
Abstract
Recurrent spontaneous abortion (RSA) is defined as two or more consecutive pregnancy failures, which brings tremendous stress to women of childbearing age and seriously affects family well-being. However, the reason in about 50% of cases remains unknown and is defined as unexplained recurrent spontaneous abortion (URSA). The immunological perspective in URSA has attracted widespread attention in recent years. The embryo is regarded as a semi-allogeneic graft to the mother. A successful pregnancy requires transition to an immune environment conducive to embryo survival at the maternal–fetal interface. As an important member of regulatory immunity, regulatory T (Treg) cells play a key role in regulating immune tolerance at the maternal–fetal interface. This review will focus on the phenotypic plasticity and lineage stability of Treg cells to illustrate its relationship with URSA.
Introduction
Immune self-stabilization is one of the three functions of human immune system.Citation1 Regulatory T (Treg) cells are named for their powerful function in regulating the immune system and improving immunological self-tolerance, which plays an important role in immune homeostasis.Citation2,Citation3 Treg cells have been confirmed to be related to various immunological diseases such as rheumatoid arthritis (RA), type 1 diabetes, allergy and graft-versus-host disease (GVHD).Citation4–7 In recent years, substantial evidence has shown that Treg cells play a major role in fetal-maternal tolerance.Citation8–10 Treg cells not only suppress inflammation but also prevent the adverse effects of anti-fetal alloantigen, facilitating essential vascular adaptations crucial for placental morphogenesis at the maternal–fetal interface.Citation11–14 In the first trimester of human pregnancy, T cells comprise 10% to 20% of decidual immune cells,Citation15 of which Treg cells account for 10–30% of the CD4+ T cells.Citation16,Citation17 Phenotypic plasticity is an important characteristic of Treg cells, and lineage stability of Treg cells is crucial for their function. Since the 1970s, scholars have made efforts to characterize Treg cells by reliable molecular markers.Citation18 In the mid-1990s, Sakaguchi et al discovered that Treg cells constitutively and highly expressed CD25.Citation19 In 2003, transcription factor Fork head box P3 (FoxP3) was found specifically expressed in CD25+CD4+ natural Treg cells in rodents and human,Citation20–22 which is a key determinant of their suppressive function. Subsequently, in order to better elucidate its function and heterogeneity, more and more markers have been found to characterize its phenotype, such as Helios, neuropilin-1 (Nrp-1), inducible co-stimulator (ICOS), programmed cell death protein 1 (PD-1), ITIM domain protein (TIGIT) and T cell immunoglobulin and mucin domain-containing protein 3 (TIM-3), etc.Citation23–27 However, phenotypic plasticity and lineage stability of Treg cells is still a controversial topic.
Recurrent spontaneous abortion (RSA) is defined as two or more consecutive pregnancy failures according to the guidelines of the American Society of Reproductive Medicine.Citation28 A lot of evidence indicates that RSA is related to genetic defects, immune disorders, abnormal genital structure, specific and nonspecific inflammation, endocrine disorders and other factors.Citation29–32 The etiology of RSA is complex, and more than 50% of patients are unknown.Citation33 As the number of miscarriages increases, the likelihood of URSA women experiencing early miscarriage, premature birth, placenta previa and other related complications also increase when they become pregnant again.Citation34,Citation35 This can be serious adverse effects on women with URSA. In recent years, the immunological perspective in recurrent miscarriage (RM) has attracted widespread attention. Successful pregnancy requires the attachment of the embryo to the endometrium, decidualization of the endometrium, and the differentiation of blastocysts into trophoblasts to invade the decidua.Citation10,Citation36 Abundant immune cells reside in the decidua in close contact with paternally derived alloantigens and fetal tissues. They participate in the establishing, sustaining and terminating pregnancy extensively.Citation10 As a member of regulatory immunity, the significance of Treg cells during the implantation and maintenance of the healthy pregnancy is evident. However, the role of Treg cells in URSA is still a topic worthy of further study. This review delves into the phenotypic plasticity and lineage stability of Treg cells and elucidates the relationship between Treg cell functions and URSA, aiming to present novel insights for immunological approaches to treating URSA.
Classification of Treg Cells
According to differentiation, Treg cells can be categorized into two groups: natural Treg (nTreg) cells and induced Treg (iTreg) cells. During thymus development, immature T lymphocytes produce nTreg cells, identified by the presence of CD4+CD25+Foxp3+ T cells. Conversely, mature CD4+CD25− T cells can convert into iTreg cells under stimulation of peripheral antigen or induction of immunosuppressive factors. iTreg cells can be divided into Type 1 regulatory T (Tr1) and Th3 subsets. Tr1 Treg cells mainly produce interleukin (IL)-10, while Th3 cells primarily secrete transforming growth factor beta (TGF-β).Citation4,Citation37
In recent years, scholars have recommended that Treg cells can be classified into two categories according to their origins. The aforementioned nTreg cells may be termed thymus-derived Treg (tTreg) cells, originating from the thymus with a T-cell receptor (TCR) featuring relatively high self-affinity.Citation38 Periphery-derived Treg (pTreg) cells develop from CD4+ effector cells under TCR signal transduction or other factors (such as TGF-β, IL-2),Citation39 which mainly exist in peripheral barrier tissues and play an important role in controlling local inflammation.Citation40
According to the function and location, Treg cells can also be divided into central Treg (cTreg) cells and effector Treg (eTreg) cells.Citation41 cTreg cells, expressing CC-chemokine receptor (CCR) 7 and L-Selectin (CD62L) at high levels, are mainly located in peripheral lymphoid tissue.Citation42 eTreg cells are mainly found in non-lymphoid tissues and can be identified by the presence of surface markers like ICOS or CD44.Citation43 They exhibit a remarkable ability to adapt and specialize to specific tissue environments.Citation44,Citation45
Immunosuppressive Mechanism of Treg Cells
The immunosuppressive effect of Treg cells is primarily accomplished through the interaction of their inhibitory surface molecules with other immune cells. TIGIT presented on Treg cells interacts with CD155 on dendritic cells (DCs) to suppress the activation of effector T cells (Teffs), Th1, and Th17, which is achieved by IL-10 augmentation and IL-12 reduction.Citation46–49 Cytotoxic T lymphocyte-associated antigen-4 (CTLA-4) on Treg cells interacts with CD80 and CD86 on antigen-presenting cells (APCs), which results in the inhibition of antigen presentation and maturation functions of APCs.Citation50 Furthermore, the activation of indoleamine 2,3-dioxygenase (IDO) expressed in DCs ultimately leads to the suppression of Teffs.Citation51 PD-1 binds to its ligand PD-L1 and PD-L2 on DCs, which gives rise to the inhibition of Teffs via enhancing the transactivation of Smad3 by TGF-β.Citation52 Binding of lymphocyte activation gene 3 (LAG-3) to major histocompatibility complex class II (MHC-II) molecules expressed on immature DCs induces inhibitory signaling pathways which suppresses DCs maturation and the activation of Teffs.Citation53 Caspase-8 activated by the combination of tumor necrosis factor (TNF)–related apoptosis-inducing ligand (TRAIL) and death receptor 5 (DR5) induces apoptosis in effector lymphocytes.Citation54,Citation55 CD25, also known as interleukin IL-2 receptor (IL-2R), has been demonstrated to control the acquisition of cytotoxic activity of CD4+T cells by competing for IL-2.Citation56
In addition to the molecules mentioned above, Treg cells exert their immunosuppressive functions through soluble intermediates. New evidence emphasizes the significance of adenosine and cAMP in the ability of Treg cells to inhibit Teffs.Citation57,Citation58 Ectoenzymes CD39 and CD73 expressed on Treg cells were shown to raise the concentration of adenosine, which suppressed the function of Teffs through activating the adenosine A2A receptor.Citation59,Citation60 Granzyme-A, granzyme-B and perforin ensure the cytolysis of Treg cells to other immune cells, such as B cells, NK cells and CD8+ T cells.Citation61–64 Anti-inflammatory cytokines, such as IL-10, TGF-β and IL-35, mediate the anti-inflammatory effect of Treg cells.Citation65
The Relationship with Pregnancy
The Origin of Decidual Treg Cells
