
Abstract
Purpose
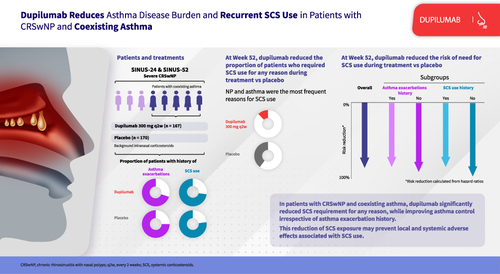
Dupilumab significantly reduced the requirement for systemic corticosteroids (SCS) in patients with severe chronic rhinosinusitis with nasal polyps (CRSwNP). Patients with CRSwNP and coexisting asthma typically have a higher disease burden and have more difficulty in managing disease. Here, we report an analysis of asthma outcomes and SCS use in patients with CRSwNP and coexisting asthma.
Patients and Methods
This was a post hoc analysis of the randomized, placebo-controlled SINUS-24 and SINUS-52 studies (NCT02912468/NCT02898454) in patients with severe CRSwNP and coexisting asthma (patient self-reported) from the pooled intention-to-treat population randomized to dupilumab 300 mg every 2 weeks or placebo. On-treatment SCS use was estimated using Kaplan–Meier analysis. Forced expiratory volume in 1 s (FEV1), percent predicted FEV1, and the 6-item Asthma Control Questionnaire (ACQ-6) were assessed at baseline and Week 24 (pooled SINUS-24/52) in patients with/without history of asthma exacerbation or prior SCS use.
Results
Of 337 patients with coexisting asthma, 88 (26%) required on-treatment SCS use. The requirement for on-treatment SCS use for any reason was significantly lower with dupilumab (20/167 patients; 12%) vs placebo (68/170; 40%); hazard ratio (95% confidence interval) 0.248 (0.150–0.409); p < 0.0001. The most frequent reasons for SCS use were nasal polyps (dupilumab 3% and placebo 27%) and asthma (2% and 9%, respectively). FEV1, percent predicted FEV1, and ACQ-6 were all significantly improved at Week 24 with dupilumab vs placebo irrespective of history of asthma exacerbation or prior SCS use (all p < 0.01).
Conclusion
Dupilumab significantly reduced the requirement for SCS and improved asthma outcomes irrespective of history of asthma exacerbation or prior SCS use vs placebo in patients with CRSwNP and coexisting asthma, demonstrating concomitant reduction of SCS use and asthma disease burden in these patients.
Plain Language Summary
Chronic rhinosinusitis with nasal polyps (CRSwNP) and asthma are type 2 inflammatory conditions that often coexist. Patients with both CRSwNP and asthma generally have worse symptoms that are more difficult to treat. Their standard treatment is topical (inhaled/intranasal) corticosteroids, but where this is ineffective, systemic corticosteroids, also called SCS, are used. SCS are effective at reducing nasal polyp size and improving symptoms, but this effect often does not last, and many patients experience side effects when SCS are used for a long time. Dupilumab, a drug that targets type 2 inflammation, is approved for treating both uncontrolled CRSwNP and moderate-to-severe asthma. Here, we investigate whether dupilumab changes how often patients with CRSwNP and asthma need to use SCS and its effect on their asthma. We found that dupilumab-treated patients were 75% less likely to need SCS than patients treated with placebo and also had significantly greater improvements in measures of their asthma severity, irrespective of their history of previous asthma attacks or previous SCS use. These results show that, in patients with CRSwNP and asthma, dupilumab can improve asthma symptoms and reduce the need for SCS use. Using fewer SCS may help patients avoid the side effects associated with SCS use.
Graphical Abstract
Introduction
Chronic rhinosinusitis with nasal polyps (CRSwNP) is a predominantly type 2 inflammatory disease that shares inflammatory pathophysiology with asthma, with up to 60% of patients with CRSwNP having coexisting asthma.Citation1 These patients typically have more severe CRSwNP and asthma that are more difficult to treat, resulting in poorer upper and lower airway outcomes.Citation2 Patients with poor symptom control despite use of inhaled nasal corticosteroids are often prescribed systemic corticosteroids (SCS) to address systemic inflammation. Although effective at reducing the size of nasal polyps (NP) and improving symptoms, response is often temporary and long-term use of SCS is associated with adverse local or systemic effects.Citation3 Real-world evidence also suggests that the use of SCS as a rescue therapy may be necessary during treatment with biologics in some patients with CRSwNP.Citation4 Dupilumab is a fully human monoclonal antibody that inhibits interleukin (IL)-4 receptor alpha, the shared receptor for IL-4 and IL-13, which are key cytokines driving type 2-mediated inflammation.Citation5,Citation6 In the Phase 3 SINUS-24 and SINUS-52 studies in patients with severe CRSwNP (NCT02912468 and NCT02898454), dupilumab significantly reduced the requirement for SCS during the treatment period by 73.9% and the mean number of SCS courses by 75.3% vs placebo, and was generally well tolerated.Citation7 Here, we report the findings of a post hoc analysis of SCS use and asthma outcomes in SINUS-24 and SINUS-52 patients with coexisting asthma.
