
ABSTRACT
Introduction
Return to play related research is increasing rapidly, with two recent competency-based frameworks offering conceptualised support for on-field rehabilitation (OFR) decision-making. It is still unknown, however, who is responsible for OFR and how they typically select, monitor, and progress OFR processes.
Aims
The purpose of this study was to investigate current OFR practice within English professional football to support practitioners with decision-making and highlight opportunities for future research related to the design, monitoring, and progression of OFR.
Methods
Sixty-nine practitioners responsible for the design and implementation of OFR at 69 clubs (75% of the English Premier League and Football League) responded to a survey containing 30 questions (14 open and 16 closed).
Results
The main findings were that therapists (physiotherapists/sports therapists) have the largest influence on OFR, followed by physical performance coaches (sports scientists/strength and conditioning coaches), technical coaches and medical doctors. There was more agreement for the ordering of specific OFR drills earlier in the process when activities are easier to control. The most frequently reported objective monitoring tool was global positioning systems (GPS), with functional/clinical experience/expertise remaining subjectively vital. GPS outputs (e.g., sprint metrics and accelerations/decelerations) were most used for between session decision-making, with verbal communication being key for within session decision-making.
Conclusion
Future research should use evidence of current practice, such as drill design and monitoring techniques, to explore drill-level analysis and give practitioners greater insights into which stage of current OFR frameworks specific drills fall, and how they might be more objectively progressed/regressed.
Introduction
When injuries occur in elite football, it is vital that players are returned timely and with an acceptable risk of subsequent injury to mitigate negative performance and economic implications (López-Valenciano et al. Citation2020). Whilst the incidence and impact of injuries are well reported, criterion evidence for return to play (RTP) protocols from moderate to severe (>14 days) injuries is lacking (Hägglund et al. Citation2018; Ekstrand et al. Citation2020, Citation2021; Eliakim et al. Citation2020). There is growing agreement that RTP processes should be competency-based (Ardern et al. Citation2016; Bisciotti et al. Citation2019; Buckthorpe et al. Citation2019a; Taberner et al. Citation2019), and transition through clinical rehabilitation, on-field rehabilitation (OFR), return to training, return to competition, and return to performance (Buckthorpe et al. Citation2019). OFR acts as the bridge between medical and coaching staff, whereby graduated movements/activities common to the game (e.g., jogging, sprinting, turning, cutting, kicking) are performed to ready the player in an ecologically valid environment (Taberner et al. Citation2022).
Recently, two conceptual frameworks have been developed which offer stepwise progressions to OFR processes (Buckthorpe et al. Citation2019a; Taberner et al. Citation2019). Designed as an educational piece to provide evidential support to current practice, the four pillars of OFR suggest that movement quality should be restored before adding physical conditioning and then sport-specific skills, whilst progressively developing chronic training load (Buckthorpe et al. Citation2019a). Additionally, these authors promote a 5-stage progression (from anterior cruciate ligament injury) of (1) linear and (2) multidirectional movements, (3) technical and reactive movement actions, (4) sport-specific movements and skill reintegration, and (5) training simulation and reconditioning (Buckthorpe et al. Citation2019b). These progressions are like those proposed by Taberner et al. (Citation2019) in the ‘control-chaos continuum’, although Taberner et al. (Citation2019) add more specific external running load guidelines, highlighting the need to contextualise practice, and offer considerations for different pathologies (Taberner et al. Citation2019, Citation2020, Citation2020; Taberner, Haddad, et al. Citation2020).
Whilst both frameworks appear conceptually sound, they are based on expert opinion and case study applications. Despite inherent challenges, there is now a need to attempt validation through experimental evidence (Hägglund et al. Citation2018; Ekstrand et al. Citation2020; Impellizzeri et al. Citation2020). To enhance understanding, insights into how OFR is currently being executed and how this relates to existing frameworks should be sought. Whilst current frameworks highlight the importance of training load management, there is scarce information regarding specific metrics and thresholds for OFR (Dunlop et al. Citation2020). At present, there is a lack of knowledge about how practitioners select, monitor and progress OFR. There is therefore a need to capture this information to improve practice, generate specific research questions and assist in future study design (Dunlop et al. Citation2020; Fanchini et al. Citation2020; Impellizzeri et al. Citation2020). The purpose of this study was to investigate current OFR practices within English professional football. Its aims were to: (i) describe details of those responsible for OFR; (ii) identify frequently selected OFR drills and their progressions; and (iii) investigate current techniques to monitor training load during OFR and, if used, explore popular Global Positioning System (GPS) metrics.
Methods
Participants
One member of the Sports Science and Medicine department from each English Football League club (Premier League to League Two; 92 clubs) was contacted and invited to participate in this structured survey. We requested the survey to be completed by the person with lead responsibility for the design and implementation of OFR processes. This approach was taken to be reflective of club processes, rather than individual philosophy, and to avoid response bias. Participants were asked to answer all questions from a general/club rather than personal perspective and avoid specific examples (Buchheit et al. Citation2023). If known by the authors, the appropriate person was contacted directly, else industry networks and social media platforms were used to reach a person in that club for redirection. An email was then sent to potential respondents outlining the purpose and requirements of the study, with a web link to the survey (QualtricsTX online software, Utah, USA; https://www.qualtrics.com). Consent was recorded via the participant selecting informed agreement of involvement in question one, which enabled access to the rest of the survey. Data were collected between April and June 2021 to reflect practice in the 2020/2021 season. The Ethics Committee of the University of Suffolk (Ipswich, United Kingdom) approved this study (RETH20/048).