Decidual Treg cells originate from peripheral blood Treg cells, including tTreg cells and pTreg cells, exhibiting varying phenotypic heterogeneity according to the cycle and environment.Citation27,Citation66,Citation67 Recruitment of Treg cells into the uterus commences in endometrial proliferation stage of each cycle and peaks at ovulation.Citation68 Estrogen in uterine and TGF-β and prostaglandin (PGE) in seminal fluid play a role in recruiting macrophages and DCs, which makes them acquire M2 macrophages and tolerogenic DCs (tDCs) phenotypes. Interferon-gamma (IFN-γ) and IL-10 secreted by uterine natural killer (uNK) cells, Granulocyte-macrophage CSF (GM-CSF) and chemokines secreted by uterine epithelial cells also facilitate the acquirement of M2 macrophages and tDC phenotypes.Citation69,Citation70 tDCs take up paternal alloantigens in seminal fluid and present antigen to Th0 cells in uterus-draining para-aortic lymph nodes (PALNs).Citation71,Citation72 Later, Th0 cells can be activated and differentiated into pTreg cells. In mice, systemic expansion and accumulation of tTreg cells in the PALNs and uterus occur during the estrous stage in response to elevated levels of estradiol (E2) at ovulation.Citation73 During and before embryo implantation, pTreg and tTreg cells are recruited to the uterus and retained there. Treg cells increased in the early and middle trimesters and decreased prior to delivery, which is the similar pattern as Treg cells in peripheral blood.Citation74
Regulating Trophoblasts Invasion and Uterine Spiral Artery Remodeling
Embryo implantation necessitates trophoblast infiltration and remodeling of the uterine spiral arteries (SpA). During embryo implantation priming, the excessive production of IL-2 and IFN-γ enhances the development of cytotoxic CD8+ T cells, which subsequently contribute to fetal loss.Citation75 Meanwhile, unrestrained Teffs release inflammatory cytokines and play cytotoxicity effect on trophoblast through antigen-dependent, which adversely affects placental development.Citation75,Citation76 Decidual Treg cells may contribute to constraining Teffs in early pregnancy by expressing CTLA4, CD25, and PD-L1, and secreting TGF-β as well as IL-10.Citation77,Citation78
A variety of immune cells play a synergistic role in the embryo implantation, such as uNK cells, uterine dendritic cells (uDC) and uterine mast cells (uMC).Citation79–81 Treg cells cooperate with them to support the formation of decidua and promote embryo implantation.Citation59 M2 macrophages, tDC and uNK cells promote the peripheral differentiation of Treg cells and recruitment to the uterus.Citation69,Citation70 On the one hand, Treg cells respond to epithelial cell-derived chemokine C-C motif ligand (CCL) 3, CCL4, CCL5, and CCL19.Citation82,Citation83 Meanwhile, they inhibit the activation and function of Th1 and Th17 cells by consuming IL-2 or other inhibitory mechanisms.Citation77,Citation78,Citation84 On the other hand, Treg cells control inflammation by releasing TGF-β, IL-10 and heme oxygenase-1 (HO-1) to interact with DCs and uNK cells.Citation77,Citation78,Citation85 This eventually facilitated decidualization and embryo implantation.Citation51,Citation85–88 Besides, the regulatory loop between trophoblasts and maternal immune cell subsets might be bidirectional. An interesting finding suggests that trophoblasts regulated the differentiation of maternal CD4+T cells into immunosuppressive Treg cells, while CD4+T cells might promote the growth and invasiveness of trophoblasts.Citation89
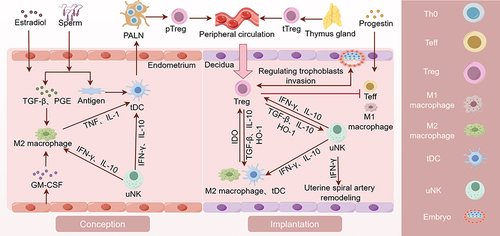
In recent years, increasing evidence has shown that Treg cells play an important role in the vascular endothelium and blood flow homeostasis.Citation13,Citation14 uNK cells regulate the invasion of extravillous trophoblasts as well as displacement of endothelial cells and smooth muscle cells (SMCs) by releasing IFN-γ, which ultimately facilitates the decidual vascular remodeling.Citation81,Citation90,Citation91 Treg cells suppress inflammatory activation and modulate the phenotypes of decidual uNK cells, macrophages and DCs by releasing TGF-β, IL-10 and HO-1, which promotes the decidual vascular remodeling.Citation16,Citation77,Citation78,Citation85 Treg cells restrict the activation and infiltration of M1 macrophages, so as to reduce the release of tumor necrosis factor α (TNF-α) and improve the vascular endothelial microenvironment.Citation13,Citation14 At the same time, they inhibit the erosive effect of Th1 and Th17 on blood vessels,Citation12,Citation78 which gives rise to diminished vascular resistance and increased blood supply to the placenta ().
Figure 1 Mechanisms of Treg Cells in Female Pregnancy. Estrogen and semen recruit macrophages and DCs, which promotes their polarization towards M2 macrophages and tDC phenotypes. tDCs uptake paternal antigens in semen and transport them to the PALN draining the uterus. Under the stimulation of paternal antigens, Th0 cells in PALN differentiate into pTreg cells. pTreg cells and tTreg cells converge in the peripheral circulation and re-enter the uterine cavity during the implantation stage to exert their functions. Decidual Treg cells restrict Teffs by secreting IL-10 and TGF-β and expressing CD25, CTLA4 and PD-L1, which directly promotes the embryo implantation. Additionally, they work in collaboration with decidual immune cells to promote decidualization and enhance endometrial receptivity. Treg cells not only directly inhibit Teffs and M1 macrophages, but also work in collaboration with M2 macrophages, uNK, and tDC cells to promote trophoblast invasion and vascular remodeling. PALN, para-aortic lymph node. (By Figdraw).
The Phenotypes of Decidual Treg Cells
The Treg cell population during pregnancy exhibits remarkable diversity, both in the peripheral blood and at the maternal–fetal interface.Citation9 Until now, the populations of Treg cells at the maternal–fetal interface and their contribution to the decidual microenvironment have not been fully defined. Originally, a population of CD4+CD25+ T cells, expressing intracellular CTLA-4, glucocorticoid-induced tumor necrosis factor receptor-related protein (GITR) and OX40 (CD134), was identified in the human decidua.Citation92 It is implied that Treg cells exist in decidua and play an important role in the regulation of local maternal tolerance towards the fetus.Citation92 Later, Dimova firstly demonstrated the presence and in situ distribution of CD4+ Foxp3+ cells in decidua,Citation93 which were classified into CD4+ CD25++ Foxp3+, CD4+ CD25+ Foxp3+, and CD4+ CD25− Foxp3+ subpopulations on the basis of CD25 expression.Citation93 These Foxp3+ cells were found to express TGFβ1 mRNA and exhibit surface molecules consistent with Treg phenotype, including CD45RO (a marker for memory lymphocytes), CTLA-4, CD103, Nrp-1, LAG-3, and CD62L.Citation93
Recently, three distinct types of decidual CD4+ Treg cells in healthy pregnancies were investigated, whose phenotypes are CD25HI FoxP3+, PD1HI FoxP3− IL-10+ and TIGIT+ FoxP3dim Treg cells.Citation94 The characteristics of these three types of Treg cells are summarized in . In comparison to Treg cells in the blood, CD25HIFoxP3+ Treg cells in the decidual tissue exhibit higher levels of co-inhibitory proteins or mRNAs, such as CTLA-4, GITR, CD39, ST2, and LRRC32.Citation94 This observation indicates an enhanced activation and suppressive function of Treg cells in the decidual tissue, which plays a crucial role in regulating inflammation at the maternal–fetal interface.
Table 1 Different Phenotypes of Treg Cells During Pregnancy
Unlike the studies above, a systematic review discussed the heterogeneity within the FoxP3− Treg cell compartment and their role in pregnancy.Citation9 FoxP3−HLA-G+Treg cells have been identified in both decidua and peripheral blood during pregnancy, which plays a crucial role in establishing a tolerogenic decidual microenvironment by secreting IL-10 and soluble HLA-G.Citation95–97 Tr1 Treg cells, which primarily product IL-10Citation98–100 and express co-signaling molecules such as PD-1, CTLA-4, TIM-3, ICOS, GARP (LRRC32), and latency associated peptide (LAP),Citation101–103 are also found in both peripheral blood and human decidua.Citation94,Citation104 Additionally, the observation of mRNA cytokine profiles similar to Th3 represents the first description of a potential presence of Th3 cells in the decidua.Citation93 The main suppressive effects of Th3 Treg cells are mediated by TGF-β in a cell-contact independent mannerCitation105,Citation106 ().
The Relationship with URSA
CD4+ CD25+ Treg-deficient mouse model was established to demonstrate that allogeneic fetuses are consistently rejected without Treg cells.Citation107 Transferring of Treg cells into mice prone to miscarriage resulted in an increase number of uMC, which possess a positive impact on the remodeling of the placenta and SpA.Citation108 Both in the peripheral blood and decidua, the number and function of Treg cells are diminished in women experiencing recurrent pregnancy loss (RPL), when compared to women in control group.Citation109 This evidence confirmed that insufficient Treg numbers or inadequate function were implicated in RSA.Citation10 The following is the main hypothesis of the relationship between Treg cells and URSA.