Materials and Methods
The SINUS-24 and SINUS-52 studies have been previously described.Citation8 Briefly, eligible patients were ≥18 years of age with bilateral NP and symptoms of CRSwNP despite intranasal corticosteroid therapy and had received SCS in the previous 2 years or previous sinonasal surgery. Patients were required to have a bilateral endoscopic nasal polyp score of ≥5 (≥2 for each nostril) and at least two of moderate-to-severe nasal congestion or obstruction (patient-assessed) and either loss of smell or nasal discharge (anterior or posterior). Patients with coexisting asthma had to be stable in the 6 weeks prior to study entry using their regular asthma treatment. Patients with pre-bronchodilator forced expiratory volume in 1 s (FEV1) ≤50% of predicted normal or those who had participated in prior dupilumab clinical trials were excluded. In SINUS-24, patients were recruited at 67 hospitals or clinical centers in 13 countries. In SINUS-52, patients were recruited at 117 hospitals or clinical centers in 14 countries. Data were collected by investigators at each study site.
In this post hoc analysis, the requirements for SCS use—including the number of courses, dose(s), course duration(s), and time to first use—during the treatment period to Week 52 were assessed. Asthma disease burden was assessed using least squares mean change from baseline to Week 24 for dupilumab vs placebo in the 6-item Asthma Control Questionnaire (ACQ-6, range 0–6), pre-bronchodilator forced expiratory volume in 1 s (FEV1), and percent predicted FEV1. Analyses were conducted on the intention-to-treat population of patients with coexisting asthma, and on subgroups of these patients with and without a history of asthma exacerbation and with and without SCS use within the last 2 years prior to enrollment. Data from SINUS-24 and SINUS-52 were pooled to Week 24 and evaluated to Week 52 in SINUS-52 only.
Results
Overall, at baseline 127/170 (74.7%) and 116/167 (69.5%) patients had a history of asthma exacerbation in the placebo and dupilumab groups, respectively ( and Supplementary Figure 1), and 130/170 (76.5%) and 122/167 (73.1%) had prior SCS use within the last 2 years (). Most of the treatment subgroups showed patients had inadequately controlled asthma at baseline ().
Table 1 Baseline Demographics and SCS Use During the Treatment Period
During the treatment period, a total of 88 patients received SCS, with prednisone the most commonly used SCS (n = 42), and NP and asthma the most frequent reasons for SCS use (). Dupilumab-treated patients had less exposure to SCS than those in the placebo group, demonstrated by reduced on-treatment SCS courses, total course duration, and median cumulative prednisone-equivalent dose (). The requirement for on-treatment SCS was significantly lower with dupilumab compared with placebo in the overall patient population () and in subgroups of patients with or without a baseline history of asthma exacerbation () or prior SCS use ().
Figure 1 Kaplan–Meier plot of time to first use of SCS during the treatment period in patients with CRSwNP and coexisting asthma (A) overall and (B) by history of asthma exacerbationa or (C) prior SCS use.

Significant improvements from baseline were observed with dupilumab vs placebo at Week 24 in ACQ-6, FEV1, and percent predicted FEV1, irrespective of prior history of asthma exacerbation or prior SCS use (Supplementary Figure 2; dupilumab vs placebo p ≤ 0.0016 for all outcomes). No significant differences were observed between patients with or without a history of asthma exacerbation or between patients with or without prior SCS use for any of the three outcomes assessed (all interactions p > 0.45).
Discussion
In this post hoc analysis of patients with severe CRSwNP and coexisting asthma from the SINUS-24 and SINUS-52 studies, dupilumab reduced the requirement for SCS, used mostly for NP and/or asthma exacerbation. Furthermore, the duration of SCS use, recurrent SCS use, and median prescribed SCS dose were all significantly reduced with dupilumab compared with placebo. This reduction in SCS exposure may prevent local and systemic adverse effects in patients, as seen with steroid-sparing strategies in severe asthma.Citation9 Asthma control, as measured by ACQ-6, was improved with dupilumab irrespective of asthma exacerbation history and prior SCS use, demonstrating concomitant reduction of asthma disease burden and SCS use.
