
ABSTRACT
Background
Dyadic interventions for health behaviour change involving the romantic partner are promising. However, it often remains unclear how exactly the partner is involved in dyadic interventions. We propose a novel compendium of dyadic intervention techniques (DITs) that facilitates systematic description of dyadic interventions in terms of who performs what for whom during intervention delivery and subsequent implementation.
Objective
We aimed to systematically characterise dyadic interventions along their degree of partner involvement and to provide a comprehensive list of DITs used in dyadic interventions with romantic partners.
Methods
We systematically reviewed dyadic health behaviour change interventions with controlled designs. We included 165 studies describing 122 distinct dyadic interventions with romantic partners. Interventions were classified along their degree of partner involvement, 160 DITs were extracted, and their frequencies of use counted.
Results
The majority of interventions (n = 90, 74%) explicitly instructed partners to interact. Half of the DITs were performed jointly by the couple and also targeted the couple. Mostly, couples were instructed to jointly practice communication skills and to jointly perform problem solving for the couple.
Discussion
The present review contributes to the development of a shared and systematic way of describing dyadic interventions to facilitate cumulation of evidence.
Background
There is consistent evidence that social relationships have a protective role for health: Individuals lacking social ties are physically and mentally less healthy and more likely to die prematurely than socially integrated individuals (Holt-Lunstad, Citation2021; Holt-Lunstad et al., Citation2010). Romantic relationships, being the most important and intimate personal relationships during the adult lifespan, seem to have a particularly relevant role in influencing health (Holt-Lunstad et al., Citation2008, Citation2010). Interestingly, having a supportive network cannot compensate for worse health outcomes in unmarried or unhappily married individuals (Holt-Lunstad et al., Citation2008, Citation2010). Moreover, prior studies showed that health behaviours tend to correspond between romantic partners (Myers Virtue et al., Citation2015; Torvik et al., Citation2013) and that health behaviour change in one partner is positively linked to health behaviour change in the other partner (Jackson et al., Citation2015). This suggests that partners shape each other’s health behaviours and may facilitate health behaviour change.
Although dyadic interventions for health behaviour change involving the romantic partner seem promising, the varying levels of detail and lack of systematic labelling in intervention descriptions have impeded a clear understanding of how exactly partners are involved in these interventions. Therefore, the present review aims to systematically describe dyadic intervention techniques used in health behaviour change interventions with romantic couples. This will help to facilitate systematic reporting and evidence synthesis of dyadic interventions. Moreover, the present review serves as a starting point for the development of an agreed-upon and theory-based compendium of dyadic intervention techniques that will also facilitate the development of theory-based dyadic interventions in the future (for further information on the project, please see: https://OSF.io/r43v6/).
In recent years, there has been a rise in dyadic intervention studies that attempt to leverage the romantic partner for health behaviour change (e.g., Berli et al., Citation2016; Burkert et al., Citation2011; Knoll et al., Citation2017; Prestwich et al., Citation2014). For example, some dyadic interventions focus on extending self-regulation processes to the level of the romantic dyad, such as collaborative implementation intentions (Prestwich et al., Citation2014), dyadic planning (Burkert et al., Citation2011; Knoll et al., Citation2017), or dyadic action control (Berli et al., Citation2016). Others focus more specifically on enhancing social support, for example in smoking cessation (e.g., Faseru et al., Citation2018; McBride et al., Citation2004). Several systematic reviews and meta-analyses demonstrate positive effects across both the increase of health-enhancing behaviours such as physical activity (Carr et al., Citation2019) and the reduction of health-compromising behaviours such as sedentary behaviour (Carr et al., Citation2019; Richards et al., Citation2017), sexual risk behaviours (Burton et al., Citation2010), or substance use (O'Farrell & Schein, Citation2011). Moreover, results of meta-analyses showed improved effectiveness of couple-based interventions compared to individual interventions, although effect sizes are usually small and dependent on the type of dyad (Carr et al., Citation2019). Overall, accumulating evidence in the literature indicates that couple-based interventions appear to be a promising approach for changing health behaviours.
However, reviews also indicate a pronounced heterogeneity in couple-based interventions regarding their intervention design, intervention implementation and comparison conditions (Arden-Close & McGrath, Citation2017; Burton et al., Citation2010). Due to varying levels of detail in the reporting of intervention content in dyadic intervention studies and unsystematic labelling of intervention techniques, little is known about how exactly partners are involved and which intervention techniques and underlying mechanisms make those interventions successful (Arden-Close & McGrath, Citation2017; Burton et al., Citation2010; Carr et al., Citation2019). For instance, reviews of dyadic intervention studies showed that only few studies reported the use of specific couple-based intervention techniques (Arden-Close & McGrath, Citation2017). Carr et al. (Citation2019) provided detailed information in their meta-analysis on how dyadic interventions were delivered, how they were structured, and whether dyad members had shared goals; however, the intervention content and the involvement of the partner in the intervention were not discussed.
Thus, despite the fact that evidence on the effectiveness of dyadic interventions is increasing, potential active ingredients of such interventions, including for instance, the specific roles and involvement of the couple members, still remain unknown. So far, this might also be due to a lack of a common language for describing dyadic interventions or intervention techniques including the interaction within the dyad. This precludes comparability between studies and creates a barrier for reviews and meta-analyses synthesising the effectiveness of dyadic involvement in couple-based interventions. The present systematic review aims to establish a reporting standard of dyadic intervention content which accounts for the varying roles and involvement of each dyad member in dyadic interventions.
Types of dyadic interventions
Given the specific nature of dyadic interventions involving two persons, it is important to understand which partner the intervention focuses on (e.g., see also Richards et al., Citation2017) and what specific roles partners have during intervention delivery and subsequent implementation. Prior literature on dyadic health behaviour change suggests that the degree of partner involvement represents a meaningful characteristic when differentiating dyadic intervention content (Baucom et al., Citation1998; Martire et al., Citation2010). Joint efforts in behaviour change are assumed to allow couples to draw more efficiently from their joint pool of resources, in contrast to individual efforts that are supported or assisted by the other partner (Fitzsimons et al., Citation2015; Lewis et al., Citation2006; Lyons et al., Citation1998). The perception of, for example, a chronic illness of one partner as a shared problem or the adherence to HIV medication as a shared goal that affects the couple as a whole, is assumed to enhance motivation for cooperative action, enhance mutual support, and reduce individual coping efforts (Fitzsimons et al., Citation2015; Lewis et al., Citation2006; Lyons et al., Citation1998). A stronger personal involvement of romantic partners during the intervention delivery or subsequent implementation could be an enabling factor for improved behaviour change. In this review, we propose a compendium that aims to systematise the detailed reporting of dyadic intervention techniques (i.e., who performs what for whom). Such detailed dyadic intervention description may encompass vital information concerning potential moderator effects in the efficacy of dyadic interventions (e.g., joint techniques that are executed together might be more effective than techniques that are not executed together).
Currently, there is no universally accepted and consistently applied definition of dyadic interventions, resulting in different interpretations depending on context, study, and intervention design. For example, even at the level of systematic reviews different criteria to refer to dyadic interventions as interventions that actively or directly involve the other partner are used. Whereas in some reviews ‘involvement of the partner’ remained unspecified (Arden-Close & McGrath, Citation2017; Baucom et al., Citation2012; Brandão et al., Citation2014; Richards et al., Citation2017; Shaffer et al., Citation2020), other reviews included dyadic interventions where both romantic partners were present at the intervention (Buck et al., Citation2018). To investigate dyadic interventions, it is important to create a shared language and agreed-upon criteria defining a dyadic intervention. We refer to dyadic interventions as explicitly addressing both members of a dyad as part of the intervention, with a range of techniques targeting either one (focus person or partner) or both partners to change at least one dyad member’s health behaviour. Interventions may thus range from partners simply sharing presence to explicitly interacting with each other.
In order to account for the various ways in which partners can be involved in behaviour change interventions, Scholz et al. (Citation2020) suggested a classification of dyadic interventions according to their degree of partner involvement during intervention delivery and subsequent implementation. The framework can be used to classify interventions into different prototypes of dyadic interventions and to distinguish between intervention techniques that focus on one versus two partners. The types of dyadic interventions can be classified into two overarching categories: (1) Interventions in which both partners receive an intervention and/or are present during an intervention, but the two partners do not explicitly interact with each other (i.e., shared presence), and (2) interventions in which the dyad is explicitly asked to interact with or refer to each other in some way (i.e., instructed interaction) (see for definitions and examples). Interventions categorised as (1) shared presence include interventions in which (a) the partner is merely present, i.e., both partners attend the intervention, but at least one partner has no active role or task and receives information only passively (i.e., mere presence) or (b) interventions in which both partners perform a task in parallel without interaction between each other (i.e., parallel). Prior research suggests that social proximity might affect important determinants of health behaviour change in focus persons and their partners, such as self-efficacy or emotion regulation (Aron & Aron, Citation1986; Beckes & Coan, Citation2011). Thus, dyadic interventions only describing the mere presence of the partner should be conceptualised as distinct from individual interventions regarding the processes they might initiate. Building on the original framework by Scholz et al. (Citation2020), we classified interventions in which the partner is merely present as a type of dyadic intervention with the lowest degree of partner involvement (see ). Interventions categorised as (2) instructed interaction include interventions that are (a) directed at one partner who is explicitly asked to interact with or refer to the other partner during intervention delivery or subsequent implementation (i.e., cross-over) or interventions that (b) actively involve both partners in the intervention task (i.e., joint, see ). Depending on the type of dyadic intervention, different intervention techniques can be used. Interventions categorised as (1) shared presence may include any technique that involves only one partner. Interventions categorised as (2) instructed interaction may include any technique that involves an interaction with or reference to the other partner, either directed at one partner or both (see ).
Figure 1. Continuum of dyadic interventions.
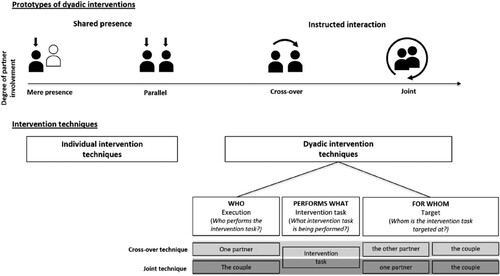
Table 1. Definitions and examples of different prototypes of dyadic interventions.
Intervention techniques in dyadic interventions
In recent years, considerable effort has been devoted to systematically identify and classify intervention techniques (e.g., Bartholomew et al., Citation2006; Kok et al., Citation2016; Michie et al., Citation2013). Existing taxonomies such as the behaviour change taxonomy (BCT; Michie et al., Citation2013) or the intervention mapping taxonomy (IM taxonomy; Kok et al., Citation2016) fundamentally contributed to behaviour change research. They have facilitated the accumulation of evidence across contexts and the development of theory- and evidence-based interventions (Bartholomew et al., Citation2006; Kok et al., Citation2016; Michie et al., Citation2013). However, the majority of behaviour change techniques identified in existing taxonomies are at the level of the individual (e.g., goal setting, self-monitoring) and those behaviour change techniques that do involve an interaction with a non-professional dyad member to change health behaviour are still under-represented or not well differentiated in existing taxonomies. In the original BCT taxonomy (Michie et al., Citation2013), for example, the differentiation of ‘social support’ in unspecified, practical and emotional support only broadly addresses different forms of support. This is despite the fact that reviews on support interventions (e.g., Hogan et al., Citation2002) suggest that there is considerable variation in the approach and concepts of support used. In the intervention mapping taxonomy, the role of others (i.e., environmental agents) is more explicitly considered and processes of social support and social influence are differentiated in more detail. However, other social exchange processes, such as communal coping (Lyons et al., Citation1998), companionship (Lüscher et al., Citation2022; Rook, Citation1987), or social control (Lewis & Rook, Citation1999; Scholz et al., Citation2021) that have been introduced more than two decades ago, are not or not fully considered. Thus, taxonomies of individual behaviour change (e.g., Kok et al., Citation2016; Michie et al., Citation2013) provide an excellent starting point for identifying potential dyadic intervention techniques. Yet, a more differentiated view that considers important features of behaviour change techniques that are unique to the dyadic context (e.g., who performs a specific task for whom) is needed. Importantly, we argue that dyadic intervention techniques are more than a specific (i.e., dyadic) delivery mode of individual intervention techniques. Rather, intervention techniques involving dyadic interaction are unique in terms of their intervention content (e.g., setting a joint goal is distinct from setting an individual goal) and should thus be explicitly identified.