Systemic Immune Imbalance
A number of scholars have analyzed the endometrial cytokine profile in normal female and patients with recurrent abortion. The luteal-phase endometrium of patients with URSA exhibited increased expression of the inflammatory mediators, such as TNF-α, IL-1β and IFN-γ.Citation110,Citation111 At the same time, the levels of TGF-β, IL-4, IL-10, leukemia inhibitory factor (LIF), and vascular endothelial growth factor (VEGF) were reduced in the endometrium of URSA patients during the luteal phase.Citation110,Citation111 In addition, several studies demonstrated that the endometrium of women with URSA was accompanied by the alteration of uNK cells and reduced expression of key angiogenic regulators.Citation112–115 TGF-β and IL-10 secreted by Treg cells were not only involved in immune regulation but also directly benefited the vasculature at the maternal–fetal interface.Citation116 The increased level of TGF-β1 in serum may lead to a reduction in the abortion rate in a mouse model prone to miscarriage.Citation117 Overall, this evidence indicates that the embryo may not survive in the inflammatory stage of implantation due to the failure to transition to an anti-inflammatory and proangiogenic immune environment. These dysfunctions may be associated with reduced numbers of Treg cells and the increase of Th17, Th1 and M1 macrophages in decidua and peripheral blood.Citation118–123
Phenotypic Plasticity and Lineage Stability
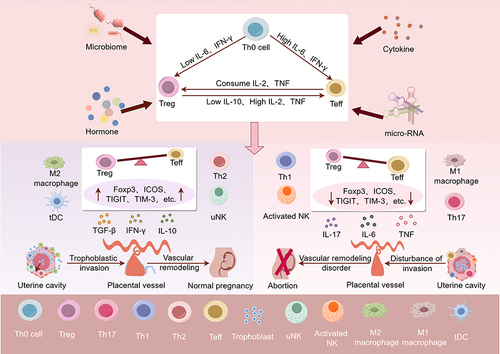
Cytokines, hormones, micro-RNAs, the reproductive tract microbiome, and seminal fluid composition all have the potential to interfere with the response of Treg cells,Citation124–127 because the newly generated pTreg cells are susceptible to lineage instability and phenotype switching.Citation128 CD4+ T cells from patients with RM were cultured with DCs and the partner’s seminal fluid antigens, which suggested that CD4+IL-17+and CD4+IFN-γ+cells proliferated excessively.Citation129 At the same time, the study revealed that fewer CD4+CD25+FoxP3+ Treg cells were generated by patients with RM compared with fertile controls.Citation129 High levels of IFN-γ could skew Th0 differentiation toward Th17 cells and caused Treg cells to transdifferentiate.Citation130,Citation131 In addition, deficiency in IL-10 triggers an unstable Treg response in the decidua, resulting in a quicker conversion of phenotypes and impairing ability to effectively anti-inflammation during the later stages of pregnancy.Citation132,Citation133 There remains a highly contentious topic: pTreg cells shift the phenotypes and express cytokines that are characteristic of Teff lineages within hyperinflammatory environment.Citation128,Citation131 Treg cells undergoing trans-differentiation into Th1 or Th17 cells were known as exTreg cells, which promote inflammation and other immune responses.Citation128 The phenotypic plasticity and switching abilities of Treg cells may contribute to the maternal ability to invest differently in reproductive opportunities. In normal circumstances, Treg cells maximize the maternal decidual receptivity and offspring adaptability by interacting with the environment, hormones, and cells.Citation126,Citation128,Citation134 However, there is also study showing that excessive immune adaptation during pregnancy might predispose pregnant females to the susceptibility of viral infections.Citation135 The ability of Treg cells to transdifferentiate into Teffs under conditions of severe infection, excessive inflammation, or disruption of fetal development allows for the termination of pregnancy to preserve maternal survival.Citation136
Recently, evidence has focused on immune checkpoint molecules and stability markers of Treg cells, such as Foxp3, Helios, Nrp-1, ICOS, PD-1, TIGIT and TIM-3, which is aimed to explain the stability of inhibitory function of Treg cells.Citation23–27 The signature of endometrial Treg transcriptomic was identified.Citation118 The researchers observed increased expression of sphingosine-1-phosphate receptor 1 (S1PR1) and decreased levels of TIGIT protein in women with primary URSA, which suggested reduced inhibitory capacity of Treg cells in women with primary URSA.Citation118 In addition, Hu et al discovered that Tim3+ Treg cells constituted over 60% Treg cells in the mouse decidua during early pregnancy.Citation8 Meanwhile, they observed the significantly lower Tim-3 expression on Treg cells in URSA, indicating that decreased Tim-3+ Treg cells might have a close relationship with impaired immunologic tolerance in women suffering URSA.Citation8 In addition, Treg cells from women with RM exhibited fewer CD45RA– cells and reduced expression of CTLA4 and Ubc13(an ubiquitin E2 conjugating enzyme),Citation66 which implied that the stability of Treg cells was reduced in URSACitation120,Citation129,Citation137 ().
Figure 2 The relationship between Decidual Treg cells and URSA. In human, cytokines, hormones, micro-RNAs, the reproductive tract microbiome, and seminal fluid composition all have the potential to interfere with the immune balance at the maternal–fetal interface. High levels of IL-6 and IFN-γ could skew Th0 differentiation toward Teffs and cause Treg cells to transdifferentiate. Newly generated pTreg cells are susceptible to lineage instability and phenotype switching. High levels of IL-2, TNF and low levels of IL-10 could skew pTreg cells differentiation toward Teffs. If pTreg cells express additional markers associated with functional stability, such as Foxp3, ICOS, TIGIT, and TIM3, it could potentially shift the immune balance at the maternal–fetal interface towards immune tolerance. This may lead to elevated TGF-β, IL-10, M2 macrophages and tDC cells, which promotes trophoblast invasion, vascular remodeling and placental development. Conversely, if the newly generated pTreg cells are unstable, it could shift the immune balance at the maternal–fetal interface towards pro-inflammation. This could result in elevated IL-6, IL-17, TNF, M1 macrophages, Th1 cells and etc, which may hinder trophoblast invasion, vascular remodeling, and ultimately causing placental dysplasia and URSA. (By Figdraw).
Therapeutic Prospects for Targeting Treg Cells
Reproductive disorders caused by instability or insufficient production of Treg cells pose a challenging problem to be addressed, which may be the result of multiple factors in the biological evolution process.Citation27,Citation66,Citation134,Citation138 Interventions aimed at increasing the number and improving the function of Treg cells are currently being developed and are showing promise in the treatment of tissue transplantation and autoimmune diseases. With the rapid progress in Treg cell therapeutics, there is a great potential for targeting Treg cells to address URSA.Citation139 Here, we propose three points:
Signaling of Treg Cells and Stability
In recent years, some scientists have proposed promoting the stability of Treg cells through selective gene knockout. However, the safety concerns associated with this approach must be taken into consideration. For example, IL-6 triggers the signal transducer and activator of transcription 3 (STAT3) transduction pathway, which then induces the expression of the DNA methyltransferase 1 (DNMT1).Citation140,Citation141 This leads to the methylation and subsequent downregulation of the Foxp3 site, ultimately resulting in the development of naive T cells into Th17 cells.Citation142 Therefore, targeting IL-6 receptor (IL-6R) or STAT3 in Treg cells could be a viable strategy to enhance the stability of Treg cells and protect them from alterations caused by IL-6 signaling.Citation143 In human, IL-6R-targeted antibodies have been identified as a potential therapeutic approach for inflammatory and autoimmune diseases like RA, Crohn’s disease, and systemic lupus erythematosus (SLE).Citation144–146
IL-2 plays a crucial role in the generation, survival, stability, and function of Treg cells.Citation147 In the absence of IL-2, Treg cells undergo apoptotic death, which leads to autoimmunity.Citation148 Therefore, various strategies have been developed to utilize IL-2 as a therapeutic pathway to improve the stability, effectiveness and survival of Treg cells in vivo.Citation147,Citation149 The hypothesis suggests that administering low doses of IL-2 would primarily activate Treg cells and restrict the activation of Teffs, which is contrary to the impact of high doses of IL-2.Citation150–153 Two therapeutic strategies targeting IL-2 have primarily been developed, and IL-2 low-dose therapy and monoclonal antibodies that target IL-2. F5111.2, a fully human anti-IL-2 antibody, were recently developed to induce the preferential expansion of human Treg cells by blocking IL-2Rβ and reducing IL-2Rα.Citation152
Interventions to Increase Treg Cell Numbers
The decrease in number of Treg cells in the decidua of women with URSA is likely a consequence of impaired generation or recruitment of Treg cells during pregnancy establishment,Citation118,Citation154 which suggests that Treg cells possess therapeutic potential in women with URSA.Citation155 Co-expression of a chemokine receptor, which could identify chemokines in an inflammatory environment, may improve Treg cell functionality.Citation143 In related studies, overexpression of chemokine receptors has been found to improve chimeric antigen receptor (CAR) T cells homing to the tumor, resulting in enhanced antitumor activity and improved survival.Citation156–158 A recent study elucidated that histone methyltransferase Nsd2 upregulated the expression of C-X-C chemokine receptor type 4 (CXCR4) through the H3K36me2 modification, which plays a crucial role in promoting the recruitment of Treg cells into the decidua and ultimately improved pregnancy outcomes in mice.Citation159
In addition to the methods of increasing number of Treg cells endogenously, methods of artificially supplementing Treg cells have been developed. The method of adoptive transplantation of Treg cells to improve the prognosis of spontaneous abortion has demonstrated effectiveness in mouse models and is anticipated to be a promising immunological treatment for women with URSA.Citation155 Evidence suggests that Treg cells from umbilical cord blood display higher repertoire diversity and lineage stability compared to those from adult peripheral blood, providing a feasible basis for Treg cell therapy.Citation160 Before the development of endogenous Treg cells from a donor’s bone marrow cells, using cord blood-derived Treg cells could offer a temporary solution.Citation143
Behavioral and Pharmacological Interventions in URSA
Metabolic, autoimmune conditions, inflammatory exposures and age strongly affect the immune response.Citation139,Citation161–163 Metabolic imbalance, such as hyperglycemia and insulin resistance, will skew the energy source driving the T cell pool, which eventually results in an increased number of Th17 cells and declined in the number of Treg cells.Citation164 Microbiome disorders, deficiencies in micronutrients and vitamins have a specific impact on Treg cells. Treating these disorders and deficiencies is anticipated to enhance uterine immune function,Citation165 which may improve the prognosis of URSA in turn.
