
Abstract
Background
Interventions involving diet, physical activity, and breathing exercises are shown to be beneficial in managing both fatigue and quality of life (QoL) related to MS; however, the impact of such interventions among people newly diagnosed with clinically isolated syndrome (CIS) or relapsing-remitting multiple sclerosis (RRMS) who decline disease-modifying therapies (DMTs) is unknown.
Methods
A 12-month prospective quasi-experimental non-inferiority trial recruited people newly diagnosed with CIS or RRMS who voluntarily declined DMTs (health behavior group; HB, n = 29) or followed standard of care (SOC, n = 15). Participants in the HB group were remotely coached on the study diet, moderate-intensity walking, and breathing exercises. All participants completed questionnaires validated to assess MS symptoms, including perceived mental and physical QoL (MSQOL54); fatigue (Fatigue Severity Scale, FSS; and Modified Fatigue Impact Scale, MFIS); mood (Hospital Anxiety and Depression Scale, HADS); and cognitive function (Perceived Deficits Questionnaire, PDQ).
Results
During the 12 months, the HB group experienced improvement in scores for mental QoL (MSQOL54 – Mental, 0.24, 95% CI 0.01, 0.47; p = 0.04), fatigue (Total MFIS, −7.26, 95% CI −13.3,-1.18; p = 0.02), and perceived cognitive function (Total PDQ, PDQ–Attention, PDQ–Promemory, and PDQ–Planning, p ≤ 0.03 for all). A between-group difference was observed only for PDQ–Planning (p = 0.048). Non-inferiority analysis revealed that the 12-month changes in means for the HB group were not worse than those for the SOC group with respect to fatigue (FSS, p = 0.02), mood (HDS–Anxiety, p = 0.02; HADS–Depression, p < 0.0001), physical QoL (MSQOL54 – Physical, p = 0.02), or cognitive dysfunction (Total PDQ, p = 0.01).
Conclusion
The multimodal lifestyle intervention for individuals newly diagnosed with CIS or RRMS, who voluntarily decline DMTs, did not yield patient-reported outcomes worse than those observed in the SOC group regarding perceived mental quality of life, mood, fatigue, and cognitive function.
Trial Registration
clinicaltrials.gov identifier: NCT04009005.
Introduction
Multiple sclerosis (MS) is a chronic neurodegenerative disease that affects 2.8 million people worldwide.Citation1 Many people who develop MS first experience a single demyelinating event of the central nervous system; this stage is termed clinically isolated syndrome (CIS). After a second demyelinating event, a relapse, the individual can be described as having relapsing-remitting MS (RRMS) once this diagnosis is confirmed by their treating neurologist through MRI and the 2017 McDonald criteria.Citation2 RRMS is the most common type of MS, accounting for approximately 85–90% of new MS cases.Citation3 Over time, people with RRMS experience additional relapses and increased loss of function.Citation4
Drug-based disease-modifying therapies (DMTs) significantly lower relapse rates in 29–68% of individuals with MS who have been treated with these therapies;Citation5 however, surveys have indicated that up to 31% of people with MS do not start treatment with DMTs.Citation6 Reasons for declining DMT treatments include high costs,Citation7 concerns about side-effects,Citation6 and a lack of insurance coverage.Citation8 Among people with MS, there is a trend toward decreased trust in pharmacological interventions and a growing interest in more holistic approaches to treatments, specifically related to diet, exercise, and emotional wellness.Citation9 In surveys, most individuals with MS report implementing some form of complementary and alternative care, either combining with DMTs or independently.Citation10 Understanding the effects of lifestyle programs in people with MS who are voluntarily DMT-naïve will be necessary for predicting the clinical course of patients.
Physical activity recommendations for people with MS encourage greater than or equal to 150 min/week of lifestyle physical activity while adapting exercise activities based on an individual’s needs and capacity, as well as personal preferences.Citation11 Several meta-analyses have shown that physical activity improves cognitive function,Citation12 depressive symptoms,Citation13 and quality of life (QoL).Citation14 Similarly, mindfulness practices, such as breathing exercises or meditative activities, have been shown to improve fatigueCitation15 and cognition,Citation16 as well as reduce self-reported emotion dysregulation.Citation17 While evidence regarding the value of therapeutic diets alone remains inconsistent,Citation18 a recent network meta-analysis revealed that patients on the Paleolithic diet showed greater improvements in mental and physical QoL than controls.Citation19 In people with RRMS, the Paleolithic diet has been associated with significant reductions (both statistically and clinically) in fatigue and increases in mental and physical QoL at 12 and 24 weeks.Citation20 Although each of these interventions individually yields beneficial effects, the combination of these health behavioral modifications has the potential to enhance the QoL for newly diagnosed individuals with MS.
Prior studies investigating the effects of a multimodal intervention consisting of a modified Paleolithic diet, supplementation of specific nutrients, strengthening exercises of core and lower limb muscles along with neuromuscular electrical stimulation, and stress reduction techniques (self-massage and meditation) showed that this approach led to clinically significant improvements in perceived fatigue, mood, gait, and the expression of metabolic biomarkers in people with progressive MS who most adhere to the intervention.Citation21–23 Although the clinical usefulness of changes in diet, physical activity, and breathing exercises as adjunct therapies for MS symptoms is encouraging, their combined effects on the disease course in the absence of DMTs remain unknown. Thus, the efficacy in people who are newly diagnosed with MS and have declined DMTs remains unclear. This study aimed to assess the effect of a remotely administered, multimodal intervention including study diet, walking program, and breathing exercise on QoL in DMT-naive people newly diagnosed with CIS and RRMS, comparing them to counterparts who had the same diagnosis but opted to receive the standard of care (SOC) treatments.