Further, dyadic intervention techniques can be linked to different determinants underlying behaviour change. So far, no model or theory of dyadic behaviour change exists that comprehensively addresses all the different determinants underlying dyadic behaviour change. For this reason, we used a meta-framework, the theoretical domains framework (TDF), outlining overarching theoretical domains that were derived from synthesising theoretical constructs from 33 theories related to behaviour change (Atkins et al., Citation2017; Cane et al., Citation2012). For instance, theoretical constructs such as social support, social comparison, or learning/modelling are nested in the domain ‘social influences’, whereas theoretical constructs such as action planning or self-monitoring are nested in the domain ‘behavioral regulation’. Although not specific for the dyadic context, the TDF comprehensively describes related theoretical constructs of behaviour change nested in overarching domains and therefore provides a heuristic model that can also be used to structure and categorise dyadic behaviour change techniques. In the present paper and as suggested by Kok et al. (Citation2016) we refer to theoretical constructs that predict behaviour change as determinants.
To systematically classify dyadic intervention techniques, the specific nature of dyadic intervention techniques needs to be considered. We define a dyadic intervention technique (DIT) to change behaviours as an observable and replicable intervention technique that explicitly involves any form of interaction with, or clear reference to, a non-professional dyad member to change behaviour. The technique specifies who performs what for whom during intervention delivery or subsequent implementation. The fact that two participants versus one participant are involved in an intervention technique yields the need to explicitly state the role and involvement of each dyad member in who is performing the intervention task and also whom the intervention task is targeted at to account for the increased level of complexity. Thus, each dyadic intervention technique can be divided into different components: (1) the execution level of the intervention task within the dyad (i.e., who performs the intervention task?), that describes two possible ways an intervention task can be completed by the dyad members: alone by one partner or together by the dyad. (2) the intervention task itself (i.e., what intervention task is being performed?), and (3) the target level of the intervention task (i.e., whom is the intervention task targeted at?) that defines whom the content of the intervention task is targeted at: one partner, the other partner or the couple, for instance whose problem is attempted to be solved or whose goal is being agreed upon.
The execution level of a technique defines whether it is a cross-over technique or a joint technique (see ). Cross-over techniques are always executed by one partner alone (i.e., execution level) and targeted at either the other partner or the couple (i.e., target level). Moreover, cross-over techniques can also be performed simultaneously or in response to the other partner. This means that cross-over techniques can be performed mutually by both partners. For example, both partners can reciprocally provide support for the respective other partner (i.e., mutual cross-over technique). Joint techniques are performed by the couple (i.e., execution level) and target either one partner or the couple (i.e., target level). Joint techniques that target one partner can just as well be performed mutually (i.e., mutual joint technique). For example, the couple can jointly (i.e., execution level) create a plan (i.e., intervention task) for one partner (i.e., target level) and subsequently do the same for the other partner (i.e., target level).
Different combinations of the execution level (i.e., who performs the intervention task?) and target level (i.e., whom is the intervention task targeted at?), allow each intervention task (i.e., what intervention task is being performed?) to be potentially implemented as four dyadic intervention techniques since each combination of execution level, intervention task, and target level is referred to as a unique dyadic intervention technique. For example, the intervention task plans for can, at the execution level, be performed by one partner (i.e., one partner plans alone) or by the couple (i.e., the couple plans together). Further, if one partner plans alone, the plan can either be targeted at the other partner (i.e., the partner who did not plan is supposed to enact the plan) or the couple (i.e., the couple is supposed to enact the plan together). Similarly, if the couple plans together, the plans themselves can either target one partner (i.e., one partner of the dyad is supposed to enact the plan alone) or the couple (i.e., the couple is supposed to enact the plan together). The couple (i.e., execution level) plans (i.e., intervention task) for one partner (i.e., target level) is also known as dyadic planning (Knoll et al., Citation2017) or we-for-me plans (Kulis et al., Citation2022a). The couple (i.e., execution level) plans (i.e., intervention task) for the couple (i.e., target level) are also known as collaborative implementation intentions (Prestwich et al., Citation2012) or we-for-us plans (Kulis et al., Citation2022a). It is important to note that, depending on the intervention task, the four theoretically possible combinations of execution level, intervention task, and target level may not always make sense or may not have been implemented so far.
Objectives
As reviewed above, although a considerable number of dyadic health behaviour change interventions have been conducted, no systematic classification and common language of dyadic intervention techniques exist. So far, active ingredients of dyadic behaviour change interventions are far from understood and most dyadic interventions do not specify partner involvement (i.e., mere presence, parallel, cross-over, joint) or how exactly the intervention techniques were conducted (i.e., execution level, intervention task, target level). Existing taxonomies of behaviour change techniques do not sufficiently cover dyadic intervention techniques including who performs what for whom. The present review contributes to the development of a shared and systematic way of reporting and describing dyadic interventions and their intervention content. This will facilitate cumulative evidence synthesis in the long run. It will also serve as a starting point for an agreed-upon and theory-based compendium of dyadic intervention techniques that can be used for intervention development (for further information on the project, please see: https://OSF.io/r43v6/).
Therefore, the primary objectives of this review are to summarise the current literature on dyadic interventions with romantic couples that aim to change one or both partners’ health-enhancing (e.g., physical activity, nutrition) or health-compromising behaviour (e.g., smoking, alcohol consumption). More specifically, we aimed to (1) characterise dyadic interventions according to their degree of partner involvement (i.e., mere presence, parallel, cross-over, joint), and to (2) provide a comprehensive list of dyadic intervention techniques used in interventions within a framework classifying execution level, intervention task, and target level.
Method
The systematic review was conducted in compliance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA; Page et al., Citation2021) guidelines. The protocol of the systematic review is registered with the Prospective Register of Systematic Reviews database (ID number: CRD42021261622; July 2021, available from: https://www.crd.york.ac.uk/prospero/display_record.php?ID = CRD42021261622).
Search strategy
A comprehensive and systematic literature search was conducted in July 2021 across five electronic databases: EMBASE, Scopus, PsycINFO, PubMed, and Web of Science (Core Collection). Search terms focused on the following concepts critical to the research question: ‘intervention’, ‘romantic couple’, and ‘health behaviour’ including different health-enhancing (i.e., ‘physical activity’, ‘healthy diet’, ‘medication adherence’) and health-compromising (i.e., ‘smoking’, ‘alcohol consumption’, ‘sexual behaviors’) behaviours. Terms were mapped to controlled vocabulary (e.g., MeSH terms) whenever possible and Boolean operators were used to combine the concepts. The search terms were discussed and agreed upon by all project partners and reviewed by a scientific librarian at the University of Zurich (see Supplement S1 for an example search term for the database: Web of Science (Core Collection)). No limitation was set on publication status (published, unpublished, in press, or in progress) or publication period. Identified related studies, study protocols, and relevant systematic reviews and meta-analyses were also searched to identify other potentially eligible studies. Authors of included studies were contacted to identify any further unpublished literature and ongoing studies and/or to obtain additional information on relevant studies.
Inclusion and exclusion criteria
Studies were eligible for inclusion if they focused on (1) a dyadic intervention for (2) couples or romantic partners to (3) change a health-enhancing (e.g., physical activity, nutrition) and/or health-compromising behaviour (e.g., smoking, alcohol consumption). Dyadic interventions were defined as interventions explicitly addressing both members of a dyad as part of the intervention covering different types of dyadic interventions as displayed in (see also Scholz et al., Citation2020). Only intervention studies using a controlled design with at least one control condition were eligible. Randomisation was not mandatory (e.g., RCT, non-randomised trials, quasi-experimental trials) and no restriction on the type of comparison condition (e.g., active or passive control group) was made.
There were no restrictions on the age of the participants, sexual orientation, setting, or location of the study. Studies were excluded if they involved other types of dyads (e.g., mother–child, friends, health professional-patient), if the intervention addressed more people besides the romantic partner (e.g., other family members) or if studies did not only involve the romantic partner but ‘others’ in general, if no health behaviour was addressed (e.g., if only a health outcome such as weight, mental health, wellbeing, distress, or relationship satisfaction was addressed), if the study design was only correlational, or if the study was published in any other language than English.
Data selection and extraction
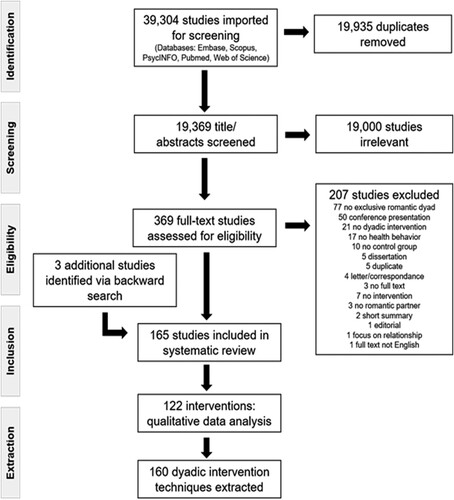
Results of database searches were imported into the Covidence© systematic review software (Veritas Health Innovation, Melbourne, Australia, available at www.covidence.org) and duplicates were removed. Records were double-screened independently by the two lead authors (SD and KV) and trained student research assistants in a comprehensive two-step process: (1) all identified titles and abstracts were screened against the pre-specified inclusion criteria (yes, maybe, no), and (2) full texts of potentially eligible publications were obtained and screened for inclusion (yes, no). Any disagreement regarding eligibility was resolved through discussions between three of the authors (SD, KV, and CB) under the consultation of the other authors until a consensus was reached. As a much greater percentage of studies was excluded than included in the title/abstract screening, an adjusted kappa was calculated to account for the unbalanced distribution (Byrt et al., Citation1993). Interrater reliability of both title/abstract screening and full-text screening was high with an adjusted kappa of PABAK = 0.97 for the title/abstract screening and Cohen’s kappa = 0.88 for the full-text screening. displays a PRISMA flowchart for the study selection process. To obtain as much detail as possible on the content and instructions of each intervention, we contacted the first authors of each included study requesting additional intervention materials and descriptions.
Figure 2. Prisma flowchart of the study selection process.
Data were systematically extracted following the ‘template for intervention description and replication’ (TIDieR; Hoffmann et al., Citation2014) and a custom-designed data extraction form implemented in Covidence©. All available information (i.e., original paper and study protocol, connected papers, and additional material provided by authors) was reviewed to extract relevant details. Data extraction included information on key study characteristics (e.g., study design and setting), the definition of romantic partners, relationship duration and partner´s role/task in the intervention, participant characteristics, intervention characteristics, and intervention description, health behaviour context/target behaviour, and outcomes of the study. Data were extracted and coded by two trained student research assistants independently and one of the lead authors (SD or KV) double-checked the form for accuracy and completeness. Any disagreement was resolved by discussion between three of the authors (SD, KV, and CB) under the consultation of the rest of the author team.
Risk of bias assessment
As the aim of the present systematic review was to comprehensively describe dyadic intervention techniques and not to assess effects of the interventions, risk of bias of the included studies was not conducted.
Classification of the degree of partner involvement
Following data extraction, the degree of partner involvement was classified according to the continuum of dyadic interventions (see ) independently by the two lead authors (SD and KV) and any disagreement was resolved by consensus. For classification, all available information (i.e., original paper and study protocol, connected papers, and additional material provided by authors) was used. Partner involvement and interaction between partners were not unequivocally identifiable in all interventions. For example, some interventions did not provide detailed information on role and interaction of partners, solely stating that couples received couple counseling together without describing the content of the sessions or the role of each partner (n = 4), or stating that the couple participated in the intervention as part of a bigger group without describing the partners’ specific interaction (n = 4). Those interventions were conservatively classified as ‘mere presence’. Classification followed a hierarchical order, e.g., if at least one interaction between partners was identified, the study was classified as a dyadic intervention with ‘instructed interaction’ (see ). Frequencies of publication dates, targeted health behaviours, and partner characteristics for each prototype of dyadic intervention (i.e., mere presence, parallel, cross-over, joint) were counted and differences between prototypes regarding these characteristics were tested using the Fisher’s exact test, considering different samples sizes across prototypes of dyadic interventions.
Extraction of specific dyadic intervention techniques
As the aim of this systematic review was the identification and classification of dyadic intervention techniques that explicitly involved both partners of the dyad, in a second step of data extraction, we focused solely on interventions including a form of instructed interaction between partners (see ), i.e., interventions with at least one cross-over technique or joint technique, to extract specific dyadic intervention techniques. Studies describing the same intervention were grouped together. The response rate of all contacted authors (n = 128) for additional materials was 36% (n = 46). Overall, 16% (n = 21) sent additional materials on intervention descriptions.
To extract and identify dyadic intervention techniques, any intervention description that included either an instruction for one or both partners to interact or an instruction to refer to one partner or the dyad was extracted by the two lead authors (SD and KV) and trained student research assistants. Intervention descriptions were taken from the original papers, and if available from study protocols, connected papers and additional material provided by the authors. Extracted information was combined and reviewed by the two lead authors (SD and KV) and a primary list of labels of dyadic intervention techniques was created in an iterative process identifying distinct techniques across studies. Feedback from the other authors was obtained at several timepoints and incorporated into the process. Consensus on the list of dyadic intervention techniques was reached via discussions with the author team.