Besides, preexisting health conditions and lifestyle factors are also significant in male partners, because of the affection of seminal fluid quality and healthy female response.Citation166 Incompatibility or insufficient disparity of HLA between partners may lead to low immunogenicity of male alloantigens, leading to either excessive inhibition or activation of uNK cells or hindering the priming and expansion of the Treg cell population.Citation167 Providing guidance on seminal fluid priming during preconception planning may be a promising approach for nulliparous women without known compatibility issues.Citation167 More interestingly, exercise and sunlight exposure potentially increase Treg cells by regulating their homeostasis.Citation168,Citation169 Intravenous immunoglobulin, prednisolone, and TNF inhibitors, initially developed for other autoinflammatory or specific autoimmune diseases,Citation61,Citation170–172 have been investigated in patients with URSA and recurrent implantation failure. However, the clinical data supporting efficacy are limited.Citation173 Progesterone has been shown to effectively inhibit the generation of Th1 and Th17 cells while also inducing Treg cell differentiation.Citation61,Citation174–176
Conclusion and Prospects
The combination of animal models and clinical studies provide evidence that decidual Treg cells play a role in reducing inflammation during the early pregnancy. They also contribute to creating an environment in the decidua that supports implantation receptivity and placenta formation. Immune maladaptation or imbalance leading to instability or insufficient of Treg cells, which may be a cause of URSA. A large number of studies should be devoted to investigate the subsets of Treg cells, which can gain more insights into their functions and roles in URSA. It is necessary to continually explore ways to improve the number and stability of Treg cells, which may be a therapeutic target for URSA.
Disclosure
The authors report no conflicts of interest in this work.
Additional information
Funding
References
- Förster R, Davalos-Misslitz AC, Rot A. CCR7 and its ligands: balancing immunity and tolerance. Nat Rev Immunol. 2008;8(5):362–371. doi:10.1038/nri2297
- Sakaguchi S, Mikami N, Wing JB, Tanaka A, Ichiyama K, Ohkura N. Regulatory T cells and human disease. Annu Rev Immunol. 2020;38:541–566. doi:10.1146/annurev-immunol-042718-041717
- Sakaguchi S, Yamaguchi T, Nomura T, Ono M. Regulatory T cells and immune tolerance. Cell. 2008;133:775–787. doi:10.1016/j.cell.2008.05.009
- Jiang Q, Yang G, Liu Q, Wang S, Cui D. Function and Role of Regulatory T Cells in Rheumatoid Arthritis. Front Immunol. 2021;12:626193. doi:10.3389/fimmu.2021.626193
- Turner JA, Stephen-Victor E, Wang S, et al.. Regulatory T Cell-Derived TGF-β1 controls multiple checkpoints governing allergy and autoimmunity. Immunity. 2020;53:1202–1214.e6. doi:10.1016/j.immuni.2020.10.002
- Bettini M, Bettini ML. Function, Failure, and the Future Potential of Tregs in Type 1 Diabetes. Diabetes. 2021;70:1211–1219. doi:10.2337/dbi18-0058
- Daenthanasanmak A, Iamsawat S, Chakraborty P, et al.. Targeting Sirt-1 controls GVHD by inhibiting T-cell allo-response and promoting Treg stability in mice. Blood. 2019;133:266–279. doi:10.1182/blood-2018-07-863233
- Hu X, Zhu Q, Wang Y, et al.. Newly characterized decidual Tim-3+ Treg cells are abundant during early pregnancy and driven by IL-27 coordinately with Gal-9 from trophoblasts. Hum Reprod. 2020;35:2454–2466. doi:10.1093/humrep/deaa223
- Krop J, Heidt S, Claas F, Eikmans M. Regulatory T Cells in Pregnancy: it Is Not All About FoxP3. Front Immunol. 2020;11:1182. doi:10.3389/fimmu.2020.01182
- Robertson SA, Care AS, Moldenhauer LM. Regulatory T cells in embryo implantation and the immune response to pregnancy. J Clin Invest. 2018;128:4224–4235. doi:10.1172/JCI122182
- Care AS, Bourque SL, Morton JS, Hjartarson EP, Robertson SA, Davidge ST. Reduction in regulatory T cells in early pregnancy causes uterine artery dysfunction in mice. Hypertension. 2018;72:177–187. doi:10.1161/HYPERTENSIONAHA.118.10858
- Samstein RM, Josefowicz SZ, Arvey A, Treuting PM, Rudensky AY. Extrathymic generation of regulatory T cells in placental mammals mitigates maternal-fetal conflict. Cell. 2012;150:29–38. doi:10.1016/j.cell.2012.05.031
- Tamosiuniene R, Manouvakhova O, Mesange P, et al.. Dominant role for regulatory T cells in protecting females against pulmonary hypertension. Circ Res. 2018;122:1689–1702. doi:10.1161/CIRCRESAHA.117.312058
- Sharma M, Schlegel MP, Afonso MS, et al.. Regulatory T cells license macrophage pro-resolving functions during atherosclerosis regression. Circ Res. 2020;127:335–353. doi:10.1161/CIRCRESAHA.119.316461
- Williams PJ, Searle RF, Robson SC, Innes BA, Bulmer JN. Decidual leucocyte populations in early to late gestation normal human pregnancy. J Reprod Immunol. 2009;82:24–31. doi:10.1016/j.jri.2009.08.001
- Mjösberg J, Berg G, Jenmalm MC, Ernerudh J. FOXP3+ regulatory T cells and T helper 1, T helper 2, and T helper 17 cells in human early pregnancy decidua. Biol Reprod. 2010;82:698–705. doi:10.1095/biolreprod.109.081208
- Tilburgs T, Roelen DL, van der Mast BJ, et al.. Differential distribution of CD4(+)CD25(bright) and CD8(+)CD28(-) T-cells in decidua and maternal blood during human pregnancy. Placenta. 2006;27:S47–53. doi:10.1016/j.placenta.2005.11.008
- Sakaguchi S. Naturally arising CD4+ regulatory t cells for immunologic self-tolerance and negative control of immune responses. Annu Rev Immunol. 2004;22:531–562. doi:10.1146/annurev.immunol.21.120601.141122
- Sakaguchi S, Sakaguchi N, Asano M, Itoh M, Toda M. Immunologic self-tolerance maintained by activated T cells expressing IL-2 receptor alpha-chains (CD25). Breakdown of a single mechanism of self-tolerance causes various autoimmune diseases. J Immunol. 1995;155:1151–1164. doi:10.4049/jimmunol.155.3.1151
- Hori S, Nomura T, Sakaguchi S. Control of regulatory T cell development by the transcription factor Foxp3. Science. 2003;299:1057–1061. doi:10.1126/science.1079490
- Khattri R, Cox T, Yasayko SA, Ramsdell F. An essential role for Scurfin in CD4+CD25+ T regulatory cells. Nat Immunol. 2003;4:337–342. doi:10.1038/ni909
- Fontenot JD, Gavin MA, Rudensky AY. Foxp3 programs the development and function of CD4+CD25+ regulatory T cells. Nat Immunol. 2003;4:330–336. doi:10.1038/ni904
- Zhang YH, Sun HX. Immune checkpoint molecules in pregnancy: focus on regulatory T cells. Eur J Immunol. 2020;50:160–169. doi:10.1002/eji.201948382
- Miko E, Meggyes M, Doba K, Barakonyi A, Szereday L. Immune Checkpoint Molecules in Reproductive Immunology. Front Immunol. 2019;10:846. doi:10.3389/fimmu.2019.00846
- Xu YY, Wang SC, Li DJ, Du MR. Co-signaling molecules in maternal-fetal immunity. Trends Mol Med. 2017;23:46–58. doi:10.1016/j.molmed.2016.11.001
- Joller N, Kuchroo VK. Tim-3, Lag-3, and TIGIT. Curr Top Microbiol Immunol. 2017;410:127–156. doi:10.1007/82_2017_62
- Wagner MI, Jöst M, Spratte J, et al.. Differentiation of ICOS+ and ICOS- recent thymic emigrant regulatory T cells (RTE T regs) during normal pregnancy, pre-eclampsia and HELLP syndrome. Clin Exp Immunol. 2016;183:129–142. doi:10.1111/cei.12693
- Practice Committee of the American Society for Reproductive Medicine. Definitions of infertility and recurrent pregnancy loss: a committee opinion. Fertil Steril. 2020;113:533–535. doi:10.1016/j.fertnstert.2019.11.025
- Dimitriadis E, Menkhorst E, Saito S, Kutteh WH, Brosens JJ. Recurrent pregnancy loss. Nat Rev Dis Primers. 2020;6:98. doi:10.1038/s41572-020-00228-z
- Garrido-Gimenez C, Alijotas-Reig J. Recurrent miscarriage: causes, evaluation and management. Postgrad Med J. 2015;91:151–162. doi:10.1136/postgradmedj-2014-132672
- Alves C, Jenkins SM, Rapp A. StatPearls. Treasure Island (FL): StatPearls; 2024.
