
Abstract
Purpose
A surge in the use of semaglutide injection (Ozempic®) approved to treat type 2 diabetes (T2D) has led to a global supply shortage. We investigated contemporary user rates and clinical characteristics of semaglutide (Ozempic®) users in Denmark, and the extent of “off-label” prescribing for weight loss.
Patients and Methods
Nationwide population-based cross-sectional study based on linked health registries January 2018 through December 2023. All adults who received a first prescription of semaglutide once weekly (Ozempic®) were included. We examined quarterly rates of new users and total user prevalences, using other glucagon-like peptide-1 receptor agonists and weight loss medications as comparison. We also investigated user characteristics including T2D, glucose control, comedications, and cardiorenal disease.
Results
The new user rate of semaglutide (Ozempic®) remained stable at approximately 4 per 1000 adult person-years between 2019 and 2021 and then accelerated, peaking at 10 per 1000 in the first quarter of 2023 after which it declined sharply. User prevalence increased to 91,626 users in Denmark in 2023. The proportion of semaglutide (Ozempic®) new users who had a record of T2D declined from 99% in 2018 to only 67% in 2022, increasing again to 87% in 2023. Among people with T2D who initiated semaglutide (Ozempic®) in 2023, 52% received antidiabetic polytherapy before initiation, 39% monotherapy, and 8% no antidiabetic therapy. Most T2D initiators had suboptimal glucose control, with 83% having an HbA1c ≥48 mmol/mol and 68% ≥53 mmol/mol despite use of antidiabetic medication, and 29% had established atherosclerotic cardiovascular disease or kidney disease.
Conclusion
The use of semaglutide (Ozempic®) in Denmark has increased dramatically. Although not approved for weight loss without T2D, one-third of new users in 2022 did not have T2D. Conversely, most initiators with T2D had a clear medical indication for treatment intensification, and “off-label” use can only explain a minor part of the supply shortage.
Introduction
Worldwide the prevalence of obesity and type 2 diabetes (T2D) is high and rapidly increasing.Citation1 Substantial progress has been made over the past decade in the pharmacological management of T2D,Citation2,Citation3 and recently also obesity.Citation4,Citation5 In developed countries, new classes of organ-protective glucose-lowering drugs, including glucagon-like peptide-1 receptor agonists (GLP-1RAs) and sodium-glucose co-transporter-2 inhibitors (SGLT-2i), have now become central to the treatment of T2D.Citation2,Citation3
Despite being developed to treat hyperglycemia in T2D, GLP-1RAs at high doses have clinically significant effects on body weight in people with obesity.Citation4 Consequently, several GLP-1RA injections are presently approved to treat T2D at a single recommended maintenance dose, and simultaneously licensed for treating obesity, but at a higher recommended maintenance dose. For instance, semaglutide injection at 1.0 mg once weekly (marketed as Ozempic®) and liraglutide injection 1.2 or 1.8 mg once daily (sold as Victoza®) are approved for T2D treatment, whereas semaglutide injection 2.4 mg once weekly (sold as Wegovy®) and liraglutide injection 3.0 mg once daily (sold as Saxenda®) are approved for treating obesity.Citation4,Citation5 Moreover, there is now randomized trial evidence for effectiveness of GLP-1RAs in secondary prevention of cardiovascular disease,Citation6 not only in patients with T2D,Citation7–9 but also in overweight or obese patients without diabetes.Citation10
A surge in the use of semaglutide injection (Ozempic®) has occurred in many countries since 2022, creating a global supply shortage.Citation11 Therefore, some people living with T2D who could benefit from semaglutide (Ozempic®) are currently unable to access this treatment. This clinical and public health problem is currently debated among patient organizations, healthcare providers, authorities, experts, and media outlets in many countries.Citation12 The increase in semaglutide consumption is thought to be associated with “off-label” prescribing of semaglutide (Ozempic®) for weight loss in people without T2D,Citation13 fueled by social media interest (which some have dubbed “Ozempic craze”)Citation14 and the current lack of licensing - or reimbursement - of higher-dose incretin-based therapies specifically for weight loss in many countries.