The common coexistence of asthma and CRSwNP has given rise to the concept of united airway disease, which is thought to be caused by type 2 inflammatory pathophysiology manifesting as a disease in both the upper and lower airways.Citation10,Citation11 Patients with coexisting asthma typically have more severe CRSwNP that is recalcitrant to standard treatments.Citation12 However, the results presented here suggest that dupilumab represents a viable therapeutic alternative for these difficult-to-treat patients with NP. Another recent analysis of the SINUS population demonstrated dupilumab efficacy in patients with CRSwNP and coexisting asthma irrespective of the severity of their asthma at baseline,Citation13 while the TRAVERSE study demonstrated dupilumab efficacy in patients with Global Initiative for Asthma (GINA)-defined type 2 asthma and CRSwNP.Citation14 The efficacy of dupilumab in CRSwNP and asthma may be explained by its mechanism of action in targeting IL-4 and IL-13, which are key drivers of type 2 inflammation in both diseases,Citation5,Citation6 with more than 95% of the overall SINUS population having type 2 inflammatory disease on the basis of a range of biomarkers and clinical measures.Citation15
Limitations of this analysis include its post hoc nature and the categorization of patients with asthma on the basis of self-reporting by the study participants. To address these, prospective randomized studies involving patients with severe CRSwNP and a confirmed diagnosis of asthma based on clinical guidelines would be informative and provide additional evidence in a more stringently diagnosed patient population. A further limitation relates to the time period of the original SINUS studies (conducted between 2016 and 2017), as guidelines on the use of SCS to control severe asthma have evolved since then, which may limit the generalizability of the results to patients with CRSwNP and coexisting asthma currently.
Conclusion
This post hoc analysis demonstrates that dupilumab treatment provides asthma control while reducing SCS usage and treatment burden in patients with the type 2 disease of CRSwNP and coexisting asthma. This also confirms that this treatment improves patient quality of life while decreasing reliance on SCS use, which can be associated with local and systemic adverse effects.
Abbreviations
ACQ-6, 6-item Asthma Control Questionnaire; CI, confidence interval; CRSwNP, chronic rhinosinusitis with nasal polyps; FEV1, forced expiratory volume in 1 s; HR, hazard ratio; IL, interleukin; NP, nasal polyps; q2w, every 2 weeks; SCS, systemic corticosteroids.
Data Sharing Statement
Qualified researchers may request access to patient-level data and related study documents including clinical study report, study protocol with any amendments, blank case report form, statistical analysis plan, and dataset specifications. Patient-level data will be anonymized, and study documents will be redacted to protect the privacy of trial participants. Further details on Sanofi’s data sharing criteria, eligible studies, and process for requesting access can be found at: https://www.vivli.org/.
Ethics Approval and Informed Consent
The SINUS-24 and SINUS-52 studies were conducted according to the Declaration of Helsinki principles and were approved by the local institutional review board or ethics committee at each study site (Supplementary Table S1). All patients provided written informed consent.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Mark Gurnell reports steering committee membership and speakers’ bureau fees for AstraZeneca, and speakers’ bureau fees for Novartis. Amr Radwan, Scott Nash, and Yamo Deniz are employees of Regeneron Pharmaceuticals Inc. and may hold stock and/or stock options in the company. Claus Bachert reports grants from Sanofi and was the principal investigator for studies for Sanofi, GlaxoSmithKline, and Novartis, during the conduct of the study. Njira Lugogo is an advisory board member and has received consultancy fees from Novartis, has received research grants from Avillion and Gossamer Bio, and is an advisory board member and has received consultancy fees and research grants from AstraZeneca, Genentech, GlaxoSmithKline, Regeneron Pharmaceuticals Inc., Sanofi, and Teva Pharmaceutical Industries Ltd. Seong H Cho has received grants from and is an advisory board member for Sanofi, and Regeneron, during the conduct of the study; received grants from the National Institute of Health, and received research grants from and is an advisory board member for Insmed, outside the submitted work. Haixin Zhang is a former employee of Regeneron Pharmaceuticals Inc. and may hold stock and/or stock options in the company. Asif H Khan, Juby A Jacob-Nara, and Paul J Rowe are employees of Sanofi and may hold stock and/or stock options in the company.