- Daumová M, Hadravská Š, Putzová M. Spontaneous abortion in the first trimester of pregnancy. Cesk Patol. 2023;59(2):60–63.
- Practice Committee of the American Society for Reproductive Medicine. Evaluation and treatment of recurrent pregnancy loss: a committee opinion. Fertil Steril. 2012;98:1103–1111. doi:10.1016/j.fertnstert.2012.06.048
- Sun H, Mao J, Su X, Du Q. Impact of spontaneous abortion history and induced abortion history on perinatal outcomes of singleton pregnancies. BMC Public Health. 2023;23(1):2360. doi:10.1186/s12889-023-17264-5
- de Ziegler D, Frydman RF. Recurrent pregnancy losses, a lasting cause of infertility. Fertil Steril. 2021;115(3):531–532. doi:10.1016/j.fertnstert.2020.12.004
- Schatz F, Guzeloglu-Kayisli O, Arlier S, Kayisli UA, Lockwood CJ. The role of decidual cells in uterine hemostasis, menstruation, inflammation, adverse pregnancy outcomes and abnormal uterine bleeding. Hum Reprod Update. 2016;22:497–515. doi:10.1093/humupd/dmw004
- Du Y, Fang Q, Zheng SG. Regulatory T cells: concept, classification, phenotype, and biological characteristics. Adv Exp Med Biol. 2021;1278:1–31. doi:10.1007/978-981-15-6407-9_1
- Josefowicz SZ, Niec RE, Kim HY, et al.. Extrathymically generated regulatory T cells control mucosal TH2 inflammation. Nature. 2012;482:395–399. doi:10.1038/nature10772
- Josefowicz SZ, Lu LF, Rudensky AY. Regulatory T cells: mechanisms of differentiation and function. Annu Rev Immunol. 2012;30:531–564. doi:10.1146/annurev.immunol.25.022106.141623
- Abbas AK, Benoist C, Bluestone JA, et al.. Regulatory T cells: recommendations to simplify the nomenclature. Nat Immunol. 2013;14:307–308. doi:10.1038/ni.2554
- Smigiel KS, Srivastava S, Stolley JM, Campbell DJ. Regulatory T-cell homeostasis: steady-state maintenance and modulation during inflammation. Immunol Rev. 2014;259:40–59. doi:10.1111/imr.12170
- Liston A, Gray DH. Homeostatic control of regulatory T cell diversity. Nat Rev Immunol. 2014;14:154–165. doi:10.1038/nri3605
- Dias S, D’Amico A, Cretney E, et al.. Effector Regulatory T cell differentiation and immune homeostasis depend on the transcription factor Myb. Immunity. 2017;46:78–91. doi:10.1016/j.immuni.2016.12.017
- Burzyn D, Benoist C, Mathis D. Regulatory T cells in nonlymphoid tissues. Nat Immunol. 2013;14:1007–1013. doi:10.1038/ni.2683
- Miragaia RJ, Gomes T, Chomka A, et al.. Single-cell transcriptomics of regulatory T cells reveals trajectories of tissue adaptation. Immunity. 2019;50:493–504.e7. doi:10.1016/j.immuni.2019.01.001
- Yu X, Harden K, Gonzalez LC, et al.. The surface protein TIGIT suppresses T cell activation by promoting the generation of mature immunoregulatory dendritic cells. Nat Immunol. 2009;10:48–57. doi:10.1038/ni.1674
- Brlić P K, Lenac Roviš T, Cinamon G, Tsukerman P, Mandelboim O, Jonjić S. Targeting PVR (CD155) and its receptors in anti-tumor therapy. Cell Mol Immunol. 2019;16:40–52. doi:10.1038/s41423-018-0168-y
- Joller N, Lozano E, Burkett PR, et al.. Treg cells expressing the coinhibitory molecule TIGIT selectively inhibit proinflammatory Th1 and Th17 cell responses. Immunity. 2014;40:569–581. doi:10.1016/j.immuni.2014.02.012
- Levine AG, Mendoza A, Hemmers S, et al.. Stability and function of regulatory T cells expressing the transcription factor T-bet. Nature. 2017;546:421–425. doi:10.1038/nature22360
- Paust S, Lu L, McCarty N, Cantor H. Engagement of B7 on effector T cells by regulatory T cells prevents autoimmune disease. Proc Natl Acad Sci USA. 2004;101:10398–10403. doi:10.1073/pnas.0403342101
- Fallarino F, Grohmann U, Hwang KW, et al.. Modulation of tryptophan catabolism by regulatory T cells. Nat Immunol. 2003;4:1206–1212. doi:10.1038/ni1003
- Tan CL, Kuchroo JR, Sage PT, et al.. PD-1 restraint of regulatory T cell suppressive activity is critical for immune tolerance. J Exp Med. 2021;218:e20182232.
- Maruhashi T, Sugiura D, Okazaki IM, et al.. Binding of LAG-3 to stable peptide-MHC class II limits T cell function and suppresses autoimmunity and anti-cancer immunity. Immunity. 2022;55:912–924.e8. doi:10.1016/j.immuni.2022.03.013
- Bodmer JL, Holler N, Reynard S, et al.. TRAIL receptor-2 signals apoptosis through FADD and caspase-8. Nat Cell Biol. 2000;2:241–243. doi:10.1038/35008667
- Ren X, Ye F, Jiang Z, Chu Y, Xiong S, Wang Y. Involvement of cellular death in TRAIL/DR5-dependent suppression induced by CD4(+)CD25(+) regulatory T cells. Cell Death Differ. 2007;14:2076–2084. doi:10.1038/sj.cdd.4402220
- Śledzińska A, Vila de Mucha M, Bergerhoff K, et al.. Regulatory T Cells Restrain Interleukin-2- and Blimp-1-Dependent Acquisition of Cytotoxic Function by CD4(+) T Cells. Immunity. 2020;52:151–166.e6. doi:10.1016/j.immuni.2019.12.007
- Sundström P, Stenstad H, Langenes V, et al.. Regulatory T cells from colon cancer patients inhibit effector T-cell migration through an adenosine-dependent mechanism. Cancer Immunol Res. 2016;4:183–193. doi:10.1158/2326-6066.CIR-15-0050
- Klein M, Bopp T. Cyclic AMP represents a crucial component of treg cell-mediated immune regulation. Front Immunol. 2016;7:315. doi:10.3389/fimmu.2016.00315
- Su W, Chen X, Zhu W, et al.. The cAMP-adenosine feedback loop maintains the suppressive function of regulatory T cells. J Immunol. 2019;203:1436–1446. doi:10.4049/jimmunol.1801306
- Schneider E, Winzer R, Rissiek A, et al.. CD73-mediated adenosine production by CD8 T cell-derived extracellular vesicles constitutes an intrinsic mechanism of immune suppression. Nat Commun. 2021;12:5911. doi:10.1038/s41467-021-26134-w
- Hayashi Y, Ohnuma K, Furue MK. Pluripotent Stem Cell Heterogeneity. Adv Exp Med Biol. 2019;1123:71–94.