Data are needed at the level of individual users to reveal current trends in semaglutide initiation and use across healthcare systems. In Denmark, semaglutide (Ozempic®) for T2D treatment is currently covered by Denmark’s tax-financed drug reimbursement scheme,Citation15 with minimal co-payment. In contrast, semaglutide (Ozempic®) use for treatment of obesity rather than T2D, as well as all dosages of semaglutide injection licensed solely for the treatment of obesity, ie, Wegovy®, licensed in Denmark since December 2022, are not generally reimbursed. Only in very rare cases will patients receive some reimbursement for this indication.Citation16 Semaglutide (Ozempic®) is a costly medication, and its subsidies are currently placing high economic pressure on the Danish National Health Service.Citation17 It has therefore been debated to what extent the “right” patients, ie, those with T2D and a guideline-supported need for semaglutide injection, receive semaglutide (Ozempic®),Citation17 yet exact data on “off-label” prescribing and user characteristics are scarce.
To address these knowledge gaps, we conducted a nationwide cross-sectional drug utilization study based on Denmark’s entire population using data from linked national Danish registries from 2018 through 2023. Our first aim was to evaluate current patterns of use of semaglutide (Ozempic®) in Denmark. We compared the trends with those for other frequently used GLP-1RAs in Denmark, ie, GLP-1RAs for T2D (including liraglutide (Victoza®) and oral semaglutide (Rybelsus®)) and GLP-1RAs for obesity (liraglutide (Saxenda®) and semaglutide (Wegovy®)). The use of lixisenatide, exenatide, and dulaglutide in Denmark during the study period was negligeable.Citation18 As a point of reference, we also described the trends in use of older weight-loss drugs. Our second aim was to investigate changing trends in the profiles of semaglutide (Ozempic®) users, with a special focus on the presence of T2D.
Material and Methods
Setting and Data Sources
Denmark has six million inhabitants and a well-integrated tax-financed nationwide healthcare system covering the whole population, with comprehensive individual-level registry information available on morbidity and medication use. Based on nationwide data from the Register of Medicinal Products Statistics covering all Danish pharmacies,Citation15 we identified all people in Denmark with a new incident prescription dispense for semaglutide once-weekly injection (Ozempic®). This drug was approved to treat T2D and licensed in Denmark in 2018. We linked the data with individual-level information on co-medications, demographics, comorbidities, and laboratory data obtained from the Register of Medicinal Products Statistics, the Danish Civil Registration System, the Danish National Patient Registry, and the Register of Laboratory Results for Research.Citation15,Citation19 Codes used for medications, diagnoses, procedures, and laboratory tests are shown in Supplementary Table 1.
Analysis of User Trends
We first examined trends in new user rates of semaglutide (Ozempic®) initiation per quarter by dividing the number of new users in each quarter by the estimated person-time at risk in that quarter (presented in person-years). New use was for each medication defined as filling a first prescription for the medication with a three-year look-back period. The prevalence proportion of semaglutide (Ozempic®) users per quarter was estimated as the number of people who had at least one drug prescription filled within the period. For comparison, we also examined the new user and prevalence trends for other GLP-1RAs in Denmark during 2018–2023. These drugs included GLP-1RAs approved for T2D treatment (ie, liraglutide injection once daily with recommended maintenance dose 1.2 or 1.8 mg (Victoza®, licensed in 2009), and semaglutide oral 7 mg once daily (Rybelsus®, licensed in 2020) as well as GLP-1RAs approved specifically for weight loss,Citation5,Citation20 including liraglutide injection once daily with recommended maintenance dose 3.0 mg (Saxenda®, licensed in 2016), and semaglutide injection once weekly with recommended maintenance dose 2.4 mg (Wegovy®, licensed in December 2022). For reference, we also examined trends for “older” weight loss medications in Denmark on a group level, ie, orlistat (Orlistat®, Xenical®, Alli®), bupropion-naltrexone (Mysimba®), and amfepramone (Regenon®, Regenon Retard®).Citation5,Citation20
Analyses of User Characteristics
Next, we examined changes in the characteristics of semaglutide (Ozempic®) users over time, focusing on the presence or absence of any indicators of T2D and related characteristics. Diabetes indicators included HbA1c test results from primary care and hospitals,Citation21 previous antidiabetic (glucose-lowering) medication use (excluding GLP-1RAs approved specifically for weight loss), and/or previous diabetes diagnoses from hospital contacts, in the annual new (January 2018–December 2023) and prevalent (2023) semaglutide user populations. Among people initiating semaglutide (Ozempic®) who had a record of T2D, we further described the number and type of prior antidiabetic medications used within the last year, the most recent HbA1c value measured within the last year, and the presence of established hospital-diagnosed atherosclerotic cardiovascular disease (ASCVD) or kidney disease at the time of semaglutide (Ozempic®) initiation. Suboptimal glucose control was defined by glycated hemoglobin (HbA1c) ≥48 mmol/mol and use of another antidiabetic medication at the time of first semaglutide (Ozempic®) initiation.Citation3,Citation22 In a second analysis, we used an HbA1c target ≥53 mmol/mol and use of another antidiabetic medication to define suboptimal control.Citation3,Citation22 All statistical analyses were conducted using SAS V.9.4 (SAS Institute).