Participants and Methods
Study Design
A single-center quasi-experimental study was conducted at the University of Iowa Hospitals and Clinics Prevention Intervention Center. A quasi-experimental study design was selected because of ethical concerns about withholding FDA-approved treatments for RRMS.Citation24 Due to the Coronavirus 2019 (COVID-19) pandemic, restrictions prevented in-person research visits during the spring of 2020, when this study was initiated. Thus, planned brain imaging, blood biomarkers, and onsite clinical assessments were omitted from the study procedures. All visits were remote, and outcomes were patient-reported. This study was conducted in accordance with the principles of the Declaration of Helsinki. The protocol was approved by the University of Iowa Institutional Review Board (IRB #201908778). The study is registered at clinicaltrials.gov, with the identifier: NCT04009005.
Study Participants
Signed documentation of the informed consent process was obtained from all participants before they enrolled. Participants were recruited from the continental United States via social media posts, email blasts, and flyers sent to local neurology clinics. Recruitment started in May 2020 and was completed in August 2021. Inclusion criteria were as follows: 1) a diagnosis of RRMS or CIS according to the 2017 McDonald criteria,Citation2 2) confirmed by the treating neurologist no more than 12 months before the first study visit was completed; 3) between 18 and 55 years of age at the time of consent; 4) consent to share the clinical notes from the primary care and neurology providers during the study period; 5) residence within the continental United States; 6) approval of enrollment by the treating neurologist.
Exclusion criteria for all participants included 1) moderate or severe cognitive impairment as measured by the Short Portable Mental Health Questionnaire;Citation25 2) use of insulin or Coumadin medication; 3) history of oxalate kidney stones, schizophrenia, or active diagnosis of an eating disorder; 4) time elapsed since initial diagnosis of RRMS or CIS greater than 12 months. Additional group-specific eligibility criteria can be found in Supplemental Table 1. Importantly, participants in the intervention group had to have voluntarily declined DMTs, prior to screening for the study.
For clinical pilot trials, inclusion of more than 10 participants per group is adequate;Citation26 therefore, we aimed to recruit more than 10 individuals per group.
Health Behaviors (HB) Group
Upon enrollment, participants in the HB group received education on the multimodal intervention, which consisted of a modified Paleolithic elimination diet, 4-7-8 breathing exercises, and a moderate-intensity walking program. The HB group participants were scheduled for a medical history review and education session with the study’s principal investigator (PI; TLW). The education module included information on the potential mechanisms by which diet, aerobic exercise, and stress reduction can influence patient-reported symptoms and comorbid disease processes. Participants were subsequently contacted through the Zoom platform by a registered dietitian nutritionist (RDN; LB), who is a credentialed nutrition expert, for the study and provided with an orientation session about the study diet, walking, and stress reduction programs. The RDN was trained in motivational interviewing and self-determination theory,Citation27–29 which emphasize patient-centered goals through the use of open-ended questions, and applied these frameworks during interactions with all study participants. After the first month was completed, participants were encouraged to attend monthly group support calls with their study peers monitored by the RDN and other research team members. The monthly group support calls entailed participants leading discussions regarding the modifications made during the intervention, such as sharing cooking recipes, offering moral support to other participants, or asking questions. The RDN answered questions and consulted with the study PI, physical therapist (PT; BB), and other study team members whenever needed. Participants received phone, email, and text support from RDN as needed.
Modified Paleolithic Elimination Diet
The study RDN instructed participants in the HB intervention group on the modified Paleolithic elimination diet, which included 6–9 combined servings of fruits and vegetables per day and 9–12 ounces of meat per day for petite women and 12–21 ounces of meat per day for men and tall women, with the exact amount determined based on gender and size. All gluten-containing grains, legumes, eggs, and dairy (except for clarified butter or ghee) were excluded, and nightshades (eg, tomatoes, white potatoes, eggplant, peppers, and seed spices) were excluded following the first three months on the diet. If the participant desired to reintroduce nightshades into the diet, this was done during months 7–9, under observation by the study team, to test tolerance and provide guidance if changes might be necessary. After problematic foods were identified during months 7–9, participants followed their personalized modified Paleolithic elimination diet (months 10–12).
Stress Reduction Using Mindfulness-Based Breathing
The participants were provided a video that provided instructions to reduce stress each day by using the “4-7-8” breathing technique, in which the participant inhales through the nose for a count of 4, holds their breath for a count of 7, and then exhales entirely through the mouth for a count of 8. The video also instructed participants to avoid tightening their muscles while holding their breath. Participants who experienced discomfort while holding their breath for 7 seconds could adjust the breathing pattern for personal comfort while ensuring that the exhalation lasted longer than the inhalation. Participants were instructed to perform this exercise daily for a minimum of 1 minute, but they could do additional 4-7-8 sessions as desired.
Moderate-Intensity Walking Program
Participants were instructed to walk at a moderately brisk pace. To ensure proper form, participants were given access to an instructional video demonstrating walking at a moderate intensity. The video not only illustrated the correct walking technique but also imparted knowledge about the advantages of walking and offered guidance on seamlessly integrating walking into their everyday schedule. Walking for at least 10 minutes was considered one session, and participants could accumulate as many sessions in a day as they would like. Furthermore, participants were advised to aim for a weekly total of 150 minutes of walking and to prevent excessive fatigue by not walking for more than 60 minutes at a time.