Survey
The survey consisted of 30 questions (Appendix A) and included seven sections under three broader categories. The first part (Section 1 – consent and personal information, and Section 2 – field-based rehabilitation frameworks) sought to understand the person completing the survey and the influence of different job roles on OFR delivery. The second part was structured on the four pillars of OFR (Buckthorpe et al. Citation2019a) to provide an evidential framework. This framework was selected due to its ease of use with regard to clearly defining the stages of OFR. Participants were surveyed to obtain their typical selection and progression of OFR drills during on-field movements (Section 3), on-field physical conditioning (Section 4), and sport-specific activities (Section 5). The third part explored how practitioners monitor and progress training loads during OFR (Section 6), and gave respondents the opportunity to add any additional information including their thoughts on future research direction (Section 7).
The survey items included six multiple-choice questions (i.e., choose from the following list), five rating questions, three scale questions, and two simple multiple-choice questions (i.e., yes/no). Operating as a Likert scale, each rating scale contained five points with labelled anchors, as fully labelled scales are more reliable and valid than partially labelled scales (Krosnick and Presser Citation2010). The survey also included 14 open questions. The inclusion of open questions was to encourage rich textual information to compliment the quantitative responses (Wright et al. Citation2012). The questions were designed by MA and for content validity supported by three experts in the field of OFR (one sports physician, one physiotherapist, one sports scientist) and three academics (one biomechanist, one physiologist, and one strength and conditioning coach with applied experience). Following two iterations, three questions were modified (two to add count data, one for clarity of wording), five were added (two to give greater insights into qualifications of respondents, two concerning fitness testing, and one to gauge differences between arbitrary and absolute GPS metrics), and two removed as they had become redundant with improved structure of the survey. The survey was then piloted by three experienced (>10 years) strength and conditioning coaches who were working in elite football and actively involved in delivering OFR, but who did not meet the study inclusion criteria (i.e., not currently working at an English professional football team). Following pilot testing, an additional question was modified (to improve clarity of wording) with changes made to software settings to enhance usability.
Data analysis
Raw data were exported to Microsoft Excel (Microsoft Corp, Redmond, WA, USA) for analysis. A mixed-method approach was taken to accommodate the different types of questions asked. Frequency, rate, and rank analysis were performed on closed questions. To yield greater insights, Q22, Q23 and Q25 (Appendix A) were ranked whereby responses of ‘extremely influential’ were awarded five points, ‘very influential’ four points, ‘moderately influential’ three points, ‘slightly influential’ two points, and ‘not influential’ one point as in previous studies (McCall et al. Citation2014, Citation2016). The total of these points was summed and ranked in order of highest to lowest overall. Additionally, responses were labelled as positive (‘extremely/very influential’), neutral (‘moderately influential’), or negative (‘slightly/not influential’) and presented as a percentage for each category.
Open questions were analysed manually using inductive qualitative content analysis (Elo and Kyngäs Citation2008). For instance, following data immersion, the open responses were subject to first cycle coding and refined into similar meaning units (i.e., words, sentences) and order concepts. To ensure trustworthiness, the codes, meaning units and categories/themes were reflected on by members of the research team until consensus and consolidation of the findings were verified. This process was continued until data saturation had occurred with emerging themes (Field et al. Citation2021).
Data availability statement Due to the sensitivity of data collected, all have been anonymised and presented collectively. Where direct quotations have been used, potentially identifiable information has been omitted. Additional information has been provided through supplementary material. Data sharing outside that presented is not available to protect those who responded.
Results
Participants
In total, 69 surveys were returned (75% response rate), 14 (15%) did not complete after the survey was sent, and nine (10%) did not respond. Respondents worked in the Premier League (n = 15, 75% of clubs in this league), Championship (n = 18, 75%), League One (n = 18, 75%) and League Two (n = 18, 75%).
From these respondents, 46 (67%) were performance coaches and 23 (33%) were medical staff. Of these, 29 identified as being a sport scientist (42%), 19 physiotherapists (28%), 16 strength and conditioning coaches (23%), and 5 as sports therapists (7%). There were no medical doctors amongst the respondents. Most listed their highest academic qualification as a postgraduate degree (n = 47, 68%), followed by an undergraduate (n = 14, 20%) and doctorate (n = 8, 12%). Supplementary material contains additional details relating to the employment, experience, and qualifications of respondents.
OFR frameworks/processes
More than half of the respondents (n = 38, 55%) stated both applied experiences and peer-reviewed frameworks had the biggest influence on their current OFR practice. Twenty-nine (42%) favoured applied experiences, with only two (3%) relying mostly on peer-reviewed frameworks. Content analysis found applied experience either came from shared (n = 18, 10%) or individual (n = 13, 7%) experiences.
Content analysis also indicated that doctors are required to provide medical clearance and ongoing support, but that they have little influence on OFR delivery. Indeed, only 14% of responses given for doctors could be described as positive (very/extremely influential) compared to 78% for physical performance coaches (sports science/strength and conditioning coaches) and 93% for therapists (physiotherapists/sports therapists) ().
Figure 1. The influence of different job roles on OFR. Horizontal coloured bars represent %, numbers within bars represent count frequency.
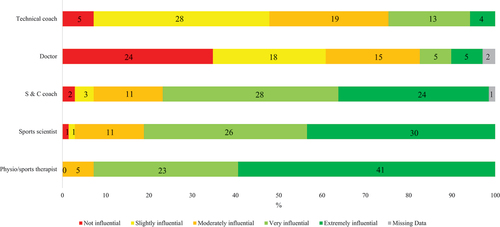
The importance of the multidisciplinary team throughout the process was a predominant theme, coded most frequently (n = 31, 48%). Results indicate that the overall OFR process is predominately led by physiotherapists (n = 23, 36%); however, there appears to be a handover point with therapists (physiotherapists/sports therapists) taking early-stage responsibility (n = 25, 39%) before transitioning towards performance staff (sports scientists/strength and conditioning coaches) during the late-stage (n = 28, 44%). Coach involvement, especially towards late-stage, appears important with doctors mainly involved in initial diagnosis/treatment and providing medical support/clearance.