Finally, two trained student assistants reassigned – independently from each other – all extracted examples from each intervention included in the review to the final list of labels of dyadic intervention techniques, and one of the lead authors (SD or KV) resolved any disagreement.
Extracted dyadic intervention techniques were clustered according to their theoretical determinants (e.g., planning, modelling, social control) and sorted according to the domains of the theoretical domains framework (Atkins et al., Citation2017; Cane et al., Citation2012). Further, dyadic intervention techniques were mapped and, where applicable, named according to wording and labels identified and described in existing individual health behaviour change taxonomies by Kok et al. (Citation2016) and Michie et al. (Citation2013). References to these taxonomies (Kok et al., Citation2016; Michie et al., Citation2013) are marked in the notes.
Counts of each dyadic intervention technique (i.e., each combination of execution level, intervention task, target level) identified in the literature were indicated using a greyscale, with darker shades indicating higher counts in the cells of the respective dyadic intervention technique. If dyadic intervention techniques were applied mutually in the reviewed literature, i.e., a technique performed reciprocally by both partners, the respective cell was marked with an asterisk (see ).
Table 2. Compendium of dyadic intervention techniques to change health behaviours.
Results
The flow diagram () outlines the search process and article disposition. We initially identified 165 articles through database and supplementary searches, based on the pre-defined eligibility criteria. Publication dates ranged from 1981 to 2022, with 91% being published in or after 2000. Articles reporting on the same intervention were grouped together. Consequently, 122 distinct interventions reported in 165 articles were included in the review.
Descriptive characteristics of dyadic interventions
The characteristics of the included interventions and corresponding reports are summarised in the Supplement (for interventions with shared presence see S3, for interventions including an instructed interaction see S4). Moreover, a summary of characteristics across included interventions by category of partner involvement can be found in the Supplement (S2). The interventions were conducted across five different continents: America (n = 52), Europe (n = 18), Africa (n = 17), Asia (n = 17), Australia (n = 7), America/Africa (n = 1). However, n = 10 interventions did not provide any information on the location. The majority of interventions (n = 106, 87%) used a randomised controlled trial design, while the remaining n = 16 interventions (13%) used non-randomised designs. Across interventions, six different categories of health behaviour change were targeted. Specifically, 44 interventions targeted multiple health behaviours, while the remaining focused on substance use (smoking, alcohol; n = 27), sexual protective/risk behaviour (n = 22), physical activity (n = 19) and cancer screening (n = 6). Eating behaviours and medication adherence were addressed by two interventions each.
Couple definition and partner characteristics
The definition of couple varied substantially between interventions. Most commonly, self-report of being married (e.g., Hartmann et al., Citation2018) or being in a committed relationship (e.g., Newcomb et al., Citation2020) was used as the definition. Some studies specified additional criteria, such as defining the minimum relationship duration ranging from three months (e.g., Koniak-Griffin et al., Citation2008) to three years (e.g., O'Farrell & Murphy, Citation1995), or minimum cohabitation duration, varying from six months (e.g., Knoll et al., Citation2017) to 12 months (e.g., Robinson et al., Citation2007). Furthermore, some interventions required a prospect of a joint future (e.g., Speizer et al., Citation2018) or daily contact between the dyad members (i.e., Voils et al., Citation2020).
A great majority of interventions focused on mixed gender dyads (n = 84), while only two interventions specifically included same gender dyads (Martinez et al., Citation2018; Newcomb et al., Citation2020). The remaining interventions either included both mixed and same gender dyads (n = 15) or did not report the type of relationship (n = 21). Overall, about half of the interventions (n = 57, 47%) included dyads from the general population. In n = 47 interventions (38%), one partner of the dyad had a medical condition, and in n = 18 interventions (15%), both partners had medical conditions.
Dyadic intervention designs
A specific feature of dyadic interventions is that the person who receives the intervention (e.g., attends intervention sessions, receives intervention materials, or is instructed to do something) may not necessarily be the person who is designated to change their health behaviour. Across interventions, we identified several possible combinations of dyadic interventions designs. The intervention can be delivered to only one partner, with the focus of the health behaviour change being on both partners (i.e., the dyad) or the other partner. For example, in an intervention by Wakefield and Jones (Citation1998), pregnant smoking women received a smoking cessation intervention with the aim of helping both the women and their smoking partners to quit. On the other hand, also the other partner, who does not receive the intervention, can be the focus of a health behaviour change intervention. For example, Chan et al. (Citation2008) conducted an intervention in which non-smoking mothers of children with a disease received health information and were asked to share the information with their smoking spouses, thereby encouraging them to quit smoking.
Likewise, the intervention can be delivered to the dyad with either both partners (i.e., the dyad) being designated to change their health behaviour or only one of the partners. For example, Osuka et al. (Citation2017) conducted an intervention in which married couples attended exercise classes and were recommended to exercise together and keep track of each other's progress in order to improve long-term exercise adherence among people aged 65 years and older. Similarly, the intervention by Fals-Stewart et al. (Citation2006) was received by both members of the dyad, i.e., women with alcohol problems, attending individual and couples’ behavioural therapy sessions together with their non-substance-abusing male partners. However, only the female partner was designated to change the health behaviour with the male partner being an active participant to help female partners remain abstinent. Within each dyadic intervention design, the specific role of each partner and degree of partner involvement can be further specified.
Degree of partner involvement
Overall, interventions showed a great amount of variation in the nature and extent of the partner involvement, covering the entire continuum of dyadic interventions (i.e., mere presence, parallel, cross-over, joint). displays the frequency of interventions per prototype. The majority of interventions (n = 90, 74%) involved at least one form of instructed interaction between partners with about three quarters of them (n = 67) explicitly asking participants to do something jointly (i.e., joint), whereas in about one quarter (n = 23) one partner was asked to interact in some form with the other partner during intervention delivery or subsequent implementation (i.e., cross-over). For instance, in joint interventions, partners were asked to perform a joint target behaviour like engaging in short stretching exercises together (Cho et al., Citation2020), set a joint goal to reduce HIV risk behaviours (El-Bassel et al., Citation2010, Citation2011; NIMH, Citation2008), or jointly planned to engage in physical activity together (Wooldridge et al., Citation2019). In cross-over interventions for example, one partner was asked to provide support to the other partner following the intervention (e.g., Voils et al., Citation2009), to imagine the perspective and the experiences of the other partner who was not present (Akers et al., Citation2020), to serve as a model or cue for the target behaviour of the other partner in daily life (e.g., Gorin et al., Citation2020), or to share health information with the other partner in future interactions (e.g., Chan et al., Citation2008).
Figure 3. Frequency of interventions per prototype of dyadic interventions.
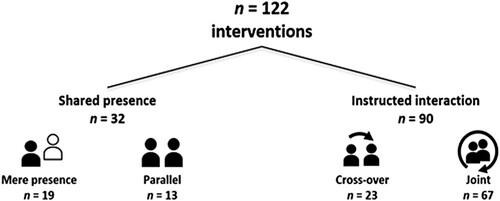
The remaining n = 32 interventions were categorised as shared presence (i.e., mere presence and parallel). In n = 13 interventions partners were asked to perform a parallel task not including an interaction between them (i.e., parallel). For example, in one study each partner set their individual activity goal at the same time (Gellert et al., Citation2011), while in another study, partners independently, but in parallel attended motivational feedback sessions (Woodin & O’Leary, Citation2010). In the other n = 19 interventions, the partner was merely present, not having an active role or interaction during the intervention procedure (i.e., mere presence). For instance, dyad members attended sessions on safe sexual behaviour (Delavande et al., Citation2016), pregnant women received tailored coaching on maternal health behaviours with their male partners being invited to attend (Oostingh et al., Citation2020; van Dijk et al., Citation2020), or data were assessed from both partners such as for example weight status and adherence to weight control behaviours from patients seeking bariatric surgery and their romantic partners (Ferriby et al., Citation2019). However, neither of these interventions explicitly described an active role of the partner or a specific interaction between partners in the intervention. As mentioned previously, interventions in which the partner was present, but it remained unclear if or how partners actively interacted with each other, for example receiving couple counseling (e.g., Becker et al., Citation2009) or participation in group activities (e.g., Dracup et al., Citation1984), were classified as mere presence.
Comparing characteristics of interventions with varying degree of partner involvement
An analysis of publication date revealed no temporal effect on the prototype of dyadic interventions. The publication date between interventions classified as instructed interaction (i.e., cross-over or joint) and shared presence (i.e., mere presence or parallel) did not significantly differ (p = .142). Therefore, there was no evidence of a change in the use of prototype of dyadic intervention over the years.
Health behaviours. Among interventions including instructed interaction between partners, the majority of interventions targeted one single health behaviour (71%), whereas most of the interventions with shared presence of partners targeted multiple health behaviours (i.e., more than one) at once (56%). Overall, there was a large overlap of the health behaviours targeted by the interventions across categories (i.e., instructed interaction and shared presence), except for cancer screening and healthy eating, which were exclusively represented in interventions with instructed interaction (see Supplement S2).
Comparing targeted health behaviours in interventions categorised as joint versus cross-over as well as parallel versus mere presence, indicated only few differences (see Supplement S2). For instance, cross-over interventions tended to target substance use more often (43%) compared to joint interventions (21%), though this difference was not statistically significant (p = .054). Moreover, more than one-third of interventions with mere presence – but no parallel intervention – focused on sexual protective/risk behaviour (37%; p = .025). Further, parallel interventions more often focused on substance use (23%) compared to mere presence interventions (of which none targeted substance use), though this also did not reach statistical significance (p = .058). Healthy eating behaviours were targeted only by cross-over interventions (9%, p = .063). Again, the differences remained on a descriptive level only.
Dyad characteristics. Dyad characteristics (e.g., mixed and same gender dyads) were similar between prototypes of dyadic interventions (see Supplement S2). A higher proportion of interventions with shared presence (34%) included dyads with both partners having a medical condition compared to interventions with instructed interaction (8%; p <.001). Further, a higher proportion of dyads with one partner having a medical condition were present in interventions with instructed interaction (50%) compared to interventions with shared presence (6%; p <.001). Overall, cross-over interventions (52%), parallel interventions (54%) and interventions with mere presence (63%) mainly included dyads without a medical condition.
Dyadic intervention techniques to change behaviour
To specifically understand how partners were involved, dyadic intervention techniques implemented in the 90 interventions classified as instructed interaction were extracted in detail. Within these interventions, we extracted 76 distinct intervention tasks (i.e., what is being performed?) that were implemented as 160 different dyadic intervention techniques (i.e., who performs what for whom) to change health behaviour. These techniques were applied 722 times across the interventions with instructed interaction (see ).
The extensive review of the extracted techniques served as the basis for the conceptual development of the definition of dyadic intervention techniques (DITs). We refer to dyadic intervention techniques as a composition of (1) the execution level of the intervention task within the dyad, (2) the intervention task itself, and (3) the target level of the intervention task (see for the conceptual overview). The compendium depicts a matrix of all identified dyadic intervention techniques nested in 30 identified theoretical determinants (i.e., theoretical predictors of behavioural change), which in turn are nested in 10 domains of the theoretical domains framework (e.g., skills or social influences; Atkins et al., Citation2017). The heat map of the compendium depicts the frequency of use, that is how often each dyadic intervention technique (i.e., who performs what for whom) was applied across all interventions. The frequency of use of each dyadic intervention technique varied between being implemented in only one single intervention to being implemented in 25 interventions. It has to be noted that intervention tasks are not always fully distinct. Thus, some instructions from intervention descriptions were assigned to more than one dyadic intervention technique. For example, in an intervention including couples with one partner being addicted to alcohol, the other partner was instructed to identify triggers for their partners’ alcohol consumption and to create plans including alternative behaviour (Flanagan et al., Citation2019; Worden et al., Citation2015). This exercise would reflect the intervention tasks one partner creates a coping plan for the other partner as well as one partner identifies barriers with identification of solutions (problem solving) for the other partner.
Of the 76 intervention tasks (i.e., what is being performed?), n = 23 intervention tasks were similar to behaviour change techniques from existing health behaviour change taxonomies (Kok et al., Citation2016; Michie et al., Citation2013). This includes for example planning, cue control, or goal setting. Overlap of intervention tasks with techniques from existing taxonomies are indicated by exponent digits following the label of the intervention task (see ). However, the majority of intervention tasks were unique to the dyadic setting and were not yet covered by previous taxonomies, such as sharing health information, practicing communication skills for health behaviour, or engaging in cooperative action.