Self-Reported Adherence to Study Components
At the 12-month time point, participants in the HB group were asked whether they followed each component throughout the intervention, including the study diet, breathing exercises, and 10-minute walking regimen. This was done using Research Electronic Data Capture (REDCap),Citation30,Citation31 a secure, web-based software platform designed to support data capture for research studies. Participants who confirmed their compliance with all components were classified as adherent.
Standard of Care (SOC) Group
The SOC group was not provided with advice or education about any component of multimodal intervention. However, to ensure that participants remained engaged with the study team, they were sent monthly emails containing information on the latest MS research that was not related to diet, physical activity, or stress reduction in MS. The study team did not restrict any changes in health-behaviors of SOC participants, if they decide to do so by themselves.
Outcomes
Study outcomes were assessed using validated questionnaires. The primary outcomes were MS-specific physical and mental QoL, which were evaluated using the MS Quality of Life 54 (MSQoL54).Citation32 The secondary outcomes included minutes of physical activity, assessed using the International Physical Activity Questionnaire-Long Form (IPAQ);Citation33 mood, specifically anxiety and depression, assessed using the Hospital Anxiety and Depression Scale (HADS);Citation34 perceived fatigue, assessed using the Fatigue Severity Scale (FSS)Citation35 and the Modified Fatigue Impact Scale (MFIS);Citation35 and cognitive dysfunction, assessed using the Perceived Deficits Questionnaire (PDQ) including Total PDQ, PDQ – Attention, PDQ – Retromemory, PDQ – Promemory, and PDQ – Planning.Citation36
An adverse event was recorded whenever a participant reported one via phone, text, email, or REDCap online survey, as well as when one was documented in the participant’s medical records. Additionally, side effects were self-reported monthly, via a questionnaire using the MyCap application; this can be downloaded on smartphones, and answers are integrated into the respective REDCap project. Diet-related, serious, and other adverse events determined to require additional attention were forwarded to the medical monitor, who reviewed the issue and determined appropriate follow-up. Self-reported relapses were assessed in the End of Study Survey distributed to participants at 12 months. Self-reported COVID-19 infection was evaluated during the End of Study Call or through email at the 12-month timepoint.
Statistical Analysis
Data were checked for accuracy and possible entry errors. Continuous variables were evaluated for normality by graphical observation. At enrollment, descriptive statistics for each variable were calculated by the treatment group, using frequencies and percentages or means and standard errors (SE). Baseline characteristics of treatment groups were compared using Fisher’s exact test for categorical variables and using a two-sample t-test for continuous variables. Missing observations were omitted from baseline comparisons.
Rates of adverse event outcomes (eg, relapse, COVID-19 infection) were reported as treatment-stratified counts and percentages. Outcome measures collected for the HB and SOC groups were assessed for differences using Fisher’s exact test.
Within- and between-treatment changes in outcomes over time were tested using the linear mixed modeling (LMM)Citation37 framework. All models include fixed effects for the treatment group, time, and their interaction. The models also specify a random effect for participants to account for repeated measures. Point estimates, 95% confidence intervals, and p-values for mean changes in outcome measures over time were generated for each outcome. For all estimates, the significance was assessed at the α = 0.05 level. Cohen’s d, also known as the standardized mean difference, was calculated to assess the magnitude of the within-group changes. A Cohen’s d score of zero means that the treatment and comparison agent have no differences in effect, whereas the absolute value above zero indicates the degree to which one treatment is more efficacious than the other.Citation38
To determine whether the HB intervention was not worse than SOC at 12-months,Citation39 a non-inferiority analysis was conducted for mental and physical QoL, fatigue, mood, and perceived cognitive difficulties outcomes. Margins used for the non-inferiority analysis of each outcome were based on statistical consideration from summarizing the historical evidence; subsequently, a clinical judgment then made by a neurologist (JK) was used to select the margin.Citation40 At 12 months, the mean change margin of non-inferiority for mental and physical QoL was 0.25 units,Citation41 FSS was 0.9 units,Citation42 Total MFIS was 8 units,Citation42,Citation43 HADS – Anxiety was 2.08 units,Citation44,Citation45 HADS – Depression was 2.8 units,Citation44,Citation45 and Total PDQ was 3 units.Citation46
All analyses were performed with two-sided tests (α = 0.05) using SAS software (version 9.4, SAS Institute, Inc.).
Results
A total of 44 participants enrolled in the trial, including 29 in the HB (n = 29) and 15 in the SOC (n = 15) groups (). During the 12-month study period, 5 participants in the HB were lost to attrition; among these, 1 withdrew due to a new health concern (unrelated to the intervention or MS), and 4 were lost to follow-up. In the SOC group, 2 participants were lost to follow-up (). At baseline, none of the characteristics assessed differed significantly between the groups ().
Table 1 Baseline Characteristics of Study Participants in the Health Behaviors (HB) and Standard of Care (SOC) Groupsa
Figure 1 Diagram illustrating participant recruitment and study flow for health behaviors (HB) intervention and standard of care (SOC) groups. *An additional breakdown of ineligibility criteria is available in the Supplemental Material. Reasons for ineligibility or exclusion may not add up to the value of ineligible or excluded because some participants were found ineligible or were excluded for multiple reasons. †Recruitment stopped due to COVID-19 pandemic.