Results
Semaglutide (Ozempic®) New User Rates
Panel A of shows the rate of new users of semaglutide injection (Ozempic®), compared with other GLP-1RAs and with “older” weight loss medications, per 1000 person-years among all Danish adults in each quarter from January 1, 2018, to December 31, 2023. The semaglutide (Ozempic®) initiation incidence increased from its license in 2018 to stable values of approximately four initiators per 1000 person-years during 2019 and 2020, after which the incidence began to further increase. A notable acceleration was observed from the end of 2021 onward with an incidence reaching 10 per 1000 person-years in the first quarter of 2023, after which the incidence declined sharply towards the end of the study period. Among the other GLP-1RAs with a T2D indication, the initiation incidence for liraglutide injection (Victoza®) declined after mid-2018, when semaglutide (Ozempic®) was approved. Semaglutide oral (Rybelsus®) had an initiation incidence of two to three per 1000 person-years since it was approved in 2020 with a slightly declining trend up to the beginning of 2023. During 2023, a marked increase in semaglutide oral (Rybelsus®) new use was observed, concurrent with the marked decrease in semaglutide (Ozempic®) new use in 2023.
Figure 1 Quarterly incidence rate of new users (A) and quarterly total user prevalence (B) of semaglutide injection (Ozempic®) in Denmark, 2018–2023. Use of other GLP-1RAs and older weight loss medications shown as comparison.
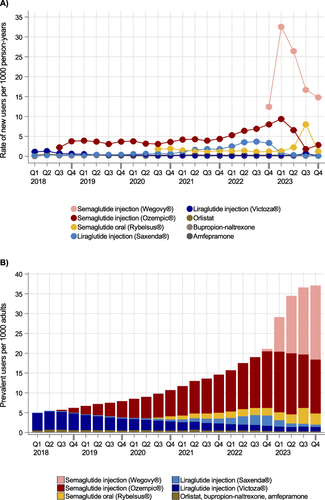
The initiation incidence of the “older” weight loss medications (orlistat, bupropion/naltrexone, and amfepramone) remained at a very low level throughout the study period ( Panel A). Among the newer weight loss medications, the initiation incidence of liraglutide injection (Saxenda®) remained fairly low from 2018 to 2020. Liraglutide (Saxenda®) new use increased during 2021–2022, with the increase beginning slightly before the rise in semaglutide (Ozempic®) initiation rates, peaking at a rate of four per 1000 person-years in the third quarter of 2022 and rapidly declining again thereafter, concurrent with the licensing of semaglutide injection (Wegovy®). The initiation incidence of semaglutide injection (Wegovy®) started off at 12 per 1000 person-years in the last quarter of 2022, when the drug entered the market. New user rates reached a maximum of 32 per 1000 person-years in the first quarter of 2023, and then declined again to 15 per 1000 person-years in the last quarter of 2023 ( Panel A).
Prevalence of Semaglutide (Ozempic®) Users
Panel B of shows a substantial increase in the total prevalence proportion of all Danish adults using semaglutide (Ozempic®), from two per 1000 adults in 2018 to 19 per 1000 adults in 2023, corresponding to an almost ten-fold increase. In comparison, regarding the other GLP-1RAs with a T2D indication, the prevalence of liraglutide (Victoza®) users markedly declined, from five per 1000 adults using the medication in 2018, and to only two per 1000 in 2023, while the prevalence of semaglutide oral (Rybelsus®) increased in 2023. The total user prevalence for the older weight loss drugs remained low. The user prevalence of newer GLP-1RA weight loss drugs increased steadily in the most recent years, first driven by increased use of liraglutide (Saxenda®) starting in late 2020 and peaking in late 2022, and afterwards driven by a rapid increase in semaglutide (Wegovy®) use, reaching a similar number of users than semaglutide (Ozempic®) during 2023 ( Panel A).