Frequency of dyadic intervention techniques
We counted the frequency of use of each dyadic intervention technique (i.e., who performs what for whom), arriving at a total use of 722 times across the 90 interventions classified as instructed interaction. Specifically, dyadic intervention techniques were applied 242 times (34% of overall frequency of use) as cross-over techniques (i.e., performed by one partner) and 480 times (66%) as joint techniques (i.e., performed by the couple) (see ).
Cross-over techniques vs. joint techniques. Of the 722 total applications, about one-third (31%, n = 221) were cross-over techniques that targeted the other partner, i.e., one partner performed the intervention task for the other partner (e.g., one partner receives education for supporting the other partner or one partner demonstrates the health behaviour to the other partner). Cross-over techniques that targeted the couple were applied in 3% (n = 21) of all frequency counts, i.e., one partner performed the intervention task for the couple (e.g., one partner recognises relationship consequences from health behaviour of the couple or one partner monitors the couple). In contrast, half (50%, n = 360) of the total applications were joint techniques targeting the couple, i.e., the couple performed the intervention task for the couple (e.g., the couple adopts an attitude of being a team for the health behaviour change of the couple or the couple performs the health behaviour for the couple). In 17% (n = 120) of the overall frequency of use, dyadic intervention techniques were performed by the couple and targeted one partner, i.e., the couple performed the intervention task for one partner (e.g., the couple identifies and changes behaviour that serves as a trigger for one partner or the couple identifies effective support behaviours for one partner).
Couple-level vs. individual-level target. Overall, the majority of all applied dyadic intervention techniques had a couple-level target (53%, n = 381) compared to an individual-level target (47%, n = 341), for instance, the couple sets a goal for the couple (n = 16) versus for one partner (n = 5) or the couple plans for the couple (n = 17) versus for one partner (n= 9).
Most frequently employed dyadic intervention techniques. Altogether, the most frequently employed dyadic intervention techniques to change health behaviour were the couple practices communication skills for health behaviour of the couple (n = 25), the couple practices skills for health behaviour of the couple (n = 23), and the couple identifies barriers with identification of solutions (problem solving) for the couple (n = 20). In total, 52 dyadic intervention techniques were used each in one intervention only, such as the couple identifies behavioural substitution for the couple (n = 1) or one partner prompts self-monitoring of the other partner (n = 1).
Frequency of dyadic intervention techniques across TDF domains. Comparing frequencies of use of dyadic intervention techniques (i.e., how often dyadic intervention techniques were applied across all interventions) between the domains of the TDF (Atkins et al., Citation2017), we found that dyadic intervention techniques nested within the domain of social influences were used 198 times (27%), followed by dyadic intervention techniques nested in the domain of behavioural regulation that were applied 185 times (26%), and the domain of goals where dyadic intervention techniques were used 80 times (11%) across all interventions.
Dyadic intervention techniques for changing support behaviour. We further identified a set of dyadic intervention techniques that specifically aimed to change support behaviours as the most proximal behavioural outcome (see ). We identified several dyadic intervention techniques to change support behaviour that were unique in terms of their intervention content, such as one partner adopts a positive attitude to provide support to the other partner (n = 6) or one partner identifies effective support behaviours for the other partner (n = 9). Additionally, we also identified dyadic intervention techniques that target the regulation of support behaviour and that use similar intervention tasks, e.g., planning, goal setting, or monitoring, as those dyadic intervention techniques to change health behaviour. We clustered all those dyadic intervention techniques targeting behaviour-specific support whose intervention tasks overlap with dyadic intervention techniques to change health behaviour within the determinant support regulation.
Mutual execution of dyadic intervention techniques. A total of n = 39 dyadic intervention techniques of the compendium were executed mutually as indicated by an asterisk in the respective cells. For example, in an intervention by Winters-Stone et al. (Citation2012), romantic partners were supposed to coach each other while exercising, and thus, one partner was instructed to take on the role as coach for the other partner, before the other partner was then instructed to adopt the role as a coach for their partner.
Discussion
This systematic review aimed to provide an overview of the landscape of existing dyadic interventions with romantic couples and the dyadic intervention techniques used in these interventions to change health behaviour. We introduced a newly revised systematic framework for classifying dyadic interventions according to their degree of partner involvement (based on Scholz et al., Citation2020), and a novel compendium of dyadic intervention techniques (DITs) used in these interventions that describes the dyadic intervention techniques’ execution level, intervention task, and target level. The compendium of dyadic intervention techniques offers a first step for more systematic reporting and description of dyadic intervention content in all its complexity. The present review also provides a basis for the development of a theory-based and agreed-upon compendium that aims to facilitate the development and evaluation of dyadic interventions and dyadic intervention techniques (for further information on the project, please see: https://OSF.io/r43v6/). This will help to broaden our understanding of dyadic behaviour change.
This systematic review makes several conceptual contributions to the existing literature. Due to the lack of structural and conceptual clarity in the dyadic health behaviour change literature, we proposed a definition of dyadic interventions that includes any type of intervention that explicitly addresses both members of a dyad as part of the intervention procedure, with a range of techniques targeting either one (focus person or partner) or both partners to change at least one dyad member’s health behaviour. Accordingly, also interventions that solely apply individual behaviour change techniques but in which the other partner is at least present or performs a task in parallel (i.e., shared presence) are considered dyadic. Interventions including any type of instructed interaction with or reference to the other partner were focused on more closely in the present review (i.e., instructed interaction). To better describe what happens in such instructed interactions between dyad members, we further introduced a compendium of dyadic intervention techniques (DITs). This compendium accounts for the complexity of dyadic intervention techniques by defining and distinguishing in a systematic manner between important features of the involvement of the dyad member in the technique. That is, a dyadic intervention technique results from a combination of an execution level (i.e., who performs the intervention task?), an intervention task (i.e., what is being performed?), and a target level (i.e., whom is the intervention task targeted at?). The fine-grained differentiation of the execution and target levels when defining a dyadic intervention technique systematically describes partner involvement in each intervention task, and thus, has important implications for intervention development and the assessment of the effectiveness of dyadic intervention techniques.
Main results of the review
The results revealed that the majority of the reviewed interventions instructed an interaction between the dyad members using cross-over techniques or joint intervention techniques (74%), whereas in only 26% of the interventions the partner was merely present or received a parallel task without any explicit interaction between the partners. We observed no significant shift in the use of dyadic interventions over time, meaning that actively involving both partners has continuously been the preferred way to intervene in couple interventions to change health behaviour. We found a large overlap of targeted health behaviours between interventions with instructed interaction and interventions with shared presence. Prototypes of dyadic interventions did not differ in terms of their targeted health behaviours. Nevertheless, it can be assumed that the level of interdependence in the target behaviour of romantic partners could influence the choice of an intervention. For example, it stands to reason that couples would set joint goals and jointly plan for their sexual protection behaviours, such as condom use. In contrast, in interventions targeting medication adherence of one partner, the other partner’s presence at an education session might be sufficient.
The dyadic intervention techniques targeted determinants across nearly all domains of the theoretical domains framework (Atkins et al., Citation2017). This is in line with prior findings indicating the importance of dyadic interaction throughout various stages of behaviour change (Rhodes et al., Citation2002). In total, 76 different intervention tasks (i.e., what is being performed?), and 160 different dyadic intervention techniques (i.e., who performs what for whom?) to change health behaviour were extracted from the included studies, indicating an abundance of possibilities to promote health behaviour change in dyads. Notably, a majority of these dyadic intervention techniques were performed by the couple (i.e., joint techniques), whereas fewer were performed by one partner alone (i.e., cross-over techniques). Most joint techniques targeted the couple, whereas only a few joint techniques targeted one partner. For instance, more interventions instructed the partners to create couple-level plans, set couple-level goals, or to recognise the couple-level risk of a health behaviour, instead of jointly planning, setting goals, or recognising health risks for only one partner. This is in line with theoretical propositions suggesting that increased partner involvement in behaviour change holds more potential for successful behaviour change (Fitzsimons et al., Citation2015; Lewis et al., Citation2006). Cross-over techniques primarily targeted the other partner, including tasks such as receiving education about support, providing instrumental, informational, emotional, or unspecified support or taking on the role as a coach for the other partner. It is conceivable that many of these intervention tasks would have been subsumed under ‘support provision’, when using existing taxonomies to code individual intervention techniques (Bartholomew et al., Citation2006; Kok et al., Citation2016; Michie et al., Citation2013). The great variety of intervention tasks of the present compendium that instructed on how to encourage, how to support, or how to understand the partner, empathises the importance of a more fine-grained way to describe dyadic intervention content as will be facilitated by the compendium.
The most commonly used dyadic intervention techniques instructed the couples to practice communication skills, to practice (other) skills, or to engage in problem solving for the health behaviour of the couple. The great focus on improving couple-level skills might be attributed to the fact that the joint execution of skills requires more complex behavioural scripts than the individual execution of skills in order to be effective (van der Wel et al., Citation2021). For example, joint problem solving necessitates discussion and coordination to reach a satisfactory agreement on the type of problem and its solution, whereas individual problem solving usually does not require such interpersonal arrangements (van der Wel et al., Citation2021). Assuming that romantic partners communicate and coordinate well, couple-level skills can unlock additional resources (Rusbult & Van Lange, Citation2003). For instance, jointly solving a problem, as opposed to individual problem solving, might aid the identification of barriers and solutions through good communication and mutual cooperation, partners might be able to expand on each other’s ideas and perspectives, anticipate additional needs or difficulties, and identify synergies regarding interests and skills more easily. Jointly arranging an active vacation, for example, might lead to the agreement to do a multi-day bike tour for which one partner selects the route and commits to navigate throughout the tour, while the other partner agrees to take care of bike tools and maintenance of the bikes throughout the tour. In addition, a positively experienced conversation about the bike tour has the potential to strengthen the emotional bond between partners, increasing their commitment to the tour and the coordinated action required to make the bike tour possible. The relatively high number of interventions that instructed couples to practice their communication about health behaviour and support behaviours, seems promising in light of prior findings highlighting the importance of couple communication for successful behaviour change (Dailey et al., Citation2011). In a similar vein, many intervention tasks aimed at improving the quality of support attempts, such as receiving education for supporting, adopting a positive attitude to provide support, or identifying support needs. Prior studies have shown that social support should be tailored to recipients’ needs to be positively associated with health (Lee et al., Citation2019; Selcuk & Ong, Citation2013; Thong et al., Citation2006). Thus, the reviewed dyadic interventions that aim to directly improve support behaviour seem particularly promising.
Importantly, as the compendium at this point only includes dyadic intervention techniques extracted from the literature, it needs to be highlighted that there may be additional dyadic techniques that are not yet included. Therefore, the compendium cannot be interpreted as an exhaustive list of all possible dyadic intervention techniques. Similar to the evolution of the BCT taxonomy (Michie et al., Citation2013) into a behaviour change intervention ontology (BCIO, Marques et al., Citation2023), the present compendium serves as a starting point for the development of an agreed-upon and theory-based compendium of dyadic intervention techniques.
Contributions of the review
This review significantly contributes to the systematic description of dyadic interventions. The newly revised continuum of dyadic interventions developed by Scholz et al. (Citation2020) allows for a systematic classification into different prototypes of dyadic interventions based on the degree to which the partner is involved. This is particularly important because the different prototypes of dyadic interventions might trigger different processes (i.e., mechanisms of action, Moore & Evans, Citation2017) linked to behaviour change (Scholz et al., Citation2020). Prior evidence suggests that individual performance (e.g., as response to an intervention task) is interdependent with the social context (Gully et al., Citation2002). For example, close partners are assumed to share memory resources (Wegner et al., Citation1991) or to automatically expand their self-concept by the resources of others, leaving more capacity for the individual to acquire new skills or qualities (Aron & Aron, Citation1986). Accordingly, the social baseline theory (Beckes & Coan, Citation2011) posits that individuals, when with others, automatically adjust their expectations about the availability of their own personal resources by including those resources expected to be available from the social setting. This might hold individuals in a state of relative calm with lower need for emotion regulation or self-regulation when facing situational challenges when with others as opposed to being alone (Beckes & Coan, Citation2011). The beneficial effect of social proximity increases with greater familiarity or interdependence of the social environment so that the presence of a romantic partner is assumed to be particularly beneficial for self-regulation processes (Beckes & Coan, Citation2011). Thus, dyadic interventions with shared presence might foster important mechanisms of action in focus persons (e.g., memories, self-efficacy, attention, helpful cognitions, and emotions) simply by physical proximity, and in partners (e.g., knowledge, attitudes, self-efficacy) by observing the intervention or performing a task in parallel. Interventions with an instructed interaction that use dyadic intervention techniques, either by targeting one partner (i.e., cross-over techniques) or by targeting both partners jointly (i.e., joint techniques) are likely to trigger additional processes of social exchange, such as supportive interactions (Burkert et al., Citation2011) or relational mechanisms such as communal coping (Lewis et al., Citation2006). Interdependence theory posits that any kind of joint engagement for a health outcome of one partner or the couple increases coordination between dyad members and activates ability-related traits and behaviours, such as problem-solving or improved action taking (Rusbult & Van Lange, Citation2003).