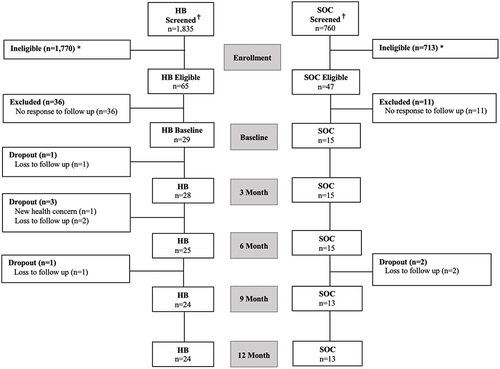
Participants in the HB group self-reported adherence to all components of the study intervention at the end of the study were follows: 95.8% for diet (23/24), 91.7% for physical activity (22/24), and 75% for breathing exercises (18/24). However, 4 participants (16.7%) self-reported starting a DMT during the study course, with 1 of those participants withdrawing from the study due to a new health concern (unrelated to the intervention or MS). In the SOC group, 4 participants reported changing or reducing the dose of their DMTs during the study (Supplemental Table 2), as well as 38.5% (5/13) of participants self-reported beginning a specific diet during the study period, with 15.4% (2/13) starting the Paleolithic diet and 23.1% (3/13) starting the Wahls diet.
In terms of adverse events, at the 12-month timepoint, differences between the groups were non-significant (Supplemental Table 3). Self-reported relapse occurred in 16.7% of participants in the HB group (4/24) and in 7.1% of those in the SOC group (1/14) (p = 0.63). Similarly, the incidence of self-reported COVID-19 cases was 37.5% of participants in the HB group (9/24), and 7.7% of participants in the SOC group (1/13) (p = 0.07). Additionally, no serious adverse events (ie, requiring medical monitoring intervention) were reported for either the HB (Supplemental Table 4) or SOC group (Supplemental Table 5).
The mean scores of the self-reported outcomes were assessed at baseline and 12-months, with within-group changes assessed from baseline to 12-months. The HB group showed a favorable statistically significant mean increase from baseline for mental QoL, as assessed by MSQoL-54 – Mental composite score (4.08 ± 0.13; p = 0.04; ). In contrast, the SOC group exhibited favorable improvements from baseline in physical QoL, as assessed by MSQoL-54 – Physical composite score (2.87 ± 0.04; p = 0.049; ). However, the HB group exhibited an unfavorable reduction in minutes of vigorous activity, as assessed by IPAQ – Vigorous MET (580.00 ± 298.84; p = 0.007; ), whereas the SOC group exhibited a favorable mean decrease in physical activity fatigue, as assessed by MFIS – Physical value (8.54 ± 2.95; p = 0.008; ). For the HB group, the HADS–Anxiety mean value showed a favorable decrease in anxiety (6.63 ± 0.84; p = 0.009); whereas the HADS–Depression value showed a favorable reduction in depressive symptoms in only the SOC group (2.69 ± 0.94; p = 0.02; ). For the HB group, the mean fatigue score favorably decreased, as assessed by Total MFIS and MFIS – Cognitive (25.29 ± 4.28; p = 0.02; 12.75 ± 2.17, p = 0.002; respectively, ), and the mean of cognitive dysfunction was favorably reduced from that at baseline, as assessed Total PDQ, PDQ – Attention, PDQ – Promemory, and PDQ – Planning (p ≤ 0.03 for all; ). Additional mean outcomes for months 3, 6, and 9 are presented in Supplemental Table 6.
Table 2 Baseline and 12-Month Outcome Means and Magnitude of Mean Change for the Health Behaviors (HB) Intervention and Standard of Care (SOC) Groups
The magnitude of mean change for the outcomes was assessed to compare the response of the intervention from baseline to 12-months. For the HB group, the magnitude of mean change had favorable increases for mental QoL, as assessed by MSQoL54 (0.24, 95% CI 0.01, 0.47; p = 0.04; ). In contrast, the SOC group had a favorable magnitude of mean increase for physical QoL, as evaluated by MSQoL54 – Physical (0.12, 95% CI 0.00, 0.24; p = 0.049; ). The HB group had a favorable decrease in the mean magnitude of change for the anxiety score, as assessed HADS – Anxiety value (−1.75, 95% CI −3.08, −0.43; p = 0.009), whereas, only the SOC group showed a favorable reduction in the mean magnitude of change in the depression score, as evaluated by HADS – Depression value (−0.93, 95% CI −2.91, 1.05; p = 0.009; ). In the HB group, the magnitude of mean change in minutes of vigorous activity was unfavorable, as assessed IPAQ – Vigorous MET (0.30, 95% CI 0.12, 0.72; p = 0.007; ). The magnitude of mean change in fatigue differed meaningfully only for the HB group, as evaluated Total MFIS and MFIS – cognitive values (−7.26, 95% CI −13.34, −1.18; p = 0.02; and −4.59, 95% CI −7.56, −1.63; p = 0.002; respectively; ). For the HB group, the magnitude of the change in cognitive dysfunction was favorable, as assessed by Total PDQ and all PDQ subdomains, except for PDQ – Retromemory (p ≤ 0.03 for all). No statistically significant difference in the magnitude of mean between groups was observed for any outcome from baseline to 12-months (p > 0.05), except for PDQ – Planning (p = 0.048; ). A medium effect size was observed for PDQ – Planning with a Cohen’s d of −0.59 ().
Non-inferiority between-group differences revealed that the 12-month change in mean for the HB group was not worse than that for the SOC for MSQOL54 – Physical QoL by a margin of 0.25 units (p = 0.02), HADS – Anxiety by a margin of 2.08 units (p = 0.02), HADS – Depression by a margin of 2.8 units (p < 0.0001), FSS by a margin of 0.9 units (p = 0.02), and Total PDQ by a margin of 3 units (p = 0.01) ().