Characteristics of Semaglutide (Ozempic®) Users
Overall Characteristics and Occurrence of Diabetes
shows the characteristics of people initiating semaglutide (Ozempic®). The prevalence proportion of female (Ozempic®) initiators increased from 42% in 2018 to a high 55% in 2022, falling again to 48% in 2023. The median age at initiation decreased by five years, from 62 years in 2018 to 57 years in 2022, then increasing to 60 years in 2023. In 2018, the proportion of new semaglutide (Ozempic®) users who had any indication of diabetes ever before semaglutide (Ozempic®) initiation was 99%, including 99% who had used another antidiabetic medication before semaglutide (Ozempic®) initiation, 98% who had an HbA1c level ≥48 mmol/mol registered, and 83% who had a previous hospital diagnosis of diabetes recorded. By 2022, the prevalence proportion of new users with any indication of diabetes had decreased substantially to a low 67%, including 65% that had ever used another antidiabetic medication, 63% who had an HbA1c level ≥48 mmol/mol, and 36% who had a previous hospital diagnosis of diabetes. In 2023, the proportion having diabetes clearly increased again, to 87%.
Table 1 Characteristics of All New Initiators of Semaglutide Injection (Ozempic®) in Denmark from January 2018 to December 2023, and Characteristics of Prevalent Users in 2023
Table 2 Characteristics of patients with a record of diabetes who initiated semaglutide injection (Ozempic®) from January 2018 to December 2023 or were prevalent users in 2023
Characteristics in People with T2D
shows the characteristics of the people with a record of T2D who initiated semaglutide (Ozempic®). Among semaglutide (Ozempic®) new users in 2023, 52% received antidiabetic glucose-lowering polytherapy (31% dual and 21% three or more medications), 39% received monotherapy, and 8% received no antidiabetic medication before they initiated semaglutide (Ozempic®). The data suggested a gradually earlier use of semaglutide (Ozempic®) in the course of T2D therapy, ie, moving from a typical third- or fourth-line glucose-lowering medication in 2018–2020 to a frequent second-line and sometime first-line medication by 2023 (). Among new users in 2023, 83% had suboptimal glucose control, as evidenced by the use of another glucose-lowering medication and an HbA1c level ≥48 mmol/mol within the prior year. When applying a less strict HbA1c target of ≥53 mmol/mol and use of another glucose-lowering medication, 68% initiators of semaglutide (Ozempic®) had suboptimal glucose control. A hospital history of either established ASCVD (24%) and/or kidney disease (8%) was observed in a total of 29% of these individuals.
Discussion
Key Results
In this nationwide population-based study of semaglutide (Ozempic®) utilization in Denmark, we observed a sharp increase in use in 2021–2022, with a falling incidence in 2023. Even though semaglutide (Ozempic®), is not approved for weight loss in people without T2D, 12% of all prevalent users in 2023 did not have T2D. A high 33% of people who were new users in 2022 did not have T2D at their drug initiation, but the proportion without T2D recently decreased again to 13% of new users in 2023. Among new users with T2D in 2023, between 68% and 83% had a clear medical indication for glucose-lowering medication intensification, depending on the level of HbA1c accepted. Our findings suggest that in Denmark, there was a clear increase in semaglutide (Ozempic®) “off-label” use through 2022, however, of a magnitude that can explain only a minor part of the drug shortage, and with a decreasing “off-label” user trend observed in 2023.
Strengths and Limitations
The main strengths of our study are its population-based setting with uniform access to healthcare for all citizens; the complete registration of high-quality prescription data through nationwide monopolized community pharmacies;Citation15,Citation19 and the availability of individual-level data on comorbidities, comedications, and glucose control.Citation21
Study limitations include lack of data on the exact medical indication for physicians prescribing semaglutide (Ozempic®) or other medications, as only diagnoses made during hospital contacts are available for research purposes. However, as we also leveraged primary care testing of HbA1c, we expect to correctly identify individuals with T2D prior to treatment initiation. The very high proportions (>95%) of semaglutide (Ozempic®) initiators who had T2D recorded during the first three study years also support that the chosen indicators of T2D, when present, are not systematically under-recorded in our data sources. Another limitation is that we were unable to make inferences about the use of other GLP-1RAs including lixisenatide, exenatide, and dulaglutide, as the uptake of these three drugs has been very low in Denmark, with only around 1000 prevalent users combined in 2022.Citation18
Interpretation
A major finding was that the proportion of people who initiated semaglutide (Ozempic®) approved for T2D but who did not have a record of T2D (ie, “off-label” use) increased from close to 0% during 2018–2020 to one-third in 2022. It is likely that, before semaglutide injection (Wegovy®) approved for weight loss became available in Denmark in December 2022, obese people without T2D have asked physicians to prescribe semaglutide injection (Ozempic®) although this use does not accord with Danish clinical guidelines.Citation22 It is also likely that the licensing of semaglutide injection (Wegovy®) is related to the apparent decrease in “off-label” use of semaglutide (Ozempic®) during 2023. Tirzepatide, a dual GIP/GLP-1 receptor agonist with even greater effectiveness on glycemia and weight loss than semaglutide,Citation23,Citation24 received marketing authorization for diabetes treatment (Mounjaro®) in the European Union in 2022,Citation25 but is not yet available on the Danish market; the introduction of tirzepatide can therefore not explain any changes in the demand for semaglutide observed in this study. A recent Norwegian study documented clear increases in the adult population use of drugs to treat obesity from 2017 to 2022.Citation26 The authors reported a sharp increase in the use of semaglutide injection (Ozempic®) without reimbursement (i.e, “off-label” use) from 2021 to 2022, corroborating our findings in Denmark. In contrast to our results, the use of bupropion-naltrexone in Norway was high with substantial increases in recent years, probably due to more generous reimbursement rules than in Denmark.