On-field movement, physical conditioning, and sport-specific progressions
demonstrates commonality of OFR progressions. Jog/walk progressions and running mechanic drills appeared to be used similarly, with the others forming a sequential order (). During on-field movement progressions, most responders start with body weight exercises (82%) and finish with controlled change of direction activities (62%). The introduction of ball work appears more variable, with content analysis indicating that this is often prescribed on an individual basis and largely for psychosocial reasons. During on-field physical conditioning, most start with pitch-based runs (58%) and finish with random change of direction drills (77%) (). The introduction of isolated acceleration and deceleration drills appears to be interchangeable. Although sport-specific progressions followed a general trend, ordering is perhaps less clear than during more controlled discrete tasks. This said, most (67%) introduced small sided games last ().
Table 1. Rank order (%) of activities (used earlier [1] to later [7]) with regard to typical field-based movements (A), physical conditioning (B) and sport-specific skill progressions (C).
Content analysis revealed the most frequently used activities within each subsection. In sum, the most frequently coded drills were box to box runs (n = 53), interval runs (n = 18), S-runs (n = 18), T-drill (n = 16), pitch laps (n = 14), slalom runs (n = 14), and Z-runs (n = 14) (Supplementary Material, Table B).
Monitoring OFR
Of the respondents, 59 (86%) highlighted that they use fitness testing at their club to benchmark results as part of RTP. Content analysis found that most did some form of aerobic capacity (n = 34), strength (n = 29), jump (n = 28) and/or speed (n = 21) testing.
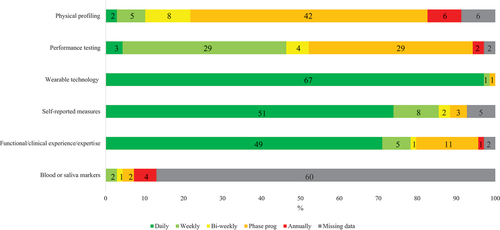
Using a Likert scale (1 = not influential, 5 = extremely influential), most respondents ranked wearable technology (summed score = 341, n = 69) as the most popular training load monitoring technique, followed by self-reported measures (299, n = 64), functional/clinical experience/expertise (291, n = 67), performance testing (203, n = 67), physical profiling (144, n = 63), and blood or saliva markers (19, n = 9), respectively (Supplementary Material, Table D). Additional content analysis highlighted that blood or saliva markers were used for health-related investigations and not necessarily OFR. Responses indicated that wearable technology is used daily in 97% of cases, self-reported measures 74%, and functional/clinical experience/expertise 71% (). GPS was the most coded term during content analysis (n = 22, 61%).
Figure 2. Tools used to monitor training load, and frequency of use. Horizontal coloured bars represent %, numbers within bars represent count frequency.
For within session decision-making, verbal communication (summed score = 329, n = 69) was ranked highest (100% positive), followed by functional/clinical experience/expertise (313, n = 69, 94% positive), self-reported measures (303, n = 69, 86% positive), wearable technology (300, n = 69, 91% positive), and video (192, n = 64, 23% positive) . For between session decision-making, functional/clinical experience/expertise (306, n = 68, 90% positive) was ranked highest followed by wearable technology (298, n = 69, 93% positive), self-reported measures (280, n = 67, 77% positive), performance testing (268, n = 69, 70% positive), physical profiling (227, n = 66, 48% positive), and blood or saliva markers (44, n = 22, 0% positive) . Content analysis revealed that monitoring techniques transitioned from more subjective to objective as OFR progressed from early- to late-stage, with GPS being a dominant theme.
Figure 3. The importance of different monitoring tools to inform decision-making within sessions (A), and between sessions (B), with the importance of selected GPS metrics during OFR (C). Horizontal coloured bars represent %, numbers within bars represent count frequency. Accels = accelerations, decels = decelerations, HR = heart rate, HSR = high speed running, MPM = meters per minute, sprint = sprint distance.
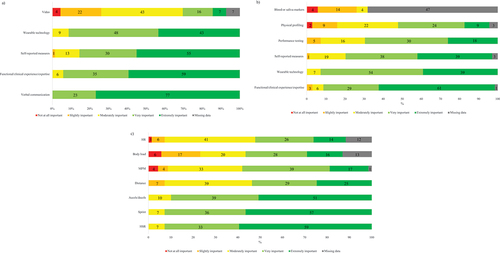
Concerning GPS metrics, high-speed running (HSR) (summed score = 312, n = 69, 93% positive) and sprint distance (310, n = 69, 93% positive) were rated as most important, followed by accelerations and decelerations (304, n = 69, 90% positive), total distance (256, n = 69, 54% positive), meters per minute (246, n = 68, 57% positive), heart rate (215, n = 61, 41% positive), and ‘Body Load’ (a GPS company derived metric that summarises accumulated accelerations (Beato and Drust Citation2021); 201, n = 60, 43% positive) . Content analysis highlighted that generally OFR was progressed on a continuum from volume to intensity (n = 12, 27%). Respondents also indicated that the reasons for using GPS included individualisation (n = 24, 28%), player comparisons (n = 19, 22%), maximal speed progressions (n = 13, 15%), comparison against match outputs (n = 10, 12%), and to ensure position-specific targets are met (n = 7, 8%). Only two respondents (2%) used GPS to compare against normative data within the literature.