Discussion
The results of the 12-month comparison of a remotely delivered multimodal intervention (diet, breathing exercises, and walking program) for individuals who were newly diagnosed with RRMS or CIS and were voluntarily DMT-naïve revealed that the mean changes for key symptoms of MS, including perceived fatigue, QoL, mood, and cognition, are not worse than those for the participants in the SOC group, who were taking DMTs. Thus, newly diagnosed individuals with RRMS or CIS who voluntarily decline DMTs may benefit from a diet and lifestyle behavioral intervention for the management of MS-related symptoms. However, the mechanisms that contribute to these beneficial effects, as well as whether such a therapy has an impact on relapse rate and disease progression, remain unclear.
This study indicates that interest in therapeutic diet and lifestyle modifications is generally high among individuals with MS. This was evident from the self-reported adherence of the HB participants to the study diet, ie, the modified Paleolithic diet, being 95.8% at the 12-month intervention timepoint. This is higher than a previous study reporting 80% adherence after 3.5 months.Citation47 The high adherence to the diet could potentially be explained by the continued support from the study RDNs throughout the duration of the present study. RDNs are qualified to provide personalized medical nutrition therapy; thus, they can help people with MS, especially those newly diagnosed with RRMS or CIS, develop resilience and adaptive strategies regarding food literacy through these patient-centered support strategies.Citation48 A second line of support for an interest in diet modifications is that, although members of the SOC group were not provided with information on a special diet, 38.5% reported starting a specific diet during the course of the study. Therefore, newly diagnosed people with RRMS or CIS may benefit from having RDNs as part of their MS care team, regardless of whether they opt to receive a DMT to support diet or dietary modifications, as part of either a complementary or alternative treatment.
The multimodal intervention in the HB group resulted in a significant magnitude of mean changes from baseline to 12 months for perceived fatigue, mental QoL, mood, and cognition. Moreover, the non-inferiority analysis revealed that the 12-month change in mean values for fatigue, mood physical QoL, and cognitive difficulties in HB participants were not worse than that for SOC for the aforementioned outcomes. These findings corroborate the conclusions from a prior multimodal intervention in individuals with MS, ie, that increased engagement in healthy eating habits and physical activity (self-reported) is related to reduced fatigue, perceived stress, and depression, as well as improved cognitive health.Citation49 Similarly, results from a study of multimodal lifestyle modifications, which included a plant-based diet very low in saturated fat, omega-3 fatty acids supplementation, increased physical activity, and the use of stress reduction techniques, such as meditation, included improvements in health behaviors outcomes (assessed using mental health and QoL assessments), and maintenance of these lifestyle changes over a 3-year follow-up.Citation50 Findings from both a prior multimodal intervention study that included a Paleolithic dietCitation23 and a study of a low-fat dietary interventionCitation51 also suggest that lifestyle modifications can have favorable effects on cognitive function. Thus, our study corroborates the notion that interventions based on diet and behavior modifications have the potential to reduce perceived fatigue and cognition problems, as well as improve mental and physical QoL and mood in individuals who are newly diagnosed with RRMS or CIS who decline DMTs.
Although physical activity is an established component of rehabilitation for people with MS,Citation11,Citation52 the physical activity scores of the HB intervention group in the current study did not improve. Despite the high self-reported adherence to walking program component of the intervention, the HB group participant’s vigorous minutes of activity exhibited a significant unfavorable decrease at 12-months from baseline. It is possible that the COVID-19 pandemic, which coincided with the current study, greatly impacted the participants’ physical activity. This would be consistent with the effects of decreased physical activity observed in people with MS in other studies during the pandemic.Citation53,Citation54 Additionally, a systematic review of 13 studies evaluating the impact of COVID-19 on physical activity among people with neurological diseases, including MS, reported that COVID-19 had a negative impact on levels of physical activity.Citation55 Home isolation and quarantining may have led to decreased physical activity and increased sedentary behavior in the current study.Citation53
This is the first study to have assessed the effects of diet and behavioral interventions on QoL among people with MS who voluntarily decline DMTs. Strengths of this study include high study adherence (to diet, 95.8%; and to physical activity, 91.7%) among participants in the intervention group and robust analytical methods. Although the design did not include randomization, a quasi-experimental study design was necessary because DMTs are efficacious and FDA-approved for reducing relapse risk and slowing disease progression.Citation5 Randomizing individuals with MS to a group in which DMTs are withheld would have been unethical.Citation24 Thus, it was necessary to recruit participants who have MS but voluntarily declined DMT treatment prior to enrollment, which is a limitation of the study. Another limitation is the small study size, which may have skewed the outcomes and adverse events measured; further research will be necessary to confirm these results and to understand the physiological underpinnings of the present study’s findings. However, the measures used did capture the perspectives of individuals regarding living with their disease or treatments and perceived wellness, and these may not be captured otherwise.Citation56 Moreover, the side effects associated with DMTs may reduce the QoL in the SOC group, contributing to the difference in QoL seen between groups. These side effects underscore the reason why many individuals with MS opt to reject the utilization of DMTs. Additionally, it is important to consider the potential impact of volunteer bias on the initiation of a specific diet concurrent with DMTs within the SOC group. The observed behavior may stem from the high motivation characteristic of individuals inclined to participate in research studies, thereby limiting the generalizability of the findings. However, studies show that around 40% of individuals report making dietary modifications after their diagnosis,Citation57 especially 1-year following diagnosis.Citation58 Lastly, the fact that the current study coincided with the COVID-19 pandemic likely also affected the perceptions of QoL and other self-reported measures, such as physical activity.Citation59 Future investigations would benefit from a combination of self-reporting and clinical and objectively measurable outcomes data. This would provide a more complete understanding of the multimodal intervention’s effects.