The proportion of adults having obesity (body mass index ≥30) is currently 19% in the Danish general population,Citation27 slightly below the average level of 23% in the World Health Organization European Region,Citation28 whereas 42% of adults in the United States are now obese.Citation29 In comparison, 7% of adults in DenmarkCitation30 and 11% in the United StatesCitation31 are currently diagnosed with T2D. For both obesity and T2D, weight loss is a key clinical guideline recommendation since weight reduction improves metabolic risk factors for future complications.Citation3,Citation28,Citation32 In addition, many overweight people wish to lose weight since obesity may be associated with societal stigma and perceived unattractiveness.Citation33
The significant weight loss potential of semaglutideCitation9,Citation34 has been widely disseminated by social and mainstream media with global outreach, by mouth to mouth, and, in some countries, by direct-to-consumer prescription drug advertising.Citation12–14 Indeed, many primary care physicians report strongly increasing demands from their patients, and it is well-known that such pressure can lead to inappropriate prescribing patterns.Citation35
Finally, costs of semaglutide may play a role. Even in a homogeneous and equal society such as Denmark, obesity is twice as prevalent in socioeconomically disadvantaged groups compared with among people with high income.Citation27 Patients putting pressure on physicians to prescribe a reimbursed/subsidized medication such as semaglutide (Ozempic®) can be expected. Based on data from Danish health authorities, the number of users of semaglutide (Ozempic®) prescriptions who did not receive reimbursement/subsidies in Denmark in 2022 was relatively small, ie, in the order of 15% to 20% of all users,Citation36,Citation37 and thus in the same order as the proportion who did not have T2D in 2022 in our study.
The marked increase in the number of patients with T2D using semaglutide (Ozempic®) generally aligns with consecutively updated clinical guidelines on T2D management.Citation3,Citation22 Since 2015, numerous large cardiovascular outcome trials have shown that GLP-1RAs including semaglutide reduce cardiovascular and renal complications in high-risk T2D patients and confer organ-protective effects beyond lowering glucose.Citation38 These studies have led to guideline changes, in which GLP-1RA and SGLT-2i are now preferred glucose-lowering drugs (regardless of HbA1c level) in T2D patients with established cardiovascular disease or renal disease and are preferred second-line medications in patients at high cardiovascular risk,Citation3,Citation22 i,e, patient groups that may constitute over a third of all people with T2D.Citation39 Furthermore, clinical T2D guidelines emphasize individualized therapy, in which the choice of glucose-lowering therapy should include considerations about glucose-reducing effects, desired weight loss, side effects, costs, and patient preferences.Citation3,Citation22
The high proportion of people with T2D with a clear clinical indication for treatment initiation (ie, a need for intensification of glucose-lowering medication, as evidenced by increased HbA1c, and/or the presence of ASCVD or kidney disease) suggests rational pharmacotherapeutic practices by the prescribing physicians. We have previously observed that GLP-1RA and SGLT-2i prescriptions are being initiated increasingly by general practitioners in addition to hospital-based physicians.Citation2 This accords with recommendations that most patients with T2D can receive high-quality care in general practice.Citation2 Notwithstanding, there is a current debate whether the use of GLP-1RA in Danish T2D patients is too high and may happen too early in the therapy line.Citation37,Citation40,Citation41
Unanswered Questions and Future Research
A substantial proportion of the adult populations in most countries might currently be candidates for semaglutide and other pharmacological weight loss therapies. This carries major implications for healthcare costs. An important future task will be to identify the most appropriate target groups to ensure cost-effective therapy. As stated above, semaglutide (Ozempic®) has documented effects in secondary prevention of cardiovascular disease in T2D patients with established cardiovascular disease.Citation9 Moreover, an effect of semaglutide (Wegovy®) in secondary prevention of cardiovascular disease was recently proven also in overweight or obese patients with established cardiovascular disease.Citation10 In contrast, there is less clear evidence for an effectiveness of GLP-1RA on primary prevention of cardiovascular disease, both for T2DCitation42 and obesity, although there is some indication that GLP-1RAs may reduce cardiovascular outcomes in people with T2D and multiple cardiovascular risk factors,Citation8 reflected in “Class IIb”, “Level C” recommendations in the most recent European Society of Cardiology guidelines.Citation6 There is also no evidence yet for long-term sustainable weight loss with GLP-1RA after the first one to two years,Citation5 with the STEP-4 trial showing that patients unfortunately regain weight quickly when discontinuing semaglutide injection.Citation43 Finally, possible long-term adverse effects of high-dose semaglutide injection therapy remain to be clarified.Citation5,Citation16 Future routine clinical care studies should therefore follow the many new users of semaglutide and other incretin-based medications to investigate the adherence, safety, and effectiveness of these medications in a real-world setting.