- Zhao DM, Thornton AM, DiPaolo RJ, Shevach EM. Activated CD4+CD25+ T cells selectively kill B lymphocytes. Blood. 2006;107:3925–3932. doi:10.1182/blood-2005-11-4502
- Grossman WJ, Verbsky JW, Barchet W, Colonna M, Atkinson JP, Ley TJ. Human T regulatory cells can use the perforin pathway to cause autologous target cell death. Immunity. 2004;21:589–601. doi:10.1016/j.immuni.2004.09.002
- Gondek DC, Devries V, Nowak EC, et al.. Transplantation survival is maintained by granzyme B+ regulatory cells and adaptive regulatory T cells. J Immunol. 2008;181:4752–4760. doi:10.4049/jimmunol.181.7.4752
- Yano H, Andrews LP, Workman CJ, Vignali D. Intratumoral regulatory T cells: markers, subsets and their impact on anti-tumor immunity. Immunology. 2019;157:232–247. doi:10.1111/imm.13067
- Inada K, Shima T, Ito M, Ushijima A, Saito S. Helios-positive functional regulatory T cells are decreased in decidua of miscarriage cases with normal fetal chromosomal content. J Reprod Immunol. 2015;107:10–19. doi:10.1016/j.jri.2014.09.053
- Hsu P, Santner-Nanan B, Dahlstrom JE, et al.. Altered decidual DC-SIGN+ antigen-presenting cells and impaired regulatory T-cell induction in preeclampsia. Am J Pathol. 2012;181:2149–2160. doi:10.1016/j.ajpath.2012.08.032
- Arruvito L, Sanz M, Banham AH, Fainboim L. Expansion of CD4+CD25+and FOXP3+ regulatory T cells during the follicular phase of the menstrual cycle: implications for human reproduction. J Immunol. 2007;178:2572–2578. doi:10.4049/jimmunol.178.4.2572
- Lee SJ, Song L, Yang MC, et al.. Local administration of granulocyte macrophage colony-stimulating factor induces local accumulation of dendritic cells and antigen-specific CD8+ T cells and enhances dendritic cell cross-presentation. Vaccine. 2015;33:1549–1555. doi:10.1016/j.vaccine.2015.02.019
- Tao Y, Li YH, Zhang D, et al.. Decidual CXCR4(+) CD56(bright) NK cells as a novel NK subset in maternal-foetal immune tolerance to alleviate early pregnancy failure. Clin Transl Med. 2021;11:e540.
- Li Z, Liang X, Chen X, et al.. The role of thymus- and extrathymus-derived regulatory T cells in maternal-fetal tolerance. Front Immunol. 2023;14:1109352. doi:10.3389/fimmu.2023.1109352
- Yasuda I, Shima T, Moriya T, et al.. Dynamic changes in the phenotype of dendritic cells in the uterus and uterine draining lymph nodes after coitus. Front Immunol. 2020;11:557720. doi:10.3389/fimmu.2020.557720
- Kallikourdis M, Betz AG. Periodic accumulation of regulatory T cells in the uterus: preparation for the implantation of a semi-allogeneic fetus. PLoS One. 2007;2:e382.
- Shima T, Sasaki Y, Itoh M, et al.. Regulatory T cells are necessary for implantation and maintenance of early pregnancy but not late pregnancy in allogeneic mice. J Reprod Immunol. 2010;85:121–129. doi:10.1016/j.jri.2010.02.006
- Moldenhauer LM, Diener KR, Hayball JD, Robertson SA. An immunogenic phenotype in paternal antigen-specific CD8(+) T cells at embryo implantation elicits later fetal loss in mice. Immunol Cell Biol. 2017;95:705–715. doi:10.1038/icb.2017.41
- Chaturvedi V, Ertelt JM, Jiang TT, et al.. CXCR3 blockade protects against Listeria monocytogenes infection-induced fetal wastage. J Clin Invest. 2015;125:1713–1725. doi:10.1172/JCI78578
- Li L, Tu J, Jiang Y, Zhou J, Schust DJ. Regulatory T cells decrease invariant natural killer T cell-mediated pregnancy loss in mice. Mucosal Immunol. 2017;10:613–623. doi:10.1038/mi.2016.84
- Zhang Y, Liu Z, Tian M, et al.. The altered PD-1/PD-L1 pathway delivers the ‘one-two punch’ effects to promote the Treg/Th17 imbalance in pre-eclampsia. Cell Mol Immunol. 2018;15:710–723. doi:10.1038/cmi.2017.70
- Erlebacher A. Immunology of the maternal-fetal interface. Annu Rev Immunol. 2013;31:387–411. doi:10.1146/annurev-immunol-032712-100003
- Jiang X, Wang H. Macrophage subsets at the maternal-fetal interface. Cell Mol Immunol. 2020;17:889–891. doi:10.1038/s41423-020-0435-6
- Wang F, Qualls AE, Marques-Fernandez L, Colucci F. Biology and pathology of the uterine microenvironment and its natural killer cells. Cell Mol Immunol. 2021;18:2101–2113. doi:10.1038/s41423-021-00739-z
- Guerin LR, Moldenhauer LM, Prins JR, Bromfield JJ, Hayball JD, Robertson SA. Seminal fluid regulates accumulation of FOXP3+ regulatory T cells in the preimplantation mouse uterus through expanding the FOXP3+ cell pool and CCL19-mediated recruitment. Biol Reprod. 2011;85:397–408. doi:10.1095/biolreprod.110.088591
- Shima T, Nakashima A, Yasuda I, et al.. Uterine CD11c+ cells induce the development of paternal antigen-specific Tregs via seminal plasma priming. J Reprod Immunol. 2020;141:103165. doi:10.1016/j.jri.2020.103165
- Blois SM, Ilarregui JM, Tometten M, et al.. A pivotal role for galectin-1 in fetomaternal tolerance. Nat Med. 2007;13:1450–1457. doi:10.1038/nm1680
- Vacca P, Cantoni C, Vitale M, et al.. Crosstalk between decidual NK and CD14+ myelomonocytic cells results in induction of Tregs and immunosuppression. Proc Natl Acad Sci U S A. 2010;107:11918–11923. doi:10.1073/pnas.1001749107
- Munn DH, Zhou M, Attwood JT, et al.. Prevention of allogeneic fetal rejection by tryptophan catabolism. Science. 1998;281:1191–1193. doi:10.1126/science.281.5380.1191
- Zhang J, Dunk C, Croy AB, Lye SJ. To serve and to protect: the role of decidual innate immune cells on human pregnancy. Cell Tissue Res. 2016;363:249–265. doi:10.1007/s00441-015-2315-4
- Perchellet AL, Jasti S, Petroff MG. Maternal CD4⁺ and CD8⁺ T cell tolerance towards a fetal minor histocompatibility antigen in T cell receptor transgenic mice. Biol Reprod. 2013;89:102. doi:10.1095/biolreprod.113.110445
- Wang S, Qian J, Sun F, et al.. Bidirectional regulation between 1st trimester HTR8/SVneo trophoblast cells and in vitro differentiated Th17/Treg cells suggest a fetal-maternal regulatory loop in human pregnancy. Am J Reprod Immunol. 2019;81:e13106. doi:10.1111/aji.13106
- Fu YY, Ren CE, Qiao PY, Meng YH. Uterine natural killer cells and recurrent spontaneous abortion. Am J Reprod Immunol. 2021;86:e13433.
- Díaz-Hernández I, Alecsandru D, García-Velasco JA, Domínguez F. Uterine natural killer cells: from foe to friend in reproduction. Hum Reprod Update. 2021;27:720–746. doi:10.1093/humupd/dmaa062
- Heikkinen J, Möttönen M, Alanen A, Lassila O. Phenotypic characterization of regulatory T cells in the human decidua. Clin Exp Immunol. 2004;136:373–378. doi:10.1111/j.1365-2249.2004.02441.x
- Dimova T, Nagaeva O, Stenqvist AC, et al.. Maternal Foxp3 expressing CD4+ CD25+ and CD4+ CD25- regulatory T-cell populations are enriched in human early normal pregnancy decidua: a phenotypic study of paired decidual and peripheral blood samples. Am J Reprod Immunol. 2011;66(1):44–56. doi:10.1111/j.1600-0897.2011.01046.x
- Salvany-Celades M, van der Zwan A, Benner M, et al.. Tilburgs T: three types of functional regulatory T Cells Control T cell responses at the human maternal-fetal interface. Cell Rep. 2019;27:2537–2547.e5. doi:10.1016/j.celrep.2019.04.109
- Zare M, Namavar Jahromi B, Gharesi-Fard B. Analysis of the frequencies and functions of CD4(+)CD25(+)CD127(low/neg), CD4(+)HLA-G(+), and CD8(+)HLA-G(+) regulatory T cells in pre-eclampsia. J Reprod Immunol. 2019;133:43–51. doi:10.1016/j.jri.2019.06.002
- Hsu P, Santner-Nanan B, Joung S, Peek MJ, Nanan R. Expansion of CD4(+) HLA-G(+) T Cell in human pregnancy is impaired in pre-eclampsia. Am J Reprod Immunol. 2014;71:217–228. doi:10.1111/aji.12195
- Huang YH, Zozulya AL, Weidenfeller C, Schwab N, Wiendl H. T cell suppression by naturally occurring HLA-G-expressing regulatory CD4+ T cells is IL-10-dependent and reversible. J Leukoc Biol. 2009;86:273–281. doi:10.1189/jlb.1008649
- Levings MK, Bacchetta R, Schulz U, Roncarolo MG. The role of IL-10 and TGF-beta in the differentiation and effector function of T regulatory cells. Int Arch Allergy Immunol. 2002;129:263–276. doi:10.1159/000067596
- Sanjabi S, Oh SA, Li MO. Regulation of the immune response by TGF-β: from conception to autoimmunity and infection. Cold Spring Harb Perspect Biol. 2017;9:a022236. doi:10.1101/cshperspect.a022236
- Zhang J, Dunk CE, Shynlova O, Caniggia I, Lye SJ. TGFb1 suppresses the activation of distinct dNK subpopulations in preeclampsia. EBioMedicine. 2019;39:531–539. doi:10.1016/j.ebiom.2018.12.015
- Häringer B, Lozza L, Steckel B, Geginat J. Identification and characterization of IL-10/IFN-gamma-producing effector-like T cells with regulatory function in human blood. J Exp Med. 2009;206:1009–1017.