Remote delivery of a multimodal diet and lifestyle behavioral intervention may improve perceived QoL, mood, fatigue, and cognition among newly diagnosed individuals with RRMS or CIS who are voluntarily DMT-naive. The implication is that individuals reluctant to use DMTs (because of cost, potential medication related-adverse events, possible pregnancy, or breastfeeding), may benefit from adopting dietary, breathing practice, and physical activity lifestyle behavioral modifications to reduce MS-related fatigue and improve QoL. However, further research is necessary to understand the feasibility and efficacy of diet and lifestyle modifications influence MS relapse rates, disease severity, and disease progression among individuals with newly diagnosed RMSS or CIS who decline DMTs. The results from this study support the need for continued exploration of the impact of diet and lifestyle modifications on MS-related outcomes, disease severity, and disease progression, especially in those who voluntarily decline DMT therapy.
Data Sharing Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to containing information that could compromise the privacy of research participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Conflict of Interest Disclosures: Dr Terry Wahls personally follows and promotes the Wahls™ diet. She has equity interest in the following companies: Terry Wahls LLC; TZ Press LLC; The Wahls Institute, PLC; FBB Biomed Inc.; Levels Health Inc., and the website http://www.terrywahls.com. She also owns the copyright to the books Minding My Mitochondria (2nd Edition) and The Wahls Protocol, The Wahls Protocol Cooking for Life, and the trademarks The Wahls Protocol® and Wahls™ diet, Wahls Paleo™ diet, and Wahls Paleo Plus™ diets. She has completed grant funding from the National Multiple Sclerosis Society for the Dietary Approaches to Treating Multiple Sclerosis Related Fatigue Study. She has financial relationships with Vibrant America LLC, Standard Process Inc., MasterHealth Technologies Inc., Foogal Inc., and the Institute for Functional Medicine Inc. She receives royalty payments from Penguin Random House. Dr Wahls has conflict-of-interest management plans in place with the University of Iowa and the Iowa City Veteran’s Affairs Medical Center. This study received funding from Dr Terry Wahls LLC. The funder had the following involvement with the study: study design, the writing of this article, and the decision to submit it for publication. Also, Dr Tyler Titcomb received Fellowship fund that supported me for this study from the Carter Chapman Shreve Family Foundation, during the conduct of the study.
All authors declare no other competing interests.
Acknowledgments
The authors want to acknowledge the University of Iowa students who supported recruitment and data acquisition, Christine Blaumueller for her editing assistance, and thank the study participants for their dedication and commitment to the study intervention.
Additional information
Funding
References
- Walton C, King R, Rechtman L, et al. Rising prevalence of multiple sclerosis worldwide: insights from the Atlas of MS, third edition. Mult Scler. 2020;26(14):1816–1821. doi:10.1177/1352458520970841
- Thompson AJ, Banwell BL, Barkhof F, et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018;17(2):162–173. doi:10.1016/S1474-4422(17)30470-2
- Goodin DS. The epidemiology of multiple sclerosis: insights to disease pathogenesis. Handb Clin Neurol. 2014;122:231–266. doi:10.1016/B978-0-444-52001-2.00010-8
- Dobson R, Giovannoni G. Multiple sclerosis - A review. Eur J Neurol. 2019;26(1):27–40. doi:10.1111/ene.13819
- Thompson AJ, Baranzini SE, Geurts J, Hemmer B, Ciccarelli O. Multiple sclerosis. Lancet. 2018;391(10130):1622–1636. doi:10.1016/S0140-6736(18)30481-1
- Stratos K, McGarragle K, Thistle J, Vyas MV, Lee L. Non-compliance with disease modifying therapies in patients with Multiple Sclerosis: a qualitative analysis. Mult Scler Relat Disord. 2020;41:102016. doi:10.1016/j.msard.2020.102016
- Hartung DM, Bourdette DN, Ahmed SM, Whitham RH. The cost of multiple sclerosis drugs in the US and the pharmaceutical industry: too big to fail? Neurology. 2015;84(21):2185–2192. doi:10.1212/WNL.0000000000001608
- Wang G, Marrie RA, Salter AR, et al. Health insurance affects the use of disease-modifying therapy in multiple sclerosis. Neurology. 2016;87(4):365–374. doi:10.1212/WNL.0000000000002887
- Dunn M, Bhargava P, Kalb R. Your patients with multiple sclerosis have set wellness as a high priority-and the national multiple sclerosis society is responding. US Neurol. 2015;11(2):80–86.