Thirteen (19%) respondents stated that they predominately use arbitrary GPS metrics (i.e., set at a squad level), 17 (25%) used relative (i.e., set at an individual level), and 39 (56%) used a combination of both. Although the majority (n = 23, 58%) said that GPS metrics and thresholds do not alter across their RTP process, content analysis revealed that in such instances there is a tendency to go from absolute to relative. Seven (14%) respondents indicated that future research should create potential GPS targets, with 14 (28%) promoting the need for more objective frameworks. The majority (n = 28, 54%) categorised HSR as ≥5.5 m·s−1 (19.8 km·h−1), with 12 (23%) using a percentage (relative) threshold. For sprint distance, most respondents (n = 21, 41%) used ≥7.0 m·s−1 (25.2 km·h−1), some a percentage (n = 10, 20%), and others a combination of both (n = 6, 12%). Categorisations for accelerations and decelerations were less clear, with seven (17%) using a threshold ≥ 2.0 m·s−1 (7.2 km·h−1) and eight (20%) ≥ 3.0 m·s−1 (10.8 km·h−1). Thresholds based on match outputs were also coded on seven occasions (13%) for HSR, seven (14%) for sprint distance, and nine (22%) for accelerations and decelerations (Supplementary Material, Table E).
Content analysis revealed that future research should further explore GPS usage for OFR and, if possible, create targets/thresholds for returning players. To support this, typical GPS outputs for specific drills would support planning, as would information on the loading journey from OFR to return to performance.
Discussion
Who is responsible for OFR and what evidence do they use?
This survey reinforces the importance of shared decision-making in the RTP process (Dijkstra et al. Citation2017; Dunlop et al. Citation2020). Therapists (physiotherapists/sports therapists) were the most influential decision makers throughout OFR, followed by performance staff (sports science/strength and conditioning coaches) and technical coaches. Doctors were rated least influential, with content analysis revealing that whilst input is required for medical clearance to return to OFR and offer ongoing support, direct involvement in OFR decision-making is limited. It should be acknowledged that no doctors completed this survey and thus might be underrepresented. The findings of this study might also be influenced by practice specific to the country of origin, with cultural differences in other geographical locations likely to alter responses (Buchheit et al. Citation2023). The fact that technical coaches were deemed more influential than doctors during OFR could be explained by a need to work collaboratively to return the player to the club’s playing and subsequent conditioning philosophy. Technical coaches should be active drill designers (Armitage et al. Citation2022) and facilitate transitions from OFR to return to training, return to competition and return to performance, as effective communication between coaching and medical staff is an important factor to mitigate against subsequent injury (Ekstrand et al. Citation2019; Ghrairi et al. Citation2019). Although outside the scope of this paper, this creates an interesting future research question with regard to who has overall responsibility for OFR. Currently, specific roles and responsibilities are poorly defined (Arvinen-Barrow and Clement Citation2015). Whilst it is perhaps intuitive that medical staff should take accountability during the rehabilitation stage and performance staff during reconditioning, the suitability of staff skillsets to lead on OFR remains unclear.
Content analysis found that OFR progressions should be continuum-based (n = 20, 54%), with the control-chaos continuum (Taberner et al. Citation2019) often mentioned directly (n = 18, 49%). One respondent stated, ‘the framework that has most influenced my practice would be Matt Taberner’s “Control-Chaos Continuum”. This provided a framework on how to progress athletes through the on-field rehab safely whilst ensuring players return to training having been exposed to a number of stimuli’. Balancing acute and chronic training loads (i.e., Gabbett Citation2016) was also popular (n = 9, 24%), although this method has been strongly challenged due to conceptual and computational limitations (Impellizzeri, Tenan, et al. Citation2020; Impellizzeri, Woodcock, et al Citation2020). The four pillars of OFR were only mentioned once, with this respondent stating ‘similar to Taberner’s work, gives practitioners an idea of on-field rehabilitation programming that can assist in the logical progression to return to train/play’. These findings indicate that research is reaching practice, however it does not indicate if it is being applied properly. Research using observational or participatory designs might fit better in the future. The fact that nearly half (42%) of respondents still favour applied experiences independently suggests that more can still be done (Bartlett and Drust Citation2021).
Drill selection and progression
A large proportion of practitioners relying on their practical experiences reinforces a need to capture such perceptions and for them to be shared and developed. In the absence of empirical evidence (Hägglund et al. Citation2018; Ekstrand et al. Citation2020; Impellizzeri et al. Citation2020), insights into clinical experience/expertise are vital to evolve evidence-based practice (Coutts Citation2017; Fanchini et al. Citation2020). Such information is also important for creating future research questions (Dunlop et al. Citation2020), and where possible stimulating experimental studies with testable hypotheses (Impellizzeri et al. Citation2020).
An example of this could be drill-level analysis to offer greater insights into within and between session progressions for current OFR frameworks (i.e., in what stage do specific drills broadly fall) (Armitage et al. Citation2022). Indeed, responses regarding how future research might better support OFR included ‘some exercise structures based on GPS metrics’, ‘standardised drills with average GPS outputs that can be accurately used to plan and programme OFR’, and ‘how specific drills can repeatedly provide set metrics which could be used to plan sessions with a high degree of accuracy’.