- Akdis M, Verhagen J, Taylor A, et al.. Immune responses in healthy and allergic individuals are characterized by a fine balance between allergen-specific T regulatory 1 and T helper 2 cells. J Exp Med. 2004;199:1567–1575. doi:10.1084/jem.20032058
- White AM, Wraith DC. Tr1-Like T cells - an enigmatic regulatory T cell lineage. Front Immunol. 2016;7:355. doi:10.3389/fimmu.2016.00355
- Niedzielska M, Israelsson E, Angermann B, et al.. Differential gene expression in human tissue resident regulatory T cells from lung, colon, and blood. Oncotarget. 2018;9:36166–36184. doi:10.18632/oncotarget.26322
- Weiner HL. Induction and mechanism of action of transforming growth factor-beta-secreting Th3 regulatory cells. Immunol Rev. 2001;182:207–214. doi:10.1034/j.1600-065X.2001.1820117.x
- Elkord E, Abd Al Samid M, Chaudhary B. Helios, and not FoxP3, is the marker of activated Tregs expressing GARP/LAP. Oncotarget. 2015;6:20026–20036.
- Aluvihare VR, Kallikourdis M, Betz AG. Regulatory T cells mediate maternal tolerance to the fetus. Nat Immunol. 2004;5:266–271. doi:10.1038/ni1037
- Woidacki K, Meyer N, Schumacher A, Goldschmidt A, Maurer M, Zenclussen AC. Transfer of regulatory T cells into abortion-prone mice promotes the expansion of uterine mast cells and normalizes early pregnancy angiogenesis. Sci Rep. 2015;5:13938. doi:10.1038/srep13938
- Keller CC, Eikmans M, van der Hoorn MP, Lashley L. Recurrent miscarriages and the association with regulatory T cells; A systematic review. J Reprod Immunol. 2020;139:103105. doi:10.1016/j.jri.2020.103105
- Banerjee P, Jana SK, Pasricha P, Ghosh S, Chakravarty B, Chaudhury K. Proinflammatory cytokines induced altered expression of cyclooxygenase-2 gene results in unreceptive endometrium in women with idiopathic recurrent spontaneous miscarriage. Fertil Steril. 2013;99:179–187.e2. doi:10.1016/j.fertnstert.2012.08.034
- Yang X, Tian Y, Zheng L, Luu T, Kwak-Kim J. The Update Immune-Regulatory Role of Pro- and Anti-Inflammatory Cytokines in Recurrent Pregnancy Losses. Int J Mol Sci. 2022;24:132. doi:10.3390/ijms24010132
- Kwak-Kim J, Bao S, Lee SK, Kim JW, Gilman-Sachs A. Immunological modes of pregnancy loss: inflammation, immune effectors, and stress. Am J Reprod Immunol. 2014;72:129–140. doi:10.1111/aji.12234
- Lissauer D, Goodyear O, Khanum R, Moss PA, Kilby MD. Profile of maternal CD4 T-cell effector function during normal pregnancy and in women with a history of recurrent miscarriage. Clin Sci (Lond). 2014;126:347–354. doi:10.1042/CS20130247
- Lédée N, Munaut C, Aubert J, et al.. Specific and extensive endometrial deregulation is present before conception in IVF/ICSI repeated implantation failures (IF) or recurrent miscarriages. J Pathol. 2011;225:554–564. doi:10.1002/path.2948
- Zhao X, Jiang Y, Wang L, Li Z, Li Q, Feng X. Advances in understanding the immune imbalance between T-Lymphocyte Subsets and NK cells in recurrent spontaneous abortion. Geburtshilfe Frauenheilkd. 2018;78(7):677–683. doi:10.1055/a-0634-1813
- Cubro H, Kashyap S, Nath MC, Ackerman AW, Garovic VD. The role of interleukin-10 in the pathophysiology of preeclampsia. Curr Hypertens Rep. 2018;20:36. doi:10.1007/s11906-018-0833-7
- Kedzierska AE, Lorek D, Slawek A, Chelmonska-Soyta A. Tregitopes regulate the tolerogenic immune response and decrease the foetal death rate in abortion-prone mouse matings. Sci Rep. 2020;10:10531. doi:10.1038/s41598-020-66957-z
- Granne I, Shen M, Rodriguez-Caro H, et al.. Characterisation of peri-implantation endometrial Treg and identification of an altered phenotype in recurrent pregnancy loss. Mucosal Immunol. 2022;15:120–129. doi:10.1038/s41385-021-00451-1
- Yang H, Qiu L, Chen G, Ye Z, C L, Lin Q. Proportional change of CD4+CD25+ regulatory T cells in decidua and peripheral blood in unexplained recurrent spontaneous abortion patients. Fertil Steril. 2008;89:656–661. doi:10.1016/j.fertnstert.2007.03.037
- Jin LP, Chen QY, Zhang T, Guo PF, Li DJ. The CD4+CD25 bright regulatory T cells and CTLA-4 expression in peripheral and decidual lymphocytes are down-regulated in human miscarriage. Clin Immunol. 2009;133:402–410. doi:10.1016/j.clim.2009.08.009
- Inada K, Shima T, Nakashima A, Aoki K, Ito M, Saito S. Characterization of regulatory T cells in decidua of miscarriage cases with abnormal or normal fetal chromosomal content. J Reprod Immunol. 2013;97:104–111. doi:10.1016/j.jri.2012.12.001
- Sasaki Y, Sakai M, Miyazaki S, Higuma S, Shiozaki A, Saito S. Decidual and peripheral blood CD4+CD25+ regulatory T cells in early pregnancy subjects and spontaneous abortion cases. Mol Hum Reprod. 2004;10:347–353. doi:10.1093/molehr/gah044
- Wang WJ, Hao CF, Yi-Lin Y, Bao GJ, Qiu SH, Lin LH. QD: increased prevalence of T helper 17 (Th17) cells in peripheral blood and decidua in unexplained recurrent spontaneous abortion patients. J Reprod Immunol. 2010;84:164–170. doi:10.1016/j.jri.2009.12.003
- Robertson SA, Sharkey DJ. Seminal fluid and fertility in women. Fertil Steril. 2016;106:511–519. doi:10.1016/j.fertnstert.2016.07.1101
- Omenetti S, Pizarro TT. The Treg/Th17 Axis: a dynamic balance regulated by the gut microbiome. Front Immunol. 2015;6:639. doi:10.3389/fimmu.2015.00639
- Sadlon T, Brown CY, Bandara V, et al.. Unravelling the molecular basis for regulatory T-cell plasticity and loss of function in disease. Clin Transl Immunology. 2018;7:e1011.
- Schjenken JE, Zhang B, Chan HY, Sharkey DJ, Fullston T, Robertson SA. mi RNA Regulation of Immune Tolerance in Early Pregnancy. Am J Reprod Immunol. 2016;75:272–280. doi:10.1111/aji.12490
- Hori S. Lineage stability and phenotypic plasticity of Foxp3⁺ regulatory T cells. Immunol Rev. 2014;259:159–172. doi:10.1111/imr.12175
- Liu C, Wang XZ, Sun XB. Assessment of sperm antigen specific T regulatory cells in women with recurrent miscarriage. Early Hum Dev. 2013;89:95–100. doi:10.1016/j.earlhumdev.2012.08.003
- Bettelli E, Carrier Y, Gao W, et al.. Reciprocal developmental pathways for the generation of pathogenic effector TH17 and regulatory T cells. Nature. 2006;441:235–238. doi:10.1038/nature04753
- Zhao J, Zhao J, Perlman S. Differential effects of IL-12 on Tregs and non-Treg T cells: roles of IFN-γ, IL-2 and IL-2R. PLoS One. 2012;7:e46241.