More theoretical work is needed to generate hypotheses about the dyadic mechanisms triggered by different prototypes of dyadic interventions. Moreover, subsequent empirical work needs to test these assumptions. The specific dyadic mechanisms of action (Connell et al., Citation2019) triggered by interventions with instructed interaction may also depend on the specific dyadic intervention techniques used (see more detailed discussion of this below).
Furthermore, the review makes an important contribution to systematically label and characterise dyadic intervention techniques used in interventions that include an instructed interaction. The proposed compendium accounts for the complexity of these techniques by defining and distinguishing important features such as execution level, intervention task, and target level. This can assist future researchers in describing and identifying instructed interactions in detail, which can provide valuable insights into moderator effects, such as who executes an intervention task or whom the intervention task is targeted at. The IM taxonomy (Kok et al., Citation2016) acknowledges the importance of the social environment for behaviour change by conceptualising environmental agents (e.g., couples, romantic partners) as potential recipients of intervention tasks for the behaviour change of a focus person. However, in the IM taxonomy, environmental agents do not only refer to individuals at the interpersonal level (e.g., teachers, partners, parents), but also to stakeholders at an organisational, community, or societal level. This way, authors of the IM taxonomy describe rather broad social influences that are predicted to change environmental conditions (Kok et al., Citation2016). The present compendium, in contrast, focuses on instructed interaction at an interpersonal level with the goal to facilitate at least one person’s health behaviour. In part, the present compendium builds upon existing taxonomies (e.g., BCT taxonomy; Michie et al., Citation2013; IM taxonomy, Kok et al., Citation2016) by zooming in on previously described behaviour change techniques that involve an instructed interaction with another (non-professional) person. To ensure comparability to individual intervention techniques we adapted existing labels wherever possible. The majority of intervention tasks were not covered by previous taxonomies (e.g., shares health information with the partner, practices communication skills for health behaviour, or engages in cooperative action). A total of 23 out of the 76 intervention tasks (i.e., what is being performed?) extracted in the present review closely resembled behaviour change techniques in individual health behaviour change taxonomies (Kok et al., Citation2016; Michie et al., Citation2013). For instance, planning, controlling cues, or setting goals. In these cases, the intervention task itself was comparable to existing BCTs, but they were adapted significantly for dyadic use (e.g., instead of planning for oneself, the couple plans together for one person or the couple plans together for themselves). The explicit involvement of another individual in an intervention task yields an important qualitative difference compared to a traditional individual behaviour change technique. We propose that the involvement of a partner in an intervention task (i.e., either at the execution or target level) creates a different experience from executing an intervention task alone (or with a professional interventionist), and thus will foster different mechanisms of action. Unlike a simple mode of delivery, which defines how the intervention content (i.e., intervention task) is delivered (Marques et al., Citation2021), a dyadic intervention technique defines what content is brought to participants. For example, a goal-setting task can be delivered in written or oral form, which is the mode of delivery. The content of an intervention task (i.e., what the participants perform to accomplish the goal-setting task) does not change depending on the mode of delivery. If two versus one person are instructed to set a goal together, this directly influences what participants do during the goal-setting task, e.g., discuss, consult or potentially monitor each other’s actions. Dyadic intervention techniques therefore extend individual intervention techniques as they are assumed to instigate natural processes in everyday life that primarily evolve from the instructed interaction with a close other. However, the specific processes that are triggered by dyadic intervention techniques are still not well understood.
Moreover, the compendium of dyadic intervention techniques will facilitate the identification of mechanisms of action (MoA; Connell et al., Citation2019), which are the psychological, physical, or social processes, that can influence, maintain, or catalyse a change in behaviour (Carey et al., Citation2018; Connell et al., Citation2019; Moore & Evans, Citation2017). Both individual and dyadic intervention techniques are assumed to modify or stimulate mechanisms of action for behaviour change. Understanding the link between dyadic intervention techniques and mechanisms of action is crucial to understand dyadic behaviour change and to facilitate the development of effective intervention designs. Strongly theory-driven, the IM taxonomy was the first taxonomy to provide theory-based assumptions about the link of behaviour change techniques with psychological variables and regulatory processes preceding behaviour change (Kok et al., Citation2016). Recently, there has been considerable effort to identify BCT-MoA links to understand individual behaviour change (Carey et al., Citation2018; Connell et al., Citation2019; Michie et al., Citation2018; Schenk et al., Citation2023). Literature review and expert consensus showed that even at the level of individual behaviour change there is great diversity in how specific BCTs influence certain MoAs (Carey et al., Citation2018; Connell et al., Citation2019). As shown in the present review, introducing a partner in the process of behaviour change increases the complexity of intervention techniques themselves and thus likely also increases the diversity of potential MoAs for behaviour change. As dyadic intervention techniques involve two people (e.g., the couple plans for the couple), MoAs might act through intrapersonal mechanisms at the individual level (e.g., individual planning) and/or through interpersonal mechanisms at the couple-level (e.g., collaborative social control; Kulis et al., Citation2022), both of which can facilitate behaviour change (see also Lewis et al., Citation2006). The proposed framework of dyadic intervention techniques, specifying who performs which intervention task for whom, will serve as an important basis to identify different sets of dyadic intervention techniques (e.g., techniques with a joint execution or joint target level) that uniquely stimulate certain MoAs.
According to the transactive goal dynamics theory (Fitzsimons et al., Citation2015), the pool of couple-level resources (e.g., skills, mental and physical capacities, energy, or time) increases with greater interdependence of goals (e.g., being physically active together), pursuits (e.g., blocking time for each other, monitoring progress of each other), and outcomes (e.g., joint weight loss) between romantic partners (Fitzsimons et al., Citation2015). The theory suggests that having similar goals for the other partner or for them as a couple (i.e., shared goal representation), understanding and recognising needs and resources of the partner (i.e., responsiveness), as well as the efficient coordination of efforts facilitating behaviour change, predicts the extent to which dyad members unlock couple-level resources and show improved behaviour change (Fitzsimons et al., Citation2015). Dyadic intervention techniques might influence both, the extent to which behaviour change efforts between partners are intertwined as well as important factors facilitating the efficient use of the pooled resources. For instance, dyadic intervention techniques, where dyad members set goals, plan, or solve a problem together, should improve shared goal representation as partners agree on goals and means of how to pursue them. Dyadic intervention techniques, such as sharing thoughts and feelings towards health behaviour, identification of support needs, or practice of communication skills about support behaviour might improve partner responsiveness to recipients’ needs in behaviour change efforts and therefore improve coordination and also relationship satisfaction. Other dyadic intervention techniques make the use of pooled resources even more visible. For instance, instructing the couple or one partner to set an external cue, prompt self-monitoring, demonstrate health behaviour or to take on the role as a coach for the other partner. Further considerations on the link between dyadic intervention techniques, mechanisms of action (MoAs), and successful behaviour change can be informed by hypotheses from communal coping theory (Lewis et al., Citation2006). This theory suggests that motivation to cope with a problem together and to engage in cooperative action is higher if dyad members perceive a problem as shared, rather than individual (Lewis et al., Citation2006; Lyons et al., Citation1998). Thus, intervention tasks such as adopts an attitude of being a team for the health behaviour change of one partner or the couple, as well as engages in cooperative action for the health behaviour of one or both partners should increase the intention of dyad members for communal coping and facilitate cooperative action.
So far, no comprehensive model or framework of dyadic behaviour change exists that addresses different MoAs underlying dyadic behaviour change. However, using the structure of the theoretical domains framework (Atkins et al., Citation2017; Cane et al., Citation2012) allows for the categorisation of related theoretical constructs in a meaningful way. This can be used as a first step for more elaborated empirical research on the underlying processes and MoAs through which dyadic intervention techniques stimulate behaviour change.
Effectiveness of dyadic intervention techniques
Creating a systematic reporting and shared language of dyadic intervention techniques will facilitate data syntheses for testing the effectiveness of dyadic interventions. It needs to be acknowledged that the explicit bottom-up approach, as done in the present review, does not allow conclusions about the significance or effectiveness of single dyadic intervention techniques, yet. However, providing a systematic approach for describing dyadic interventions, including dyadic intervention techniques used, is a first important step to shed more light on the heterogeneity of couple interventions and their effectiveness. Preliminary evidence suggests that different constellations of the target levels (i.e., whether an intervention task targets the couple or one partner) of the same intervention task (i.e., planning) are not equally effective. Kulis et al. (Citation2022a) demonstrated improved physical activity when dyad members (including, but not limited to romantic couples) jointly planned for one partner (i.e., ‘we for me’) compared to a control condition. However, this was not the case for dyad members who jointly planned for the dyad (i.e., ‘we for us’, collaborative planning; Kulis et al., Citation2022a). Which components of dyadic intervention techniques (i.e., who performs what for whom?) will uncover meaningful differences empirically needs to be examined by future research.
The precise description of dyadic intervention techniques will also enable the identification of optimal matches between dyadic intervention techniques and dyad characteristics. For example, intervention tasks performed by the couple (i.e., joint execution level) and targeted at only one partner (i.e., individual target level) may be more effective in case one partner is in greater need to change their health behaviour, such as due to a medical condition. In contrast, when behaviour change is equally desirable for both partners, joint techniques targeting only one partner might even diminish intervention effectiveness in some circumstances. For example, a study by Keller et al. (Citation2020) showed that randomly assigned target persons from couples of a dyadic planning condition (instructed to plan together only for the randomly assigned target person) to increase physical activity had – particularly in case of low relationship quality – the least favourable effects on physical activity compared to target persons from an individual planning condition and a no-planning control group. The authors concluded that randomly determining the target person of the intervention undermined dyadic processes and created inequity within the dyad that might have been counter-productive (Keller et al., Citation2020). For such intervention designs, a mutual form of dyadic planning may be more promising, where partners first plan together for one, and then for the other partner. Our compendium should encourage researchers to specifically pay attention to the fit between dyadic intervention techniques and dyad characteristics and the possible dynamics that may result.
The findings of the present review emphasise the need for more differentiated analyses when examining effectiveness of dyadic interventions. Meta-analyses could account for the heterogeneity of couple interventions by differentiating effects for the prototypes of dyadic interventions, different health behaviour domains, specific combinations of execution and target level (e.g., cross-over techniques versus joint techniques), or specific dyadic intervention techniques. The synthesis of evidence for the prototypes of dyadic interventions as well as combinations of execution and target level can thus be guided by the conceptualisations of the present review. However, it is important to note that the compendium does not represent a coding taxonomy like the BCT taxonomy (Michie et al., Citation2013). It does not guarantee distinctiveness of the different intervention tasks (e.g., identification of effective support behaviour, provide emotional support, etc.). Therefore, evidence synthesis for single intervention tasks based on the compendium should be conducted with caution, considering potential overlaps.
Boundary conditions of dyadic intervention techniques to change health behaviour
With the detailed description of different features of dyadic interventions that we extracted in this review, we can begin to establish theoretical assumptions and empirical findings in terms of when and for whom certain types of dyadic interventions or dyadic intervention techniques might be particularly effective, ineffective, or even potentially harmful (i.e., boundary conditions).
The choice of the appropriate dyadic intervention type and dyadic intervention technique should depend on the structural context, which includes aspects such as the targeted health behaviour, the target of the intervention (one partner vs. the couple), the characteristics of the setting, as well as the unique characteristics of the partners (e.g., health status, role within the relationship, attachment style) and/or dyad characteristics (e.g., type of relationship, relationship dynamics, relationship satisfaction). For instance, some health behaviours are inherently dyadic in nature (e.g., safer sex), where both members of the dyad share equal responsibility and accountability for execution. In such cases, dyadic intervention techniques that equally focus on both partners (i.e., joint techniques targeting the couple) are likely to be more effective. Conversely, there are health behaviours that are more individual in nature but can also be performed together (e.g., cancer screening). For these ‘more individual’ behaviours, such as flossing, it may be more reasonable to focus on one partner as the assisting figure.
Dyadic interventions using cross-over techniques (i.e., one partner performs an intervention task that targets the other partner or the couple) might be better suited for interventions where, for example, only one partner is available for the intervention. This might be due to a lack of willingness on the part of one partner to participate in an intervention or pre-existing role allocation between partners, e.g., patient/target partner-care/support partner (Pitkälä et al., Citation2013). Cross-over techniques in dyadic interventions that allow partners to self-select their roles (i.e., focus person or partner) may also involve less conflict for couples with pre-existing asymmetries, which should remain untouched by the dyadic intervention technique (Rusbult & Van Lange, Citation2003). However, dyadic interventions using joint techniques that target the couple are more likely to ensure equal attention to both partners’ needs and perspectives and therefore might improve intervention fidelity and effectiveness (Richards et al., Citation2017).