Conclusion
In conclusion, the use of semaglutide injection (Ozempic®) in Denmark has increased dramatically. Although semaglutide (Ozempic®) is not approved for weight loss in people without T2D in Denmark, by 2022, one-third of new users did not have T2D. The amount of “off-label” medication initiation seems to be on the decline in 2023, and it cannot alone explain the current supply shortage. Most initiators who had T2D also had a clear medical indication for intensification of glucose-lowering medication, based on glucose levels and/or comorbidities.
Ethics Approval and Informed Consent
The study was approved by the Danish Data Protection Agency. According to Danish legislation, no approval from an ethics committee or informed consent from patients is required for studies based entirely on registry data.
Data Sharing Statement
Data are available as presented in the paper and in the Supporting Information files. Danish legislation does not allow us to distribute or make individual-level patient data directly available to other parties. Authorized researchers may apply for data access through the Research Service at the Danish Health Data Authority (e-mail: [email protected]). Up-to-date information on data access is available online (http://sundhedsdatastyrelsen.dk/da/forskerservice). Access to data from the Danish Health Data Authority requires approval from the Danish Data Protection Agency (https://www.datatilsynet.dk/english/the-danish-data-protection-agency/introduction-to-the-danish-data-protection-agency/).
Disclosure
Professor Anton Pottegård reports grants from Novo Nordisk, outside the submitted work. Professor Jens Søndergaard reports grants from Roche Diagnostics, AstraZeneca a/s; personal fees from Novo Nordisk a/s, Abbott Rapid Diagnostics a/s, outside the submitted work. The authors report no other conflicts of interest in this work.
Acknowledgments
The Department of Clinical Epidemiology, Aarhus University and Aarhus University Hospital is a member of The Danish Centre for Strategic Research in Type 2 Diabetes (DD2), supported by the Danish Agency for Science (grant nos. 09-067009 and 09-075724), the Danish Health and Medicines Authority, the Danish Diabetes Association, and The Novo Nordisk Foundation. Project partners are listed on the website http://www.DD2.dk. The Department of Clinical Epidemiology, Aarhus University and University Hospital, receives funding for other studies from EMA and companies in the form of research grants to (and administered by) Aarhus University. None of these studies have any relation to the present study.
Additional information
Funding
References
- World Health Organization. Obesity and overweight. June 9, 2021. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
- Pottegård A, Andersen JH, Søndergaard J, Thomsen RW, Vilsbøll T. Changes in the use of glucose-lowering drugs: a Danish nationwide study. Diabetes Obes Metab. 2023;1‐9. doi:10.1111/dom.14947
- Davies MJ, Aroda VR, Collins BS, et al. Management of hyperglycemia in type 2 diabetes, 2022. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2022;45(11):2753–2786. doi:10.2337/dci22-0034
- Andreasen CR, Andersen A, Vilsbøll T. The future of incretins in the treatment of obesity and non-alcoholic fatty liver disease. Diabetologia. 2023;66(10):1846–1858. doi:10.1007/s00125-023-05966-9
- Müller TD, Blüher M, Tschöp MH, DiMarchi RD. Anti-obesity drug discovery: advances and challenges. Nat Rev Drug Discov. 2022;21(3):201–223. doi:10.1038/s41573-021-00337-8
- Marx N, Federici M, Schütt K, et al. ESC Guidelines for the management of cardiovascular disease in patients with diabetes. Eur Heart J. 2023;44(39):4043–4140. doi:10.1093/eurheartj/ehad192
- Marso SP, Daniels GH, Brown-Frandsen K, et al. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2016;375(4):311–322. doi:10.1056/NEJMoa1603827
- Gerstein HC, Colhoun HM, Dagenais GR, et al. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): a double-blind, randomised placebo-controlled trial. Lancet. 2019;394(10193):121–130. doi:10.1016/s0140-6736(19)31149-3
- Marso SP, Bain SC, Consoli A, et al. SUSTAIN-6 investigators. semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2016;375(19):1834–1844. doi:10.1056/NEJMoa1607141
- Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. SELECT trial investigators. semaglutide and cardiovascular outcomes in obesity without diabetes. N Engl J Med. 2023;389(24):2221–2232. doi:10.1056/NEJMoa2307563
- European Medicines Agency. Shortage of Ozempic. October 19, 2022. https://www.ema.europa.eu/en/documents/shortage/ozempic-semaglutide-supply-shortage_en.pdf.