This study found that typical field-based movement progressions appeared logical and consistent, supporting a notion of continuum-based progressions for relatively ‘controlled’ OFR tasks. Jog/walk and running mechanics progressions were somewhat interchangeable, although overall jog/walks were implemented before running mechanic drills more frequently. During the movement progression stage, there was strong consensus for starting with body weight exercises and finishing with controlled change of direction tasks. Physical conditioning progressions were more variable, with linear intermittent runs being implemented before increased intensity linear runs more frequently. It should be acknowledged, however, that responders may have benefited from additional definitions of terms to help differentiation. Generally, physical conditioning started with pitch-based runs and finished with random change of direction tasks. Although sport-specific skill progressions followed a general trend, this was the most variable (i.e., less choices that were > 50%). This highlights the complexity of the area, with it being easier to be more prescriptive early on during OFR when things are more controlled. According to the responders of this survey, technical ball work (e.g., volleys, passing and heading) should be completed before moving onto ball striking, tackling and position-specific tasks (although this might be influenced by pathology). There was agreement that small sided games (or simulated 1v1’s) should be targeted last, and before a graduated return to team training.
These findings offer additional detail to existing conceptual frameworks (Buckthorpe et al. Citation2019a; Taberner et al. Citation2019) with regard to the ordering of specific drills. Due to the structure of this survey, alignment of findings to the four pillars is easier, however some parallels to the control-chaos continuum can still be made. On-field movement progressions could be described as highly controlled and physical conditioning progressions (except random change of direction tasks) could be described as moderately controlled. Depending on the task/intensity ball striking, tackling, and position-specific tasks could be placed under control-chaos/moderate chaos, with simulated match-play (i.e., small sided games) high chaos. Where the control-chaos continuum offers greater breadth is an appreciation that drills can be constrained to increase/decrease the complexity and/or the physical demands of the task. Therefore, some drills listed within this study could be replicated across the OFR process but manipulated with regard to distances, speeds, work:rest ratios, etc. The potential for high variability within/between drills due to differences between pathologies and individuals should be acknowledged, but decision-making could still be supported by creating ‘bucket’ groups. For example, if a drill demonstrates high variability this could be classified as ‘high chaos’ and should be considered later when planning OFR.
Monitoring OFR
The majority of respondents (n = 59, 86%) highlighted that they use fitness testing at their clubs for ‘benchmarking’ purposes. This is less than the 95% reported by Buchheit et al. (Citation2023) and might be explained by differences in leagues, match schedules and training philosophies. It would be interesting in the future to explore when and how these tests are deployed and whether they are pathology-specific.
Wearable technology (i.e., GPS) appears to be extremely popular for supporting OFR decision-making, with 97% (n = 67) reporting that it is used daily. In agreement with Buchheit et al. (Citation2023), speed outputs (HSR ≥ 5.5 m·s−1/19.8 km·h−1, sprint distance ≥ 7.0 m·s−1/25.2 km·h−1) were reported to be the most important metrics. Akenhead and Nassis (Citation2016) completed a similar survey study, concentrating on healthy (non-injured) players with some similarities in findings. Although they reported total distance more frequently than the current study, acceleration variables and HSR were the most used. A reduction in the importance of measuring total distance could be explained by a change in the energetic demands of the sport over recent years. Allen et al. (Citation2023) have recently reported only a small increase (1%) in total distance covered in matches between 2014/15 and 2018/19, but moderate increases in high-intensity running (12%) and sprints (15%) over the same period. As the game continues to become more intense with a greater number of accelerations, decelerations, and changes of direction (Harper et al. Citation2019; Hostrup and Bangsbo Citation2023), the need to accurately quantify such actions grows. The ability of GPS to measure high-intensity activities over shorter distances has been questioned (Delaney et al. Citation2019), hence an increasing interest in accelerometry-derived metrics (Verheul et al. Citation2020). The pinnacle for practitioners might be a single metric or technology to give an indication of overall load, however this currently seems a long way off and/or theoretically implausible. For now, practitioners should look to combine technologies and their associated metrics to inform decision-making (Akenhead and Nassis Citation2016; Delaney et al. Citation2018; Armitage et al. Citation2022). For example, external running load (e.g., HSR via GPS), external mechanical load (e.g., accelerations/decelerations via accelerometers), external biomechanical load (e.g., impact loading via inertial measurement units), metabolic/cardiovascular load (e.g., heart rate) and response to load (e.g., RPE/wellness questionnaires). A common finding from this study and that of Akenhead and Nassis (Citation2016) is the importance of blending both objective and subjective measures. With regard to OFR, this study found functional/clinical experience/expertise to be a vital source of information for within and between session decision-making. Whilst technological advancements will help to support better decisions, OFR is likely to remain a balance between the application of science and the art of coaching (Allen et al. Citation2021; Buchheit et al. Citation2023). Content analysis revealed a need to create targets/thresholds for each stage within current frameworks and to generate typical outputs from commonly used drills. This will provide support in two ways: offer experienced practitioners a source to justify decision-making and/or challenge conformation biases, or create a starting point for those without sufficient clinical experience (i.e., early-career practitioners). Once greater understanding is provided for OFR, consideration should also be given to ‘quantifying the success of a rehabilitation process and what the long-term implications are on a player’. This might include exploring ‘GPS metrics for certain injuries’ and the safe return of players ‘with reduced risk of reinjury based on achieving specific markers/thresholds e.g., number of training sessions, percentages of training/game loads’. These insights would give practitioners greater awareness of training load management across the whole return to performance process. This said, such information should always be considered within the complex nature of sports injuries, and a need to address movement qualities as well as quantities, especially during high-risk tasks in relation to the aetiology of specific injuries.
