wei, Zhou Guizhi, Zhao Fengying, et al. A case of paget-like Bowen’s disease. Chin J Leprosy Dermatol. 2016;32(04):231.
- Gao Y, SongNing J, Yuan X, et al. A case of paget-Like Bowen’s disease. A case of paget-like Bowen’s disease. Chin J Leprosy Skin Diseases. 2011;27(02):135–136.
- Zhigang W, Yanguo Z, Kaijun W, et al. A case of paget-like Bowen’s disease between the toes. Chin J Leprosy Dermatol. 2010;26(12):867–868.
- Han Haicheng,Wang Junmin,Liu Yan. A case of paget-like squamous cell carcinoma in situ. Chin J Dermatol Venereol. 2009;23(04):233–234.
- Xu Jia,Gulidariha Bodhi,Wang Ping.A case of paget-like Bowen’s disease. Chin J Dermatol Venereol. 2009;23(06):369–370.
- Congjungle C. Report of a case of Paget’s disease. Chin J Misdiagnosis. 2008;(01):15–17.
- Limin L, Xiaohong M, Kejian Z, et al. A case report of Paget’s disease. Chin J Dermatol Venereol. 2006;(02):102–103.
- Hongzhong J, Jiabi W. Paget’s disease. J Clinic Dermatol. 2004;(06):391–392.
- Barrutia L, Martinez-Garcia G, Santamarina-Albertos A, et al. Differentiating pagetoid Bowen disease from paget disease on the nipple-areola complex: two unique, challenging cases. J Cutan Pathol. 2021;48(11):1416–1422. doi:10.1111/cup.14092
- Malagutti N, Rotondo JC, Cerritelli L, et al. High Human Papillomavirus DNA loads in Inflammatory Middle Ear Diseases. Pathogens. 2020;9(3):224.
- Shimizu A, Yamaguchi R, Kuriyama Y. Recent advances in cutaneous HPV infection. J Dermatol. 2023;50(3):290–298. doi:10.1111/1346-8138.16697
- Chen M-L, Wang S-H, Wei J-C-C, et al. The impact of human papillomavirus infection on skin cancer: a population-based cohort study. Oncologist. 2021;26(3):e473–e483. doi:10.1002/onco.13593
- Fang Q, Wu J, Liu F. Oncologic outcome and potential prognostic factors in primary squamous cell carcinoma of the parotid gland. BMC Cancer. 2019;19(19):752. doi:10.1186/s12885-019-5969-6
- Miraflor AP, LeBoit PE, Hirschman SA. Intraepidermal Merkel cell carcinoma with pagetoid Bowen’s disease. J Cutaneous Pathology. 2016;43(11):921–926. doi:10.1111/cup.12813