It also needs to be highlighted that dyadic interventions might not be suitable for every couple. Whether an interaction between the partners, instructed by the interventionist, is perceived or enacted as positive and helpful, strongly depends on relationship- and couple characteristics, such as communication patterns, relationship satisfaction, equity, expertise, power dynamics, or attachment types and individual characteristics (e.g., preference for self-reliance) (Huelsnitz et al., Citation2022). While a substantial body of evidence supports the positive link between social relationships and health (Holt-Lunstad, Citation2021; Holt-Lunstad et al., Citation2015), it is important to recognise that not every relationship is inevitably positive. In fact, negative social interactions or being in an unhappy relationship might have a negative impact on health outcomes (Robles & Kiecolt-Glaser, Citation2003; Yang et al., Citation2016), and the behaviour of close others can also sabotage the efforts to change behaviour (e.g., Stanforth & Mackert, Citation2009). Whether the use of social control strategies has a favourable effect on health behaviour change, for example, was shown to depend on the types of control strategies (Young et al., Citation2019), and relationship satisfaction of the couple (Siwa et al., Citation2023). Particularly, negative social control strategies (e.g., pressure) as opposed to positive social control strategies (e.g., persuasion) may have a negative impact on relationship (Siwa et al., Citation2023) and health outcomes (Craddock et al., Citation2015), and therefore should be used with caution in dyadic interventions. Further, research indicates that the effects of social control can vary based on relationship quality, such as in the context of cigarette smoking (e.g., Scholz et al., Citation2013). Accordingly, Martire et al. (Citation2010) argued that couples with higher marital satisfaction might still perceive positive aspects, such as good intentions, in unhelpful support attempts, whereas unhelpful support attempts might yield only negative effects in couples with lower marital satisfaction (Martire et al., Citation2010). Consequently, dyadic interventions aimed at increasing the interaction and interdependence of partners regarding health behaviour change, may not be suitable for every couple. Aspects of the structural context, especially the targeted health behaviour as well as partner and dyad characteristics, should be considered when deciding on the type of dyadic interventions and dyadic intervention techniques.
Implications for future research
The continuum of dyadic interventions () and the compendium of dyadic intervention techniques (), in all their complexity, presents a first step towards a systematic description of dyadic interventions and dyadic intervention techniques. By clustering identified dyadic intervention techniques within the theoretical domains framework (Atkins et al., Citation2017), the proposed compendium of dyadic intervention techniques provides first insights in the targeted determinants potentially driving dyadic behaviour change. These determinants should be tested as mediating pathways of dyadic intervention effects in future research. Additionally, potential moderating effects should be tested in effectiveness analyses, considering different types of dyadic interventions and their boundary conditions, different dyad characteristics, as well as different combinations of execution and target level across intervention tasks (e.g., joint techniques versus cross-over techniques). Providing links to theory is important to further enhance the understanding of underlying mechanisms of action of dyadic behaviour change. Therefore, as an important next step, we will integrate and link identified dyadic intervention techniques to theoretical concepts. Subsequently, we will conduct an expert consensus to validate the identified and described dyadic intervention techniques, aiming to achieve an agreed-upon compendium of theoretically-derived, clearly labelled, and defined dyadic intervention techniques (for further information on the project see: https://OSF.io/r43v6/).
Limitations
In addition to the above-outlined strengths of the current review, limitations need to be recognised.
First, the results of the present review and the compendium of extracted dyadic intervention techniques are limited to published studies in English, and eligible studies in other languages might have been omitted. However, several measures were taken to reduce this risk, such as searching in multiple databases, conducting backward searches, searching for connected studies, and contacting authors of included studies for additional research.
Second, the classification of the degree of partner involvement and the extracted dyadic behaviour change techniques are limited to the available information in intervention descriptions. This bears the risk of miss-classifying interventions or missing additional dyadic intervention techniques. To address this potential bias and prevent missing data, authors of included interventions were contacted to request more detailed descriptions of the intervention and additional material, including intervention or training manuals. When available, study protocols, connected papers, and additional material sent by the first authors of reviewed studies were included in the extraction process. However, for eight interventions we could only affirm the mere presence of the partner since the intervention description lacked further details.
Third, it is important to acknowledge that the present compendium of dyadic intervention techniques is limited to health behaviour change interventions in romantic couples. Nevertheless, the compendium lays a foundation for other more extended versions of dyadic intervention techniques across different dyad constellations (e.g., parent–child dyads) and behavioural contexts (e.g., mental health, stress).
Fourth, the present compendium is highly complex, with various combinations of execution and target levels for each intervention task. This complexity requires a thorough understanding of the compendium’s structure and may pose challenges to its practical application. In the field of dyadic behaviour change, we are generally confronted with a high degree of complexity. The Health Influence Model, for example, identifies numerous possible pathways between health behaviours and beliefs, relational behaviours and beliefs, and influence strategies through which partners can influence each other's health behaviours (Huelsnitz et al., Citation2022). The compendium aims to alleviate some of this complexity by systematically describing all possible couple combinations within each intervention task in a unified matrix. Moreover, the allocation of dyadic intervention techniques to both the domains of the TDF (Atkins et al., Citation2017; Cane et al., Citation2012) and theoretical determinants should facilitate the reporting of and theory-guided selection from the numerous dyadic intervention techniques. Furthermore, at this early stage of development, the structure of the compendium enables the identification of potentially important features of dyadic intervention techniques, particularly by specifying ‘who performs what for whom?’. This specification may have significant empirical relevance in the future.
Conclusion
In conclusion, the compendium of dyadic intervention techniques extends the individual perspective of behaviour change to a dyadic perspective, specifically indicating how partners can be involved in health behaviour change interventions. It lays a foundation for the systematic description of dyadic interventions and implemented dyadic intervention techniques by specifying who is performing (i.e., execution level) an intervention task and whom the intervention task is targeted at (i.e., target level). The next steps consist of further refinement and integration of theory to provide a comprehensive compendium of dyadic intervention techniques to change behaviour, guiding not only standardised reporting, but also evidence synthesis and intervention development.
Availability of data
For specific requests please contact the corresponding author.
Supplemental Material
Download PDF (2.8 MB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Akers, L., Andrews, J. A., Lichtenstein, E., Severson, H. H., & Gordon, J. S. (2020). Effect of a responsiveness-based support intervention on smokeless tobacco cessation: The UCare-ChewFree randomized clinical trial. Nicotine & Tobacco Research, 22(3), 381–389. https://doi.org/10.1093/ntr/ntz074
- Arden-Close, E., & McGrath, N. (2017). Health behaviour change interventions for couples: A systematic review. British Journal of Health Psychology, 22(2), 215–237. https://doi.org/10.1111/bjhp.12227
- Aron, A., & Aron, E. N. (1986). Love and the expansion of self: Understanding attraction and satisfaction. Hemisphere Publishing Corp/Harper & Row Publishers.
- Atkins, L., Francis, J., Islam, R., O’Connor, D., Patey, A., Ivers, N., Foy, R., Duncan, E. M., Colquhoun, H., Grimshaw, J. M., Lawton, R., & Michie, S. (2017). A guide to using the Theoretical Domains Framework of behaviour change to investigate implementation problems. Implementation Science, 12(1), 1–18. https://doi.org/10.1186/s13012-016-0533-0
- Bartholomew, L. K., Parcel, G. S., Kok, G., Gottlieb, N. H., Schaalma, H. C., Markham, C. C., & Partida, S. C. (2006). Planning health promotion programs: An intervention mapping approach. Jossey-Bass.
- Baucom, D. H., Porter, L. S., Kirby, J. S., & Hudepohl, J. (2012). Couple-based interventions for medical problems. Behavior Therapy, 43(1), 61–76. https://doi.org/10.1016/j.beth.2011.01.008
- Baucom, D. H., Shoham, V., Mueser, K. T., Daiuto, A. D., & Stickle, T. R. (1998). Empirically supported couple and family interventions for marital distress and adult mental health problems. Journal of Consulting and Clinical Psychology, 66(1), 53. https://doi.org/10.1037/0022-006X.66.1.53
- Becker, S., Mlay, R., Schwandt, H. M., & Lyamuya, E. (2010). Comparing couples’ and individual voluntary counseling and testing for HIV at antenatal clinics in Tanzania: A randomized trial. AIDS and Behavior, 14(3), 558–566. https://doi.org/10.1007/s10461-009-9607-1
- Beckes, L., & Coan, J. A. (2011). Social baseline theory: The role of social proximity in emotion and economy of action. Social and Personality Psychology Compass, 5(12), 976–988. https://doi.org/10.1111/j.1751-9004.2011.00400.x
- Berli, C., Stadler, G., Inauen, J., & Scholz, U. (2016). Action control in dyads: A randomized controlled trial to promote physical activity in everyday life. Social Science & Medicine, 163, 89–97. https://doi.org/10.1016/j.socscimed.2016.07.003
- Brandão, T., Schulz, M. S., & Matos, P. M. (2014). Psychological intervention with couples coping with breast cancer: A systematic review. Psychology & Health, 29(5), 491–516. https://doi.org/10.1080/08870446.2013.859257
- Buck, H. G., Stromberg, A., Chung, M. L., Donovan, K. A., Harkness, K., Howard, A. M., Kato, N., Polo, R., & Evangelista, L. S. (2018). A systematic review of heart failure dyadic self-care interventions focusing on intervention components, contexts, and outcomes. International Journal of Nursing Studies, 77, 232–242. https://doi.org/10.1016/j.ijnurstu.2017.10.007
- Burkert, S., Scholz, U., Gralla, O., Roigas, J., & Knoll, N. (2011). Dyadic planning of health behavior change after prostatectomy: A randomized-controlled planning intervention. Social Science & Medicine, 73(5), 783–792. https://doi.org/10.1016/j.socscimed.2011.06.016
- Burton, J., Darbes, L. A., & Operario, D. (2010). Couples-focused behavioral interventions for prevention of HIV: Systematic review of the state of evidence. AIDS and Behavior, 14(1), 1–10. https://doi.org/10.1007/s10461-008-9471-4
- Byrt, T., Bishop, J., & Carlin, J. B. (1993). Bias, prevalence and kappa. Journal of Clinical Epidemiology, 46(5), 423–429. https://doi.org/10.1016/0895-4356(93)90018-V
- Cane, J., O’Connor, D., & Michie, S. (2012). Validation of the theoretical domains framework for use in behaviour change and implementation research. Implementation Science, 7(1), 1–17. https://doi.org/10.1186/1748-5908-7-37