Limitations
In agreement with Dunlop et al. (Citation2020), we acknowledge that only level 5 evidence (expert opinion) has been provided, and as such this research should be updated alongside emerging evidence and paradigm shifts. Furthermore, it should be acknowledged that this study contains the potential for responder bias (Gregson et al. Citation2022). The responders’ prior knowledge/understanding might have influenced their responses to specific research questions. Moreover, the authors’ personal networks might have influenced responses and explain a greater representation of performance staff. Whilst the intention of this study was to survey staff only working in elite English football, with them giving general responses to be reflective of club practice rather than personal philosophy, the overall sample size could still be deemed as low, despite the good response rate (75%). Interpretation of results might have also been improved by limiting missing data points, for which this study contained 1323 (Supplementary Material, Table A). Open/follow-up questions generated the most ‘missing’ data points (n = 980), highlighting a potential reluctance of responders to answer numerous open questions (Gray Citation2021). In three questions, nine responses were removed due to a formatting issue that created uncertainty over the validity of responses completed on mobile devices, which generated 189 missing data points. A further 151 missing data points were generated from questions that contained ‘if used’, emphasising a need for surveys to carefully consider the wording of their questions and/or add clearer not applicable options, as the missing data could have been generated by the options not being used by the respondents. To limit impact, missing data were treated as missing not at random and thus only data given from responders were analysed (Benson et al. Citation2021; Bache-Mathiesen et al. Citation2022; Borg et al. Citation2022).
Conclusion
This is the first study of its kind to survey current OFR practice within the English Preimer League and Football League. It reinforces a need for a multidisciplinary approach, with medics leading the early aspects before passing on to performance staff at the latter-stage. Although there was evidence of research influencing practice, OFR drills are still largely selected and progressed based on practitioners’ own experience. There was more agreement on the ordering of specific drills earlier in the process. Both objective and subjective measures were important to monitor training loads during OFR, particularly functional/clinical experience/expertise and GPS monitoring. Speed outputs and accelerations/decelerations were the most used GPS metrics for OFR. Future research should seek to add objectivity to commonly used OFR drills, embracing multiple-monitoring techniques. From here, injury/individual specific targets could be developed, with greater training load information generated across the RTP journey to quantify the success of OFR.
Author contributions
Mark Armitage was responsible for the concept of the paper and its writing. Stuart McErlain-Naylor, Gavin Devereux, Marco Beato and John Iga provided feedback and support throughout. Allistair McRobert and Simon Roberts supported in the analysis and interpretation of results as well as commenting on each draft. Matt Buckthorpe supervised the project. All authors contributed to the article and approved the final version.
Supplemental Material
Download Zip (99.8 KB)Acknowledgements
The authors would like to thank the 69 responders to the survey. We acknowledge the contribution of Dr Daniel Broman and Mo Gimpel in the design of the survey, and Nick Harvey, Ben Rosen, and Gary Hall for piloting the survey.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Supplementary material
Supplemental data for this article can be accessed online at https://doi.org/10.1080/24733938.2024.2313529
Additional information
Funding
References
- Akenhead R, Nassis GP. 2016. Training load and player monitoring in high-level football: current practice and perceptions. Int J Sport Physiol. 11(5):587–593. doi: 10.1123/ijspp.2015-0331.
- Allen T, Taberner M, Zhilkin M, Rhodes D. 2023. Running more than before? The evolution of running load demands in the English Premier League. Int J Sport Sci Coach. 174795412311645. ahead of print. doi: 10.1177/17479541231164507.
- Allen T, Wilson S, Cohen DD, Taberner M. 2021. Drill design using the ’control-chaos continuum’: blending science and art during return to sport following knee injury in elite football. Phys Ther Sport. 50:22–35. doi: 10.1016/j.ptsp.2021.02.011.
- Ardern C, Glasgow P, Schneiders A, Witvrouw E, Clarsen B, Cools A, Gojanovic B, Griffin S, Khan KM, Moksnes H, et al. 2016. Consensus statement on return to sport from the First World Congress in sports physical therapy, Bern. Br J Sport Med. 50(14):853–864. doi: 10.1136/bjsports-2016-096278.
- Armitage M, McErlain-Naylor SA, Devereux G, Beato M, Buckthorpe M. 2022. On-field rehabilitation in football: current knowledge, applications and future directions. Front Sports Act Living. 4. online. doi: 10.3389/fspor.2022.970152.
- Arvinen-Barrow M, Clement D. 2015. A preliminary investigation into Athletic trainers’ views and experiences of a multidisciplinary team approach to sports injury rehabilitation. Athletic Train Sport Health Care. 7(3):97–107. doi: 10.3928/19425864-20150422-05.
- Bache-Mathiesen LK, Andersen TE, Clarsen B, Fagerland MW. 2022. Handling and reporting missing data in training load and injury risk research. Sci Med Footb. 6(4):452–464. doi: 10.1080/24733938.2021.1998587.
- Bartlett JD, Drust B. 2021. A framework for effective knowledge translation and performance delivery of sport scientists in professional sport. Eur J Sport Sci. 21(11):1579–1587. doi: 10.1080/17461391.2020.1842511.
- Beato M, Drust B. 2021. Acceleration intensity is an important contributor to the external and internal training load demands of repeated sprint exercises in soccer players. Res Sports Med. 29(1):67–76. doi: 10.1080/15438627.2020.1743993.
- Benson LC, Stilling C, Owoeye OBA, Emery CA. 2021. Evaluating methods for imputing missing data from longitudinal monitoring of athlete workload. J Sports Sci Med. 20(2):188–196. doi: 10.52082/jssm.2021.188.