- Silbermann E, Senders A, Wooliscroft L, et al. Cross-sectional survey of complementary and alternative medicine used in Oregon and Southwest Washington to treat multiple sclerosis: a 17-Year update. Mult Scler Relat Disord. 2020;41:102041. doi:10.1016/j.msard.2020.102041
- Kalb R, Brown TR, Coote S, et al. Exercise and lifestyle physical activity recommendations for people with multiple sclerosis throughout the disease course. Mult Scler. 2020;26(12):1459–1469. doi:10.1177/1352458520915629
- Li G, You Q, Hou X, et al. The effect of exercise on cognitive function in people with multiple sclerosis: a systematic review and meta-analysis of randomized controlled trials. J Neurol. 2023;270(6):2908–2923. doi:10.1007/s00415-023-11649-7
- Dalgas U, Stenager E, Sloth M, Stenager E. The effect of exercise on depressive symptoms in multiple sclerosis based on a meta-analysis and critical review of the literature. Eur J Neurol. 2015;22(3):443–e34. doi:10.1111/ene.12576
- Flores VA, Šilić P, DuBose NG, Zheng P, Jeng B, Motl RW. Effects of aerobic, resistance, and combined exercise training on health-related quality of life in multiple sclerosis: systematic review and meta-analysis. Mult Scler Relat Disord. 2023;75:104746. doi:10.1016/j.msard.2023.104746
- Gilbertson RM, Klatt MD. Mindfulness in motion for people with multiple sclerosis: a feasibility study. Int J MS Care. 2017;19(5):225–231. doi:10.7224/1537-2073.2015-095
- Manglani HR, Samimy S, Schirda B, Nicholas JA, Prakash RS. Effects of 4-week mindfulness training versus adaptive cognitive training on processing speed and working memory in multiple sclerosis. Neuropsychology. 2020;34(5):591–604. doi:10.1037/neu0000633
- Schirda B, Duraney E, Lee HK, et al. Mindfulness training for emotion dysregulation in multiple sclerosis: a pilot randomized controlled trial. Rehabilitation Psychology. 2020;65(3):206–218. doi:10.1037/rep0000324
- Evans E, Levasseur V, Cross AH, Piccio L. An overview of the current state of evidence for the role of specific diets in multiple sclerosis. Mult Scler Relat Disord. 2019;36:101393. doi:10.1016/j.msard.2019.101393
- Snetselaar LG, Cheek JJ, Fox SS, et al. Efficacy of diet on fatigue and quality of life in multiple sclerosis: a systematic review and Network Meta-analysis of Randomized Trials. Neurology. 2023;100(4):e357–e366. doi:10.1212/WNL.0000000000201371.
- Wahls TL, Titcomb TJ, Bisht B, et al. Impact of the Swank and Wahls elimination dietary interventions on fatigue and quality of life in relapsing-remitting multiple sclerosis: the WAVES randomized parallel-arm clinical trial. Mult Scler J Exp Transl Clin. 2021;7(3):20552173211035399. doi:10.1177/20552173211035399
- Bisht B, Darling WG, White EC, et al. Effects of a multimodal intervention on gait and balance of subjects with progressive multiple sclerosis: a prospective longitudinal pilot study. Degener Neurol Neuromuscul Dis. 2017;7:79–93. doi:10.2147/dnnd.S128872
- Fellows maxwell K, Wahls T, Browne RW, et al. Lipid profile is associated with decreased fatigue in individuals with progressive multiple sclerosis following a diet-based intervention: results from a pilot study. PLoS One. 2019;14(6):e0218075. doi:10.1371/journal.pone.0218075
- Lee JE, Bisht B, Hall MJ, et al. A multimodal, nonpharmacologic intervention improves mood and cognitive function in people with multiple sclerosis. J Am Coll Nutr. 2017;36(3):150–168. doi:10.1080/07315724.2016.1255160
- Bärnighausen T, Tugwell P, Røttingen JA, et al. Quasi-experimental study designs series-paper 4: uses and value. J Clin Epidemiol. 2017;89:21–29. doi:10.1016/j.jclinepi.2017.03.012
- Pfeiffer E. A short portable mental status questionnaire for the assessment of organic brain deficit in elderly patients. J Am Geriatr Soc. 1975;23(10):433–441. doi:10.1111/j.1532-5415.1975.tb00927.x
- Hertzog MA. Considerations in determining sample size for pilot studies. Research in Nursing & Health. 2008;31(2):180–191. doi:10.1002/nur.20247
- Miller WR, Rose GS. Toward a theory of motivational interviewing. Am Psychol. 2009;64(6):527–537. doi:10.1037/a0016830
- Patrick H, Williams GC. Self-determination theory: its application to health behavior and complementarity with motivational interviewing. Int J Behav Nutr Phys Act. 2012;9:18. doi:10.1186/1479-5868-9-18
- Deci EL, Ryan RM. The “what” and “why” of goal pursuits: human needs and the self-determination of behavior. PSYCHOL INQ. 2000;11(4):227–268. doi:10.1207/S15327965PLI1104_01
- Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. 2019;95:103208. doi:10.1016/j.jbi.2019.103208
- Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)--A metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. doi:10.1016/j.jbi.2008.08.010
- Vickrey BG, Hays RD, Harooni R, Myers LW, Ellison GW. A health-related quality of life measure for multiple sclerosis. Qual Life Res. 1995;4(3):187–206. doi:10.1007/BF02260859
- Myers J, Bader D, Madhavan R, Froelicher V. Validation of a specific activity questionnaire to estimate exercise tolerance in patients referred for exercise testing. Am Heart J. 2001;142(6):1041–1046. doi:10.1067/mhj.2001.118740
- Watson TM, Ford E, Worthington E, Lincoln NB. Validation of mood measures for people with multiple sclerosis. Int J MS Care. 2014;16(2):105–109. doi:10.7224/1537-2073.2013-013
- Rooney S, McFadyen DA, Wood DL, Moffat DF, Paul PL. Minimally important difference of the fatigue severity scale and modified fatigue impact scale in people with multiple sclerosis. Mult Scler Relat Disord. 2019;35:158–163. doi:10.1016/j.msard.2019.07.028
- Strober LB, Binder A, Nikelshpur OM, Chiaravalloti N, DeLuca J. The perceived deficits questionnaire: perception, deficit, or distress? Int J MS Care. 2016;18(4):183–190. doi:10.7224/1537-2073.2015-028
- Zuur AF, Ieno EN, Walker NJ, Saveliev AA, Smith GM. Mixed Effects Models and Extensions in Ecology with R. Springer; 2009.
- McGough JJ, Faraone SV. Estimating the size of treatment effects: moving beyond p values. Psychiatry. 2009;6(10):21–29.