- Carey, R. N., Connell, L. E., Johnston, M., Rothman, A. J., De Bruin, M., Kelly, M. P., & Michie, S. (2018). Behavior change techniques and their mechanisms of action: A synthesis of links described in published intervention literature. Annals of Behavioral Medicine, 53(8), 693–707. https://doi.org/10.1093/abm/kay078
- Carr, R. M., Prestwich, A., Kwasnicka, D., Thøgersen-Ntoumani, C., Gucciardi, D. F., Quested, E., & Ntoumanis, N. (2019). Dyadic interventions to promote physical activity and reduce sedentary behaviour: Systematic review and meta-analysis. Health Psychology Review, 13(1), 91–109. https://doi.org/10.1080/17437199.2018.1532312
- Chan, S. S., Leung, G. M., Wong, D. C., & Lam, T. H. (2008). Helping Chinese fathers quit smoking through educating their nonsmoking spouses: A randomized controlled trial. American Journal of Health Promotion, 23(1), 31–34. https://doi.org/10.4278/ajhp.07043040
- Cho, D., Basen-Engquist, K., Acquati, C., Ma, H., Pettaway, C., Li, Y., Diep, C. S., & McNeill, L. H. (2020). Study protocol: A lifestyle intervention for African American and Hispanic prostate cancer survivors on active surveillance and their partners. Pilot and Feasibility Studies, 6(1), 1–10. https://doi.org/10.1186/s40814-019-0545-z
- Connell, L. E., Carey, R. N., De Bruin, M., Rothman, A. J., Johnston, M., Kelly, M. P., & Michie, S. (2019). Links between behavior change techniques and mechanisms of action: An expert consensus study. Annals of Behavioral Medicine, 53(8), 708–720. https://doi.org/10.1093/abm/kay082
- Craddock, E., vanDellen, M. R., Novak, S. A., & Ranby, K. W. (2015). Influence in relationships: A meta-analysis on health-related social control. Basic and Applied Social Psychology, 37(2), 118–130. https://doi.org/10.1080/01973533.2015.1011271
- Dailey, R. M., Romo, L. K., & Thompson, C. M. (2011). Confirmation in couples’ communication about weight management: An analysis of how both partners contribute to individuals’ health behaviors and conversational outcomes. Human Communication Research, 37(4), 553–582. https://doi.org/10.1111/j.1468-2958.2011.01414.x
- Delavande, A., Wagner, Z., & Sood, N. (2016). The impact of repeat HIV testing on risky sexual behavior: Evidence from a randomized controlled trial in Malawi. Journal of AIDS & Clinical Research, 07(3), e1000549. https://doi.org/10.4172/2155-6113.1000549
- Dracup, K., Meleis, A. I., Clark, S., Clyburn, A., Shields, L., & Staley, M. (1984). Group counseling in cardiac rehabilitation: Effect on patient compliance. Patient Education and Counseling, 6(4), 169–177. https://doi.org/10.1016/0738-3991(84)90053-3
- El-Bassel, N., Jemmott, J. B., Landis, J. R., Pequegnat, W., Wingood, G. M., Wyatt, G. E., Bellamy, S. L., & National Institute of Mental Health Multisite HIV/STD Prevention Trial for African-American Couples Group (2011). Intervention to influence behaviors linked to risk of chronic diseases: A multisite randomized controlled trial with African-American HIV-serodiscordant heterosexual couples. Archives of Internal Medicine, 171(8), 728–736. https://doi.org/10.1001/archinternmed.2011.136
- El-Bassel, N., Jemmott, J. B., Landis, J. R., Pequegnat, W., Wingood, G. M., Wyatt, G. E., Bellamy, S. L., & NIMH Multisite HIV/STD Prevention Trial for African American Couples Group (2010). National Institute of Mental Health multisite Eban HIV/STD prevention intervention for African American HIV serodiscordant couples: A cluster randomized trial. Archives of Internal Medicine, 170(17), 1594–1601. https://doi.org/10.1001/archinternmed.2010.261
- Fals-Stewart, W., Birchler, G. R., & Kelley, M. L. (2006). Learning sobriety together: A randomized clinical trial examining behavioral couples therapy with alcoholic female patients. Journal of Consulting and Clinical Psychology, 74(3), 579. https://doi.org/10.1037/0022-006X.74.3.579
- Faseru, B., Richter, K. P., Scheuermann, T. S., & Park, E. W. (2018). Enhancing partner support to improve smoking cessation. Cochrane Database of Systematic Reviews, 2018(8), 1–42. https://doi.org/10.1002/14651858.CD002928.pub4
- Ferriby, M., Pratt, K., Wallace, L., Focht, B. C., Noria, S., & Needleman, B. (2019). Rationale and design of a feasibility and acceptability RCT of romantic partner and support figure attendance during bariatric surgery visits. Contemporary Clinical Trials Communications, 15, 1–9. https://doi.org/10.1016/j.conctc.2019.100422
- Fitzsimons, G. M., Finkel, E. J., & vanDellen. (2015). Transactive goal dynamics. Psychological Review, 122(4), 648–673. https://doi.org/10.1037/a0039654
- Flanagan, J. C., Joseph, J. E., Nietert, P. J., Back, S. E., & McCrady, B. S. (2019). Design of a randomized controlled trial examining the efficacy of oxytocin to enhance alcohol behavioral couple therapy. Contemporary clinical trials, 82, 1–8. https://doi.org/10.1016/j.cct.2019.05.002
- Gellert, P., Ziegelmann, J. P., Warner, L. M., & Schwarzer, R. (2011). Physical activity intervention in older adults: Does a participating partner make a difference? European Journal of Ageing, 8(3), 211–219. https://doi.org/10.1007/s10433-011-0193-5
- Gorin, A. A., Powers, T. A., Gettens, K., Cornelius, T., Koestner, R., Mobley, A. R., Pescatello, L. S., & Huedo-Medina, T. B. (2020). A randomized controlled trial of a theory-based weight-loss program for couples. Health Psychology, 39(2), 137–146. https://doi.org/10.1037/hea0000808
- Gully, S. M., Incalcaterra, K. A., Joshi, A., & Beauien, J. M. (2002). A meta-analysis of team-efficacy, potency, and performance: Interdependence and level of analysis as moderators of observed relationships. Journal of Applied Psychology, 87(5), 819–832. https://doi.org/10.1037/0021-9010.87.5.819
- Hartmann, M. A., Datta, S., Banay, R. F., Caetano, V., Floreak, R., Appaiah, P., Sreevasthsa, A., Thomas, S., Selvam, S., Barnette, Q., & Srinivasan, K. (2018). Designing a pilot study protocol to test a male alcohol use and intimate partner violence reduction intervention in India: Beautiful Home. Frontiers in Public Health, 6, 218. https://doi.org/10.3389/fpubh.2018.00218
- Hoffmann, T. C., Glasziou, P. P., Boutron, I., Milne, R., Perera, R., Moher, D., Altman, D. G., Barbour, V., Macdonald, H., Johnston, M., Lamb, S. E., Dixon-Woods, M., McCulloch, P., Wyatt, J. C., Chen, A.-W., & Michie, S. (2014). Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ, 348(3), 1–12 https://doi.org/10.1136/bmj.g1687
- Hogan, B. E., Linden, W., & Najarian, B. (2002). Social support interventions: Do they work? Clinical Psychology Review, 22(3), 381–440. https://doi.org/10.1016/S0272-7358(01)00102-7
- Holt-Lunstad, J. (2021). The major health implications of social connection. Current Directions in Psychological Science, 30(3), 251–259. https://doi.org/10.1177/0963721421999630
- Holt-Lunstad, J., Birmingham, W., & Jones, B. Q. (2008). Is there something unique about marriage? The relative impact of marital status, relationship quality, and network social support on ambulatory blood pressure and mental health. Annals of Behavioral Medicine, 35(2), 239–244. https://doi.org/10.1007/s12160-008-9018-y
- Holt-Lunstad, J., Smith, T. B., Baker, M., Harris, T., & Stephenson, D. (2015). Loneliness and social isolation as risk factors for mortality: A meta-analytic review. Perspectives on Psychological Science, 10(2), 227–237. https://doi.org/10.1177/1745691614568352
- Holt-Lunstad, J., Smith, T. B., & Layton, J. B. (2010). Social relationships and mortality risk: A meta-analytic review. PLoS Medicine, 7(7), e1000316. https://doi.org/10.1371/journal.pmed.1000316
- Huelsnitz, C. O., Jones, R. E., Simpson, J. A., Joyal-Desmarais, K., Standen, E. C., Auster-Gussman, L. A., & Rothman, A. J. (2022). The dyadic health influence model. Personality and Social Psychology Review, 26(1), 3–34. https://doi.org/10.1177/10888683211054897
- Jackson, S. E., Steptoe, A., & Wardle, J. (2015). The influence of partner’s behavior on health behavior change: The English Longitudinal Study of Ageing. JAMA Internal Medicine, 175(3), 385–392. https://doi.org/10.1001/jamainternmed.2014.7554
- Keller, J., Hohl, D. H., Hosoya, G., Heuse, S., Scholz, U., Luszczynska, A., & Knoll, N. (2020). Long-term effects of a dyadic planning intervention with couples motivated to increase physical activity. Psychology of Sport and Exercise, 49, 101710-1–9. https://doi.org/10.1016/j.psychsport.2020.101710
- Knoll, N., Hohl, D. H., Keller, J., Schuez, N., Luszczynska, A., & Burkert, S. (2017). Effects of dyadic planning on physical activity in couples: A randomized controlled trial. Health Psychology, 36(1), 8–20. https://doi.org/10.1037/hea0000423
- Kok, G., Gottlieb, N. H., Peters, G. J. Y., Mullen, P. D., Parcel, G. S., Ruiter, R. A., Fernández, M., Markham, C., & Bartholomew, L. K. (2016). A taxonomy of behaviour change methods: An intervention mapping approach. Health Psychology Review, 10(3), 297–312. https://doi.org/10.1080/17437199.2015.1077155
- Koniak-Griffin, D., Lesser, J., Henneman, T., Huang, R., Huang, X., Tello, J., Kappos, B., González-Figueroa, E., & Cumberland, W. G. (2008). HIV prevention for Latino adolescent mothers and their partners. Western Journal of Nursing Research, 30(6), 724–742. https://doi.org/10.1177/0193945907310490
- Kulis, E., Szczuka, Z., Banik, A., Siwa, M., Boberska, M., Knoll, N., Radtke, T., Scholz, U., Rhodes, R. E., & Luszczynska, A. (2022). Insights into effects of individual, dyadic, and collaborative planning interventions on automatic, conscious, and social process variables. Social Science & Medicine, 314, 115477. https://doi.org/10.1016/j.socscimed.2022.115477
- Kulis, E., Szczuka, Z., Keller, J., Banik, A., Boberska, M., Kruk, M., Knoll, N., Radtke, T., Scholz, U., Rhodes, R. E., & Luszczynska, A. (2022). Collaborative, dyadic, and individual planning and physical activity: A dyadic randomized controlled trial. Health Psychology, 41(2), 134–144. https://doi.org/10.1037/hea0001124
- Lee, A. A., Piette, J. D., Heisler, M., Janevic, M. R., & Rosland, A. M. (2019). Diabetes self-management and glycemic control: The role of autonomy support from informal health supporters. Health Psychology, 38(2), 122–132. https://doi.org/10.1037/hea0000710
- Lewis, M. A., McBride, C. M., Pollak, K. I., Puleo, E., Butterfield, R. M., & Emmons, K. M. (2006). Understanding health behavior change among couples: An interdependence and communal coping approach. Social Science & Medicine, 62(6), 1369–1380. https://doi.org/10.1016/j.socscimed.2005.08.006
- Lewis, M. A., & Rook, K. S. (1999). Social control in personal relationships: Impact on health behaviors and psychological distress. Health Psychology, 18(1), 63–71. https://doi.org/10.1037/0278-6133.18.1.63
- Lüscher, J., Pauly, T., Gerstorf, D., Stadler, G., Ashe, M. C., Madden, K. M., & Hoppmann, C. A. (2022). Having a good time together: The role of companionship in older couples’ everyday life. Gerontology, 68(12), 1428–1439. https://doi.org/10.1159/000524089
- Lyons, R. F., Mickelson, K. D., Sullivan, M. J., & Coyne, J. C. (1998). Coping as a communal process. Journal of Social and Personal Relationships, 15(5), 579–605. https://doi.org/10.1177/0265407598155001
- Marques, M. M., Carey, R. N., Norris, E., Evans, F., Finnerty, A. N., Hastings, J., Jenkins, E., Johnston, M., West, R., & Michie, S. (2020). Delivering behaviour change interventions: Development of a mode of delivery ontology. Wellcome Open Research, 5, 125. https://doi.org/10.12688/wellcomeopenres.15906.2
- Marques, M. M., Wright, A. J., Johnston, M., West, R., Hastings, J., Zhang, L., & Michie, S. (2023). The Behaviour Change Technique Ontology: Transforming the Behaviour Change Technique Taxonomy v1. Transforming the Behaviour Change Technique Taxonomy, 8(308), 1–25. https://doi.org/10.31234/osf.io/vxypn
- Martinez, O., Fernandez, I. M., Wu, E., Carballo-Diéguez, A., Prado, G., Davey, A., Levine, E., Mattera, B., Lopez, N., Valentin, O., Murray, A., & Sutton, M. (2018). A couple-based HIV prevention intervention for Latino men who have sex with men: Study protocol for a randomized controlled trial. Trials, 19(1), 1–12. https://doi.org/10.1186/s13063-018-2582-y
- Martire, L. M., Schulz, R., Helgeson, V. S., Small, B. J., & Saghafi, E. M. (2010). Review and meta-analysis of couple-oriented interventions for chronic illness. Annals of Behavioral Medicine, 40(3), 325–342. https://doi.org/10.1007/s12160-010-9216-2