- Bisciotti GN, Volpi P, Alberti G, Aprato A, Artina M, Auci A, Bait C, Belli A, Bellistri G, Bettinsoli P, et al. 2019. Italian consensus statement (2020) on return to play after lower limb muscle injury in football (soccer). BMJ Open Sport Exerc Med. 5(1):e000505. online. doi: 10.1136/bmjsem-2018-000505.
- Borg DN, Nguyen R, Tierney NJ. 2022. Missing data: current practice in football research and recommendations for improvement. Sci Med Footb. 6(2):262–267. doi: 10.1080/24733938.2021.1922739.
- Buchheit M, King R, Stokes A, Lemaire B, Grainger A, Brennan D, Norman D, Mukinen A, Ruggiero H, Shelton A, et al. 2023. Return to play following injuries in pro football: insights into the real-life practice of 85 elite practitioners around diagnostics, progression strategies and reintegration processes. Sport Perform Sci Rep. 1:1–20. https://sportperfsci.com/return-to-play-following-injuries-in-pro-football-insights-into-the-real-life-practices-of-85-elite-practitioners-around-diagnostics-progression-strategies-and-reintegration-processes/.
- Buckthorpe M, Della Villa F, Della Villa S, Roi G. 2019a. On-field rehabilitation part 1: 4 pillars of high-quality on-field rehabilitation are restoring movement quality, physical conditioning, restoring sport-specific skills, and progressively developing chronic training load. J Orthop Sport Phys. 49(8):565–569. doi: 10.2519/jospt.2019.8954.
- Buckthorpe M, Della Villa F, Della Villa S, Roi G. 2019b. On-field rehabilitation part 2: a 5-stage program for the soccer player focused on linear movements, multidirectional movements, soccer-specific skills, soccer-specific movements, and modified practice. J Orthop Sport Phys. 49(8):570–575. doi: 10.2519/jospt.2019.8952.
- Buckthorpe M, Frizziero A, Roi G. 2019. Update on functional recovery process for the injured athlete: return to sport continuum redefined. Br J Sport Med. 53(5):265–267. doi: 10.1136/bjsports-2018-099341.
- Coutts AJ. 2017. Challenges in developing evidence-based practice in high-performance sport. Int J Sport Physiol. 12(6):717–718. doi: 10.1123/IJSPP.2017-0455.
- Delaney J, Duthie G, Thornton H, Pyne D. 2018. Quantifying the relationship between internal and external work in team sports: development of a novel training efficiency index. Sci Med Footb. 2(2):149–156. doi: 10.1080/24733938.2018.1432885.
- Delaney J, Wileman T, Perry N, Thornton H, Moresi M, Duthie G. 2019. The validity of a global navigation satellite system for quantifying small-area team-sport movements. J Strength Cond Res. 33(6):1463–1466. doi: 10.1519/jsc.0000000000003157.
- Dijkstra HP, Pollock N, Chakraverty R, Ardern C. 2017. Return to play in elite sport: a shared decision-making process. Br J Sport Med. 51(5):419–420. doi: 10.1136/bjsports-2016-096209.
- Dunlop G, Ardern C, Andersen TE, Lewin C, Dupont G, Ashworth B, O’Driscoll G, Rolls A, Brown S, McCall A. 2020. Return-to-play practices following hamstring injury: a worldwide survey of 131 Premier League Football Teams. Sports Med. 50(4):829–840. doi: 10.1007/s40279-019-01199-2.
- Ekstrand J, Krutsch W, Spreco A, Van Zoest W, Roberts C, Meyer T, Bengtsson H. 2020. Time before return to play for the most common injuries in professional football: a 16-year follow-up of the UEFA Elite Club injury study. Br J Sports Med. 54(7):421–426. doi: 10.1136/bjsports-2019-100666.
- Ekstrand J, Lundqvist D, Davison M, D’Hooghe M, Pensgaard AM. 2019. Communication quality between the medical team and the head coach/manager is associated with injury burden and player availability in elite football clubs. Br J Sport Med. 53(5):304–308. doi: 10.1136/bjsports-2018-099411.
- Ekstrand J, Spreco A, Bengtsson H, Bahr R. 2021. Injury rates decreased in men’s professional football: an 18-year prospective cohort study of almost 12 000 injuries sustained during 1.8 million hours of play. Br J Sport Med. 55(19):1084–1091. doi: 10.1136/bjsports-2020-103159.
- Eliakim E, Morgulev E, Lidor R, Meckel Y. 2020. Estimation of injury costs: financial damage of english premier league teams’ underachievement due to injuries. BMJ Open Sport Exerc Med. 6(1):e000675. doi: 10.1136/bmjsem-2019-000675.
- Elo S, Kyngäs H. 2008. The qualitative content analysis process. J Adv Nurs. 62(1):107–115. doi: 10.1111/j.1365-2648.2007.04569.x.
- Fanchini M, Steendahl IB, Impellizzeri FM, Pruna R, Dupont G, Coutts AJ, Meyer T, McCall A. 2020. Exercise-based strategies to prevent muscle injury in elite footballers: a systematic review and best evidence synthesis. Sports Med. 50(9):1653–1666. Springer. doi: 10.1007/s40279-020-01282-z.
- Field A, Harper LD, Chrismas BCR, Fowler PM, McCall A, Paul DJ, Chamari K, Taylor L. 2021. The use of recovery strategies in professional soccer: a worldwide survey. Int J Sport Physiol. 16(12):1804–1815. doi: 10.1123/ijspp.2020-0799.
- Gabbett TJ. 2016. The training-injury prevention paradox: should athletes be training smarter and harder? Br J Sports Med. 50(5):273–280. doi: 10.1136/bjsports-2015-095788.