- Schumi J, Wittes JT. Through the looking glass: understanding non-inferiority. Trials. 2011;12:106. doi:10.1186/1745-6215-12-106
- Althunian TA, de Boer A, Groenwold RHH, Klungel OH. Defining the noninferiority margin and analysing noninferiority: an overview. Br J Clin Pharmacol. 2017;83(8):1636–1642. doi:10.1111/bcp.13280
- Kappos L, Gold R, Arnold DL, et al. Quality of life outcomes with BG-12 (dimethyl fumarate) in patients with relapsing-remitting multiple sclerosis: the DEFINE study. Mult Scler. 2014;20(2):243–252. doi:10.1177/1352458513507817
- Wilken J, Traboulsee A, Nelson F, et al. Longitudinal assessment of neurocognitive function in people with relapsing multiple sclerosis initiating alemtuzumab in routine clinical practice: LEM-COG study results. Mult Scler Relat Disord. 2023;73:104677. doi:10.1016/j.msard.2023.104677
- Plow M, Packer T, Mathiowetz VG, et al. REFRESH protocol: a non-inferiority randomised clinical trial comparing internet and teleconference to in-person ‘Managing Fatigue’ interventions on the impact of fatigue among persons with multiple sclerosis. BMJ Open. 2020;10(8):e035470. doi:10.1136/bmjopen-2019-035470
- Horton EJ, Mitchell KE, Johnson-Warrington V, et al. Comparison of a structured home-based rehabilitation programme with conventional supervised pulmonary rehabilitation: a randomised non-inferiority trial. Thorax. 2018;73(1):29–36. doi:10.1136/thoraxjnl-2016-208506
- Smyth P, Watson KE, Al Hamarneh YN, Tsuyuki RT. The effect of nurse practitioner (NP-led) care on health-related quality of life in people with multiple sclerosis – a randomized trial. BMC Neurol. 2022;22(1):1–275. doi:10.1186/s12883-022-02809-9
- Akbar N, Turpin K, Petrin J, Smyth P, Finlayson M. A pilot mixed-methods evaluation of MS INFoRm: a self-directed fatigue management resource for individuals with multiple sclerosis. INT J REHABIL RES. 2018;41(2):114–121. doi:10.1097/MRR.0000000000000271
- Irish AK, Erickson CM, Wahls TL, Snetselaar LG, Darling WG. Randomized control trial evaluation of a modified Paleolithic dietary intervention in the treatment of relapsing-remitting multiple sclerosis: a pilot study. Degener Neurol Neuromuscul Dis. 2017;7:1–18. doi:10.2147/dnnd.S116949
- Titcomb TJ, Bostick M, Obeidat AZ. Opinion: the role of the registered dietitian nutritionist in multiple sclerosis care in the United States. Front Neurol. 2023;14:1068358. doi:10.3389/fneur.2023.1068358
- Strober LB, Becker A, Randolph JJ. Role of positive lifestyle activities on mood, cognition, well-being, and disease characteristics in multiple sclerosis. Applied Neuropsychology: Adult. 2018;25(4):304–311. doi:10.1080/23279095.2018.1458518
- Marck CH, De Livera AM, Brown CR, et al. Health outcomes and adherence to a healthy lifestyle after a multimodal intervention in people with multiple sclerosis: three year follow-up. PLoS One. 2018;13(5):e0197759. doi:10.1371/journal.pone.0197759
- Weinstock-Guttman B, Baier M, Park Y, et al. Low fat dietary intervention with omega-3 fatty acid supplementation in multiple sclerosis patients. Prostaglandins Leukot Essent Fatty Acids. 2005;73(5):397–404. doi:10.1016/j.plefa.2005.05.024
- Kim Y, Lai B, Mehta T, et al. Exercise training guidelines for multiple sclerosis, stroke, and Parkinson disease: rapid review and synthesis. Am J Phys Med Rehabil. 2019;98(7):613–621. doi:10.1097/phm.0000000000001174
- Kalron A, Dolev M, Greenberg-Abrahami M, et al. Physical activity behavior in people with multiple sclerosis during the COVID-19 pandemic in Israel: results of an online survey. Mult Scler Relat Disord. 2021;47:102603. doi:10.1016/j.msard.2020.102603
- Matysiak M, Siger M, Walczak A, Ciach A, Jonakowski M, Stasiołek M. The influence of COVID-19 pandemic lockdown on the physical activity of people with multiple sclerosis. The role of online training. Mult Scler Relat Disord. 2022;63:103843. doi:10.1016/j.msard.2022.103843
- Abasıyanık Z, Kurt M, Kahraman T. COVID-19 and physical activity behaviour in people with neurological diseases: a systematic review. J Dev Phys Disabil. 2022;34(6):987–1012. doi:10.1007/s10882-022-09836-x
- Weinfurt KP, Reeve BB. Patient-reported outcome measures in clinical research. JAMA. 2022;328(5):472–473. doi:10.1001/jama.2022.11238
- Riemann-Lorenz K, Eilers M, von Geldern G, Schulz KH, Köpke S, Heesen C. Dietary interventions in multiple sclerosis: development and pilot-testing of an evidence based patient education program. PLoS One. 2016;11(10):e0165246. doi:10.1371/journal.pone.0165246
- Russell RD, Lucas RM, Brennan V, Sherriff JL, Begley A, Black LJ. Reported changes in dietary behavior following a first clinical diagnosis of central nervous system demyelination. Front Neurol. 2018;9:161. doi:10.3389/fneur.2018.00161
- Weinstein SM, Reilly E, Garland N, Zimmerman V, Jacobs D. Impact of a virtual wellness program on quality of life measures for patients living with multiple sclerosis during the COVID-19 Pandemic. Int J MS Care. 2022;24(6):282–286. doi:10.7224/1537-2073.2021-134