- Diabetes UK Ozempic and weight loss: the facts behind the headlines. July 5, 2023. https://www.diabetes.org.uk/about_us/news/ozempic-and-weight-loss-facts-behind-headlines.
- ‘You forget to eat’: how ozempic went from diabetes medicine to blockbuster diet drug. National Public Radio (NPR), Washington, D.C. USA. April 1, 2023. https://www.npr.org/2023/04/01/1166781510/ozempic-weight-loss-drug-big-business.
- Awan O. The ozempic craze is sending the wrong public health message. Forbes magazine. July 5, 2023. https://www.forbes.com/sites/omerawan/2023/07/05/the-ozempic-craze-is-sending-the-wrong-public-health-message/.
- Pottegård A, Schmidt SAJ, Wallach-Kildemoes H, Sørensen HT, Hallas J, Schmidt M. Data resource profile: the Danish national prescription registry. Int J Epidemiol. 2017;46(3):798. doi:10.1093/ije/dyw213
- Danish Medicines Agency. No general reimbursement for wegovy [in Danish]. July 1, 2022. https://laegemiddelstyrelsen.dk/da/soeg/~/media/64ADE64831734B8CACEB40A476DE5B45.ashx.
- TV2 News. Danish Regions expect explosive increase in subsidies for expensive drugs: scary, expert says [in Danish]. August 9, 2023. https://nyheder.tv2.dk/samfund/2023-08-08-regioner-forventer-eksplosiv-stigning-i-tilskud-til-dyr-medicin-skraemmende-siger-ekspert.
- Danish Health Data Authority. medstat.dk.
- Schmidt M, Schmidt SAJ, Adelborg K, et al. The Danish health care system and epidemiological research: from health care contacts to database records. Clin Epidemiol. 2019;11:563–591. doi:10.2147/CLEP.S179083
- Iannone A, Natale P, Palmer SC, et al. Clinical outcomes associated with drugs for obesity and overweight: a systematic review and network meta-analysis of randomized controlled trials. Diabetes Obes Metab. 2023;25(9):2535–2544. doi:10.1111/dom
- Nicolaisen SK, Pedersen L, Witte DR, Sørensen HT, Thomsen RW. HbA1c-defined prediabetes and progression to type 2 diabetes in Denmark: a population-based study based on routine clinical care laboratory data. Diabetes Res Clin Pract. 2023;203:110829. doi:10.1016/j.diabres.2023.110829
- Danish Endocrine Society (DES)/The Danish College of General Practitioners (DSAM). Type 2 diabetes guidelines [Retningslinjer for den farmakologiske behandling af type 2-diabetes]. https://vejledninger.dsam.dk/fbv-t2dm/. Accessed April 15, 2024
- Karagiannis T, Avgerinos I, Liakos A, et al. Management of type 2 diabetes with the dual GIP/GLP-1 receptor agonist tirzepatide: a systematic review and meta-analysis. Diabetologia. 2022;65(8):1251–1261. doi:10.1007/s00125-022-05715-4
- Tan B, Pan XH, Chew HSJ, et al. Efficacy and safety of tirzepatide for treatment of overweight or obesity. A systematic review and meta-analysis. Int J Obes. 2023;47(8):677–685. doi:10.1038/s41366-023-01321-5
- European Medicines Agency. https://www.ema.europa.eu/en/medicines/human/EPAR/mounjaro. Accessed April 15, 2024
- Ruiz PL, Karlstad Ø, Nøkleby K, et al. Pharmacological treatment of obesity in adults in Norway 2004-2022. Diabetes Obes Metab. 2024. doi:10.1111/dom.15515
- Schramm S, Bramming M, Davidsen M, Rosendahl H, Tolstrup J Burden of disease in Denmark: risk factors [in Danish]. 2023. https://sundhedsstyrelsen.dk/-/media/Udgivelser/2023/Sygdomsbyrden-2023/Risikofaktorer-Sygdomsbyrden-2023.ashx. Accessed April 15, 2024
- World Health Organization European Regional Obesity Report 2022. Copenhagen: World Health Organization Regional Office for Europe; 2022.