Acknowledgments
The authors thank Shahid Siddiqui, MD (formerly of Regeneron Pharmaceuticals Inc.), and Andrew Menzies-Gow, MD (Royal Brompton and Harefield Hospitals), for insights and guidance. Medical writing/editorial assistance provided by Joseph Hodgson, PhD, of Adelphi Group, Macclesfield, UK, funded by Sanofi and Regeneron Pharmaceuticals Inc. according to the Good Publication Practice guideline.
Additional information
Funding
References
- Ragab A, Clement P, Vincken W. Objective assessment of lower airway involvement in chronic rhinosinusitis. Am J Rhinol. 2004;18(1):15–21. doi:10.1177/194589240401800105
- Khan A, Huynh TMT, Vandeplas G, et al. The GALEN rhinosinusitis cohort: chronic rhinosinusitis with nasal polyps affects health-related quality of life. Rhinology. 2019;57(5):343–351. doi:10.4193/Rhin19.158
- Fokkens WJ, Lund V, Bachert C, et al. EUFOREA consensus on biologics for CRSwNP with or without asthma. Allergy. 2019;74(12):2312–2319. doi:10.1111/all.13875
- Meier EC, Schmid-Grendelmeier P, Steiner UC, Soyka MB. Real-life experience of monoclonal antibody treatments in chronic rhinosinusitis with nasal polyposis. Int Arch Allergy Immunol. 2021;182(8):736–743. doi:10.1159/000514262
- Gandhi NA, Pirozzi G, Graham NMH. Commonality of the IL-4/IL-13 pathway in atopic diseases. Expert Rev Clin Immunol. 2017;13(5):425–437. doi:10.1080/1744666x.2017.1298443
- Le Floc’h A, Allinne J, Nagashima K, et al. Dual blockade of IL-4 and IL-13 with dupilumab, an IL-4Rα antibody, is required to broadly inhibit type 2 inflammation. Allergy. 2020;75(5):1188–1204. doi:10.1111/all.14151
- Desrosiers M, Mannent LP, Amin N, et al. Dupilumab reduces systemic corticosteroid use and sinonasal surgery rate in CRSwNP. Rhinology. 2021;59(3):301–311. doi:10.4193/Rhin20.415
- Bachert C, Han JK, Desrosiers M, et al. Efficacy and safety of dupilumab in patients with severe chronic rhinosinusitis with nasal polyps (LIBERTY NP SINUS-24 and LIBERTY NP SINUS-52): results from two multicentre, randomised, double-blind, placebo-controlled, parallel-group phase 3 trials. Lancet. 2019;394(10209):1638–1650. doi:10.1016/s0140-6736(19)31881-1
- Volmer T, Effenberger T, Trautner C, Buhl R. Consequences of long-term oral corticosteroid therapy and its side-effects in severe asthma in adults: a focused review of the impact data in the literature. Eur Respir J. 2018;52(4):1800703. doi:10.1183/13993003.00703-2018
- Klain A, Indolfi C, Dinardo G, et al. United airway disease. Acta Biomed. 2021;92(S7):e2021526. doi:10.23750/abm.v92iS7.12399
- Mullol J, Maldonado M, Castillo JA, et al. Management of united airway disease focused on patients with asthma and chronic rhinosinusitis with nasal polyps: a systematic review. J Allergy Clin Immunol Pract. 2022;10(9):2438–2447.e2439. doi:10.1016/j.jaip.2022.04.039
- Laidlaw TM, Mullol J, Woessner KM, Amin N, Mannent LP. Chronic rhinosinusitis with nasal polyps and asthma. J Allergy Clin Immunol Pract. 2021;9(3):1133–1141. doi:10.1016/j.jaip.2020.09.063
- Busse WW, Pavord ID, Siddiqui S, et al. Dupilumab improves outcomes in patients with chronic rhinosinusitis with nasal polyps and coexisting asthma irrespective of baseline asthma characteristics. J Asthma Allergy. 2023;16:411–419. doi:10.2147/jaa.S391896
- Rabe KF, Pavord ID, Busse WW, et al. Dupilumab improves long-term outcomes in patients with uncontrolled, moderate-to-severe GINA-based type 2 asthma, irrespective of allergic status. Allergy. 2023;78(8):2148–2156. doi:10.1111/all.15747
- Bachert C, Khan A, Lee S, et al. Prevalence of type 2 inflammatory signatures and efficacy of dupilumab in patients with chronic rhinosinusitis with nasal polyps from two phase 3 clinical trials: SINUS-24 and SINUS-52. Int Forum Allergy Rhinol. 2023 1–10. doi:10.1002/alr.23249