- Ghrairi M, Loney T, Pruna R, Malliaropoulos N, Valle X. 2019. Effect of poor cooperation between coaching and medical staff on muscle re-injury in professional football over 15 seasons. Open Access J Sports. 10:107–113. doi: 10.2147/OAJSM.S221292.
- Gray D. 2021. Doing research in the real world. 5th ed. London: Sage.
- Gregson W, Carling C, Gualtieri A, O’Brien J, Reilly P, Tavares F, Bonanno D, Lopez E, Marques J, Lolli L, et al. 2022. A survey of organizational structure and operational practices of elite youth football academies and national federations from around the world: a performance and medical perspective. Front Sport Act Living. 4. online. doi:10.3389/fspor.2022.1031721.
- Hägglund M, Waldén M, Bengtsson H, Ekstrand J. 2018. Re-injuries in professional football: the UEFA elite club injury study. In: Musahl, V, Karlsson, J, Krutsch, W, Mandelbaum, BR, Espregueira-Mendes, J, d’Hooghe, P, editors. Return to play in football: an evidence-based approach. Berlin Heidelberg: Springer-Verlag; p. 953–962.
- Harper DJ, Carling C, Kiely J. 2019. High-intensity acceleration and deceleration demands in elite team sports competitive match play: a systematic review and meta-analysis of observational studies. Sport Med. 49(12):1923–1947. doi: 10.1007/s40279-019-01170-1.
- Hostrup M, Bangsbo J. 2023. Performance adaptations to intensified training in top-level football. Sport Med. 53(3):577–594. doi: 10.1007/s40279-022-01791-z.
- Impellizzeri F, Tenan M, Kempton T, Novak A, Coutts A. 2020. Acute: chronic workload ratio: conceptual issues and fundamental pitfalls. Int J Sport Physiol. 15(6):907–913. doi: 10.1123/ijspp.2019-0864.
- Impellizzeri F, Ward P, Coutts A, Bornn L, McCall A. 2020. Training load and injury part 2: questionable research practices hijack the truth and mislead well-intentioned clinicians. J Orthop Sport Phys. 50(10):577–584. doi: 10.2519/jospt.2020.9211.
- Impellizzeri F, Woodcock S, Coutts A, Fanchini M, McCall A, Vigotsky A. 2020. Acute to random workload ratio is “as” associated with injury as acute to actual chronic workload ratio: time to dismiss ACWR and its components. SportRxiv. 3. doi: 10.31236/osf.io/e8kt4.
- Krosnick J, Presser S. 2010. Questions and questionnaire design. In: Marsden, PV, Wright, JD, editors. Handbook of Survey Research. 2nd ed. Bingley, UK: Emerald Group Publishing; p. 263–313.
- López-Valenciano A, Ruiz-Pérez I, Garcia-Gómez A, Vera-Garcia FJ, De Ste Croix M, Myer GD, Ayala F. 2020. Epidemiology of injuries in professional football: a systematic review and meta-analysis. Br J Sport Med. 54(12):711–718. doi: 10.1136/bjsports-2018-099577.
- McCall A, Carling C, Nedelec M, Davison M, Le Gall F, Berthoin S, Dupont G. 2014. Risk factors, testing and preventative strategies for non-contact injuries in professional football: current perceptions and practices of 44 teams from various premier leagues. Br J Sport Med. 48(18):1352–1357. doi: 10.1136/bjsports-2014-093439.
- McCall A, Dupont G, Ekstrand J. 2016. Injury prevention strategies, coach compliance and player adherence of 33 of the UEFA Elite Club injury Study teams: a survey of teams’ head medical officers. Br J Sport Med. 50(12):725–730. doi: 10.1136/bjsports-2015-095259.
- Taberner M, Allen T, Cohen DD. 2019. Progressing rehabilitation after injury: consider the “control-chaos continuum”. Br J Sport Med. 53(18):1132–1136. doi: 10.1136/bjsports-2018-100157.
- Taberner M, Allen T, O’Keefe J, Cohen DD. 2022. Contextual considerations using the ′control-chaos continuum′ for return to sport in elite football - part 1: load planning. Phys Ther Sport. 53:67–74. doi: 10.1016/j.ptsp.2021.10.015.
- Taberner M, Haddad F, Dunn A, Newall A, Parker L, Betancur E, Cohen D. 2020. Managing the return to sport of the elite footballer following semimembranosus reconstruction. BMJ Open Sport Exerc Med. 6(1):e000898. online. doi: 10.1136/bmjsem-2020-000898.
- Taberner M, van Dyk N, Allen T, Drust C, Richter B, Cohen D. 2020. Physical preparation and return to performance of an elite female football player following ACL reconstruction: a journey to the FIFA Women’s World Cup. BMJ Open Sport Exerc Med. 6(1):e000843. online. doi: 10.1136/bmjsem-2020-000843.
- Taberner M, van Dyk N, Allen T, Richter C, Howarth C, Scott S, Cohen D. 2019. Physical preparation and return to sport of the football player with a tibia-fibula fracture: applying the ‘control-chaos continuum’. BMJ Open Sport Exerc Med. 5(1):1–7. doi: 10.1136/bmjsem-2019-000639.
- Verheul J, Nedergaard NJ, Vanrenterghem J, Robinson MA. 2020. Measuring biomechanical loads in team sports – from lab to field. Sci Med Footb. 1–7. doi: 10.1080/24733938.2019.1709654.
- Wright C, Atkins S, Jones B. 2012. An analysis of elite coaches’ engagement with performance analysis services (match, notational analysis and technique analysis). Int J Perform Anal Sport. 12(2):436–451. doi: 10.1080/24748668.2012.11868609.