- McBride, C. M., Baucom, D. H., Peterson, B. L., Pollak, K. I., Palmer, C., Westman, E., & Lyna, P. (2004). Prenatal and postpartum smoking abstinence: A partner-assisted approach. American Journal of Preventive Medicine, 27(3), 232–238. https://doi.org/10.1016/j.amepre.2004.06.005
- Michie, S., Carey, R. N., Johnston, M., Rothman, A. J., De Bruin, M., Kelly, M. P., & Connell, L. E. (2018). From theory-inspired to theory-based interventions: A protocol for developing and testing a methodology for linking behaviour change techniques to theoretical mechanisms of action. Annals of Behavioral Medicine, 52(6), 501–512. https://doi.org/10.1007/s12160-016-9816-6
- Michie, S., Richardson, M., Johnston, M., Abraham, C., Francis, J., Hardeman, W., Eccles, M. P., Cane, J., & Wood, C. E. (2013). The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Annals of Behavioral Medicine, 46(1), 81–95. https://doi.org/10.1007/s12160-013-9486-6
- Moore, G. F., & Evans, R. E. (2017). What theory, for whom and in which context? Reflections on the application of theory in the development and evaluation of complex population health interventions. SSM - Population Health, 3, 132–135. https://doi.org/10.1016/j.ssmph.2016.12.005
- Myers Virtue, S., Manne, S. L., Kashy, D., Heckman, C. J., Zaider, T., Kissane, D. W., Kim, I., Lee, D., & Olekson, G. (2015). Correspondence of physical activity and fruit/vegetable consumption among prostate cancer survivors and their spouses. European Journal of Cancer Care, 24(6), 827–839. https://doi.org/10.1111/ecc.12316
- Newcomb, M. E., Sarno, E. L., Bettin, E., Carey, J., Ciolino, J. D., Hill, R., Garcia, C. P., Macapagal, K., Mustanski, B., Swann, G., & Whitton, S. W. (2020). Relationship education and HIV prevention for young male couples administered online via videoconference: Protocol for a national randomized controlled trial of 2GETHER. JMIR Research Protocols, 9(1), e15883. https://doi.org/10.2196/15883
- NIMH Multisite HIV/STD Prevention Trial for African American Couples Group. (2008). Methodological overview of an African American couple-based HIV/STD prevention trial. JAIDS Journal of Acquired Immune Deficiency Syndromes, 49(Suppl. 1), S3–S14. https://doi.org/10.1097/QAI.0b013e3181842570
- O'Farrell, T. J., & Murphy, C. M. (1995). Marital violence before and after alcoholism treatment. Journal of Consulting and Clinical Psychology, 63(2), 256–262. https://doi.org/10.1037/0022-006X.63.2.256
- O'Farrell, T. J., & Schein, A. Z. (2011). Behavioral couples therapy for alcoholism and drug abuse. Journal of Family Psychotherapy, 22(3), 193–215. https://doi.org/10.1080/08975353.2011.602615
- Oostingh, E. C., Koster, M. P., van Dijk, M. R., Willemsen, S. P., Broekmans, F. J., Hoek, A., Goddijn, M., Klijn, N. F., van Santbrink, E. J. P., Steegers, E. A. P., Laven, J. S. E., & Steegers-Theunissen, R. P. (2020). First effective mHealth nutrition and lifestyle coaching program for subfertile couples undergoing in vitro fertilization treatment: A single-blinded multicenter randomized controlled trial. Fertility and Sterility, 114(5), 945–954. https://doi.org/10.1016/j.fertnstert.2020.04.051
- Osuka, Y., Jung, S., Kim, T., Okubo, Y., Kim, E., & Tanaka, K. (2017). Does attending an exercise class with a spouse improve long-term exercise adherence among people aged 65 years and older: a 6-month prospective follow-up study. BMC Geriatrics, 17(1), 1–9. https://doi.org/10.1186/s12877-017-0554-9
- Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., Shamseer, L., Tetzlaff, J. M., Akl, E. A., Brennan, S. E., Chou, R., Glanville, J., Grimshaw, J. M., Hróbjartsson, A., Lalu, M. M., Li, T., Loder, E. W., Mayo-Wilson, E., McDonald, S., … Moher, D. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Systematic Reviews, 10(1), 89. https://doi.org/10.1186/s13643-021-01626-4
- Pitkälä, K. H., Pöysti, M. M., Laakkonen, M. L., Tilvis, R. S., Savikko, N., Kautiainen, H., & Strandberg, T. E. (2013). Effects of the Finnish Alzheimer disease exercise trial (FINALEX): A randomized controlled trial. JAMA Internal Medicine, 173(10), 894–901. https://doi.org/10.1001/jamainternmed.2013.359
- Prestwich, A., Conner, M. T., Lawton, R. J., Ward, J. K., Ayres, K., & McEachan, R. R. (2012). Randomized controlled trial of collaborative implementation intentions targeting working adults’ physical activity. Health Psychology, 31(4), 486. https://doi.org/10.1037/a0027672
- Prestwich, A., Conner, M. T., Lawton, R. J., Ward, J. K., Ayres, K., & McEachan, R. R. (2014). Partner- and planning-based interventions to reduce fat consumption: Randomized controlled trial. British Journal of Health Psychology, 19(1), 132–148. https://doi.org/10.1111/bjhp.12047
- Rhodes, R. E., Jones, L. W., & Courneya, K. S. (2002). Extending the theory of planned behavior in the exercise domain: A comparison of social support and subjective norm. Research Quarterly for Exercise and Sport, 73(2), 193–199. https://doi.org/10.1080/02701367.2002.10609008
- Richards, E. A., Franks, M. M., McDonough, M. H., & Porter, K. (2018). ‘Let’s move:’ A systematic review of spouse-involved interventions to promote physical activity. International Journal of Health Promotion and Education, 56(1), 51–67. https://doi.org/10.1080/14635240.2017.1415160
- Robinson, J. K., Turrisi, R., & Stapleton, J. (2007). Efficacy of a partner assistance intervention designed to increase skin self-examination performance. Archives of Dermatology, 143(1), 37–41. https://doi.org/10.1001/archderm.143.1.37
- Robles, T. F., & Kiecolt-Glaser, J. K. (2003). The physiology of marriage: Pathways to health. Physiology & Behavior, 79(3), 409–416. https://doi.org/10.1016/S0031-9384(03)00160-4
- Rook, K. S. (1987). Social support versus companionship: Effects on life stress, loneliness, and evaluations by others. Journal of Personality and Social Psychology, 52(6), 1132–1147. https://doi.org/10.1037/0022-3514.52.6.1132
- Rusbult, C. E., & Van Lange, P. A. (2003). Interdependence, interaction, and relationships. Annual Review of Psychology, 54(1), 351–375. https://doi.org/10.1146/annurev.psych.54.101601.145059
- Schenk, P., Wright, A. J., West, R., Hastings, J., Lorencatto, F., Moore, C., Hayes, E., Schneider, V., Howes, E., & Michie, S. (2023). An ontology of mechanisms of action in behaviour change interventions. https://doi.org/10.31234/osf.io/7jpm3
- Scholz, U., Berli, C., Goldammer, P., Lüscher, J., Hornung, R., & Knoll, N. (2013). Social control and smoking: Examining the moderating effects of different dimensions of relationship quality. Families, Systems, & Health, 31(4), 354–365. https://doi.org/10.1037/a0033063
- Scholz, U., Berli, C., Lüscher, J., & Knoll, N. (2020). Changing behavior using dyadic interventions. In M. S. Hagger, L. Cameron, K. Hamilton, N. Hankonen, & T. Lintunen (Eds.), The Handbook of behavior change (pp. 632–648). Cambridge University Press.
- Scholz, U., Stadler, G., Berli, C., Lüscher, J., & Knoll, N. (2021). How do people experience and respond to social control from their partner? Three daily diary studies. Frontiers in Psychology, 11, 613546. https://doi.org/10.3389/fpsyg.2020.613546
- Selcuk, E., & Ong, A. D. (2013). Perceived partner responsiveness moderates the association between received emotional support and all-cause mortality. Health Psychology, 32(2), 231–235. https://doi.org/10.1037/a0028276
- Shaffer, K. M., Tigershtrom, A., Badr, H., Benvengo, S., Hernandez, M., & Ritterband, L. M. (2020). Dyadic psychosocial eHealth interventions: Systematic scoping review. Journal of Medical Internet Research, 22(3), e15509. https://doi.org/10.2196/15509
- Siwa, M., Szczuka, Z., Banik, A., Kulis, E., Boberska, M., Wietrzykowska, D., Knoll, N., DeLongis, A., Knäuper, B., & Luszczynska, A. (2023). The dyadic interplay between relationship satisfaction, perceived positive and negative social control, and a reduction of sedentary behavior time. Annals of Behavioral Medicine, 57(2), 165–174. https://doi.org/10.1093/abm/kaac032
- Speizer, I. S., Zule, W. A., Carney, T., Browne, F. A., Ndirangu, J., & Wechsberg, W. M. (2018). Changing sex risk behaviors, gender norms, and relationship dynamics among couples in Cape Town, South Africa: Efficacy of an intervention on the dyad. Social Science & Medicine, 209, 95–103. https://doi.org/10.1016/j.socscimed.2018.05.024
- Stanforth, D., & Mackert, M. (2009). Social undermining of healthy eating and exercise behaviors. ACSM's Health & Fitness Journal, 13(3), 14–19. https://doi.org/10.1249/FIT.0b013e3181a1b79a
- Thong, M. S., Kaptein, A. A., Krediet, R. T., Boeschoten, E. W., & Dekker, F. W. (2007). Social support predicts survival in dialysis patients. Nephrology Dialysis Transplantation, 22(3), 845–850. https://doi.org/10.1093/ndt/gfl700
- Torvik, F. A., Røysamb, E., Gustavson, K., Idstad, M., & Tambs, K. (2013). Discordant and concordant alcohol use in spouses as predictors of marital dissolution in the general population: Results from the Hunt study. Alcoholism: Clinical and Experimental Research, 37(5), 877–884. https://doi.org/10.1111/acer.12029
- van der Wel, R. P., Becchio, C., Curioni, A., & Wolf, T. (2021). Understanding joint action: Current theoretical and empirical approaches. Acta Psychologica, 215, 103285. https://doi.org/10.1016/j.actpsy.2021.103285
- van Dijk, M. R., Koster, M. P., Oostingh, E. C., Willemsen, S. P., Steegers, E. A., & Steegers-Theunissen, R. P. (2020). A mobile app lifestyle intervention to improve healthy nutrition in women before and during early pregnancy: Single-center randomized controlled trial. Journal of Medical Internet Research, 22(5), e15773. https://doi.org/10.2196/15773
- Voils, C. I., Shaw, R., Adler, R., Jeanes, E., Lewis, M. A., Sharp, W., Cronin, K. A., Hetzel, S., Mao, L., Johnson, H. M., Elwert, F., Pabich, S., Gavin, K. L., Yancy, W. S., & Porter, L. S. (2020). Protocol for Partner2Lose: A randomized controlled trial to evaluate partner involvement on long-term weight loss. Contemporary Clinical Trials, 96, 106092. https://doi.org/10.1016/j.cct.2020.106092
- Voils, C. I., Yancy, W. S., Kovac, S., Coffman, C. J., Weinberger, M., Oddone, E. Z., Jeffreys, A., Datta, S., & Bosworth, H. B. (2009). Study protocol: Couples partnering for lipid enhancing strategies (CouPLES) - A randomized, controlled trial. Trials, 10(1), 1–9. https://doi.org/10.1186/1745-6215-10-10
- Wakefield, M., & Jones, W. (1998). Effects of a smoking cessation program for pregnant women and their partners attending a public hospital antenatal clinic. Australian and New Zealand Journal of Public Health, 22(3), 313–320. https://doi.org/10.1111/j.1467-842X.1998.tb01383.x
- Wegner, D. M., Erber, R., & Raymond, P. (1991). Transactive memory in close relationships. Journal of Personality and Social Psychology, 61(6), 923–929. https://doi.org/10.1037/0022-3514.61.6.923
- Winters-Stone, K. M., Lyons, K. S., Nail, L. M., & Beer, T. M. (2012). The exercising together project: Design and recruitment for a randomized, controlled trial to determine the benefits of partnered strength training for couples coping with prostate cancer. Contemporary Clinical Trials, 33(2), 342–350. https://doi.org/10.1016/j.cct.2011.10.015
- Woodin, E. M., & O’Leary, K. D. (2010). A brief motivational intervention for physically aggressive dating couples. Prevention Science, 11(4), 371–383. https://doi.org/10.1007/s11121-010-0176-3
- Wooldridge, J. S., Ranby, K. W., Roberts, S., & Huebschmann, A. G. (2019). A couples-based approach for increasing physical activity among adults with type 2 diabetes: A pilot feasibility randomized controlled trial. The Diabetes Educator, 45(6), 629–641. https://doi.org/10.1177/0145721719881722
- Worden, B. L., Epstein, E. E., & McCrady, B. S. (2015). Pretreatment assessment-related reductions in drinking among women with alcohol use disorders. Substance Use & Misuse, 50(2), 215–225. https://doi.org/10.3109/10826084.2014.962662
- Yang, Y. C., Boen, C., Gerken, K., Li, T., Schorpp, K., & Harris, K. M. (2016). Social relationships and physiological determinants of longevity across the human life span. Proceedings of the National Academy of Sciences, 113(3), 578–583. https://doi.org/10.1073/pnas.1511085112
- Young, V. J., Burke, T. J., & Curran, M. A. (2019). Interpersonal effects of health-related social control: Positive and negative influence, partner health transformations, and relationship quality. Journal of Social and Personal Relationships, 36(11–12), 3986–4004. https://doi.org/10.1177/0265407519846565