- National Center for Health Statistics (U.S.). https://www.cdc.gov/nchs/data/nhsr/nhsr158-508.pdf. Accessed April 15, 2024
- Danish Diabetes Association. https://www.diabetestal.nu/. Accessed April 15, 2024
- Centers for Disease Control and Prevention. National diabetes statistics report website. https://www.cdc.gov/diabetes/data/statistics-report/index.html. Accessed April 15, 2024
- LeBlanc ES, Patnode CD, Webber EM, Redmond N, Rushkin M, O’Connor EA. Behavioral and pharmacotherapy weight loss interventions to prevent obesity-related morbidity and mortality in adults: updated evidence report and systematic review for the us preventive services task force. JAMA. 2018;320(11):1172–1191. doi:10.1001/jama.2018.7777
- Puhl RM, Heuer CA. Obesity stigma: important considerations for public health. Am J Public Health. 2010;100(6):1019–1028. doi:10.2105/AJPH.2009.159491
- Wilding JPH, Batterham RL, Calanna S, et al.; STEP 1 Study Group. Once-weekly semaglutide in adults with overweight or obesity. N Engl J Med. 2021;384(11):989–1002. doi:10.1056/NEJMoa2032183.
- Allen T, Gyrd-Hansen D, Kristensen SR, Oxholm AS, Pedersen LB, Pezzino M. Physicians under pressure: evidence from antibiotics prescribing in England. Med Decis Making. 2022;42(3):303–312. doi:10.1177/0272989X211069931
- Danish Health Data Authority. Medications for diabetes and overweight including wegovy flextouch [in Danish]. 2023. https://www.esundhed.dk/Emner/Laegemidler/Laegemidlermodovervaegt. Accessed April 15, 2024
- The Danish National Board of Health. The consumption of GLP-1 receptor agonists for the treatment of diabetes must decrease [In Danish]. 2023. https://www.sst.dk/da/nyheder/2023/Forbruget-af-GLP-1-receptor-agonister-til-behandling-af-diabetes-skal-ned. Accessed April 15, 2024
- Funck KL, Knudsen JS, Hansen TK, Thomsen RW, Grove EL. Real-world use of cardioprotective glucose-lowering drugs in patients with type 2 diabetes and cardiovascular disease: a Danish nationwide cohort study, 2012 to 2019. Diabetes Obes Metab. 2021;23(2):520–529. doi:10.1111/dom.14245
- Nargesi AA, Jeyashanmugaraja GP, Desai N, Lipska K, Krumholz H, Khera R. Contemporary national patterns of eligibility and use of novel cardioprotective antihyperglycemic agents in type 2 diabetes mellitus. J Am Heart Assoc. 2021;10(e021084). doi:10.1161/JAHA.121.021084
- Danish Medicines Agency. New proposal for subsidy status for diabetes medications submitted for hearing. [In Danish]. https://laegemiddelstyrelsen.dk/da/nyheder/2023/nyt-forslag-til-tilskudsstatus-for-diabetesmedicin-sendes-i-hoering/. Accessed April 15, 2024
- Danish Diabetes Association. The diabetes association is fighting to keep already issued subsidies for GLP-1 analogues. https://diabetes.dk/nyheder/2023/diabetesforeningen-kaemper-for-at-beholde-allerede-udstedte-tilskud-til-glp-1-analoger. Accessed April 15, 2024
- Mannucci E, Silverii GA. Cardiovascular prevention with glucose-lowering drugs in type 2 diabetes: an evidence-based approach to the categories of primary and secondary prevention. Diabetes Obes Metab. 2023;25(12):3435–3443. doi:10.1111/dom.15226
- Rubino D, Abrahamsson N, Davies M, et al. Effect of continued weekly subcutaneous semaglutide vs placebo on weight loss maintenance in adults with overweight or obesity: the STEP 4 randomized clinical trial. JAMA. 2021;325:1414. doi:10.1001/jama.2021.3224