- Prins JR, Zhang B, Schjenken JE, Guerin LR, Barry SC, Robertson SA. Unstable Foxp3+ regulatory T cells and altered dendritic cells are associated with lipopolysaccharide-induced fetal loss in pregnant interleukin 10-deficient mice. Biol Reprod. 2015;93:95. doi:10.1095/biolreprod.115.128694
- Rowe JH, Ertelt JM, Aguilera MN, Farrar MA, Way SS. Foxp3(+) regulatory T cell expansion required for sustaining pregnancy compromises host defense against prenatal bacterial pathogens. Cell Host Microbe. 2011;10:54–64. doi:10.1016/j.chom.2011.06.005
- Robertson SA. Immune regulation of conception and embryo implantation-all about quality control. J Reprod Immunol. 2010;85:51–57. doi:10.1016/j.jri.2010.01.008
- Mazziotta C, Pellielo G, Tognon M, Martini F, Rotondo JC. Significantly low levels of igg antibodies against oncogenic Merkel cell polyomavirus in sera from females affected by spontaneous abortion. Front Microbiol. 2021;12:789991. doi:10.3389/fmicb.2021.789991
- D’Addio F, Riella LV, Mfarrej BG, et al.. The link between the PDL1 costimulatory pathway and Th17 in fetomaternal tolerance. J Immunol. 2011;187:4530–4541. doi:10.4049/jimmunol.1002031
- Chang J-H, Xiao Y, Hu H, et al.. Ubc13 maintains the suppressive function of regulatory T cells and prevents their conversion into effector-like T cells. Nat Immunol. 2012;13(5):481–490. doi:10.1038/ni.2267
- Steinborn A, Schmitt E, Kisielewicz A, et al.. Pregnancy-associated diseases are characterized by the composition of the systemic regulatory T cell (Treg) pool with distinct subsets of Tregs. Clin Exp Immunol. 2012;167:84–98. doi:10.1111/j.1365-2249.2011.04493.x
- Bluestone JA, Trotta E, Xu D. The therapeutic potential of regulatory T cells for the treatment of autoimmune disease. Expert Opin Ther Targets. 2015;19:1091–1103. doi:10.1517/14728222.2015.1037282
- Zhang Q, Wang HY, Marzec M, Raghunath PN, Nagasawa T, Wasik MA. STAT3- and DNA methyltransferase 1-mediated epigenetic silencing of SHP-1 tyrosine phosphatase tumor suppressor gene in malignant T lymphocytes. Proc Natl Acad Sci U S A. 2005;102:6948–6953. doi:10.1073/pnas.0501959102
- Hodge DR, Cho E, Copeland TD, et al.. IL-6 enhances the nuclear translocation of DNA cytosine-5-methyltransferase 1 (DNMT1) via phosphorylation of the nuclear localization sequence by the AKT kinase. Cancer Genomics Proteomics. 2007;4:387–398.
- Kimura A, Kishimoto T. IL-6: regulator of Treg/Th17 balance. Eur J Immunol. 2010;40:1830–1835. doi:10.1002/eji.201040391
- Raffin C, Vo LT, Bluestone JA. T(reg) cell-based therapies: challenges and perspectives. Nat Rev Immunol. 2020;20:158–172. doi:10.1038/s41577-019-0232-6
- Nishimoto N, Yoshizaki K, Miyasaka N, et al.. Treatment of rheumatoid arthritis with humanized anti-interleukin-6 receptor antibody: a multicenter, double-blind, placebo-controlled trial. Arthritis Rheum. 2004;50:1761–1769. doi:10.1002/art.20303
- Ito H, Takazoe M, Fukuda Y, et al.. A pilot randomized trial of a human anti-interleukin-6 receptor monoclonal antibody in active Crohn’s disease. Gastroenterology. 2004;126:989–996. doi:10.1053/j.gastro.2004.01.012
- Illei GG, Shirota Y, Yarboro CH, et al.. Tocilizumab in systemic lupus erythematosus: data on safety, preliminary efficacy, and impact on circulating plasma cells from an open-label phase I dosage-escalation study. Arthritis Rheum. 2010;62:542–552. doi:10.1002/art.27221
- Abbas AK, Trotta E, Simeonov D, Marson A, Bluestone JA. Revisiting IL-2: biology and therapeutic prospects. Sci Immunol. 2018;3:eaat1482. doi:10.1126/sciimmunol.aat1482
- Barron L, Dooms H, Hoyer KK, et al.. Cutting edge: mechanisms of IL-2-dependent maintenance of functional regulatory T cells. J Immunol. 2010;185:6426–6430. doi:10.4049/jimmunol.0903940
- Boardman DA, Levings MK. Cancer immunotherapies repurposed for use in autoimmunity. Nat Biomed Eng. 2019;3:259–263. doi:10.1038/s41551-019-0359-6
- Tang Q, Adams JY, Penaranda C, et al.. Central role of defective interleukin-2 production in the triggering of islet autoimmune destruction. Immunity. 2008;28:687–697. doi:10.1016/j.immuni.2008.03.016
- Grinberg-Bleyer Y, Baeyens A, You S, et al.. IL-2 reverses established type 1 diabetes in NOD mice by a local effect on pancreatic regulatory T cells. J Exp Med. 2010;207:1871–1878. doi:10.1084/jem.20100209
- Trotta E, Bessette PH, Silveria SL, et al.. A human anti-IL-2 antibody that potentiates regulatory T cells by a structure-based mechanism. Nat Med. 2018;24:1005–1014. doi:10.1038/s41591-018-0070-2
- Ito S, Bollard CM, Carlsten M, et al.. Ultra-low dose interleukin-2 promotes immune-modulating function of regulatory T cells and natural killer cells in healthy volunteers. Mol Ther. 2014;22:1388–1395. doi:10.1038/mt.2014.50
- Winger EE, Reed JL. Low circulating CD4(+) CD25(+) Foxp3(+) T regulatory cell levels predict miscarriage risk in newly pregnant women with a history of failure. Am J Reprod Immunol. 2011;66:320–328. doi:10.1111/j.1600-0897.2011.00992.x
- Mohammadi S, Abdollahi E, Nezamnia M, et al. Adoptive transfer of Tregs: a novel strategy for cell-based immunotherapy in spontaneous abortion: lessons from experimental models. Int Immunopharmacol. 2021;90:107195. doi:10.1016/j.intimp.2020.107195
- Siddiqui I, Erreni M, van Brakel M, Debets R, Allavena P. Enhanced recruitment of genetically modified CX3CR1-positive human T cells into Fractalkine/CX3CL1 expressing tumors: importance of the chemokine gradient. J Immunother Cancer. 2016;4:21. doi:10.1186/s40425-016-0125-1
- Garetto S, Sardi C, Martini E, et al.. Tailored chemokine receptor modification improves homing of adoptive therapy T cells in a spontaneous tumor model. Oncotarget. 2016;7:43010–43026. doi:10.18632/oncotarget.9280
- Idorn M, Skadborg SK, Kellermann L, et al.. Chemokine receptor engineering of T cells with CXCR2 improves homing towards subcutaneous human melanomas in xenograft mouse model. Oncoimmunology. 2018;7:e1450715.
- Zhang L, Long X, Yin Y, et al.. Histone methyltransferase Nsd2 ensures maternal-fetal immune tolerance by promoting regulatory T-cell recruitment. Cell Mol Immunol. 2022;19:634–643. doi:10.1038/s41423-022-00849-2
- Motwani K, Peters LD, Vliegen WH, et al.. Human regulatory T cells from umbilical cord blood display increased repertoire diversity and lineage stability relative to adult peripheral blood. Front Immunol. 2020;11:611. doi:10.3389/fimmu.2020.00611
- Jagger A, Shimojima Y, Goronzy JJ, Weyand CM. Regulatory T cells and the immune aging process: a mini-review. Gerontology. 2014;60:130–137. doi:10.1159/000355303
- Carbone F, La Rocca C, De Candia P, et al.. Metabolic control of immune tolerance in health and autoimmunity. Semin Immunol. 2016;28:491–504. doi:10.1016/j.smim.2016.09.006
- Murai M, Krause P, Cheroutre H, Kronenberg M. Regulatory T-cell stability and plasticity in mucosal and systemic immune systems. Mucosal Immunol. 2010;3:443–449. doi:10.1038/mi.2010.27
- Amersfoort J, Kuiper J. T cell metabolism in metabolic disease-associated autoimmunity. Immunobiology. 2017;222:925–936. doi:10.1016/j.imbio.2017.03.001
- Issazadeh-Navikas S, Teimer R, Bockermann R. Influence of dietary components on regulatory T cells. Mol Med. 2012;18:95–110. doi:10.2119/molmed.2011.00311
- Sharkey DJ, Tremellen KP, Briggs NE, Dekker GA, Robertson SA. Seminal plasma pro-inflammatory cytokines interferon-γ (IFNG) and C-X-C motif chemokine ligand 8 (CXCL8) fluctuate over time within men. Hum Reprod. 2017;32:1373–1381. doi:10.1093/humrep/dex106
- Robertson SA, Moldenhauer LM, Green ES, Care AS, Hull ML. Immune determinants of endometrial receptivity: a biological perspective. Fertil Steril. 2022;117:1107–1120. doi:10.1016/j.fertnstert.2022.04.023
- Yamazaki S, Nishioka A, Kasuya S, et al.. Homeostasis of thymus-derived Foxp3+ regulatory T cells is controlled by ultraviolet B exposure in the skin. J Immunol. 2014;193:5488–5497. doi:10.4049/jimmunol.1400985
- Burzyn D, Kuswanto W, Kolodin D, et al.. A special population of regulatory T cells potentiates muscle repair. Cell. 2013;155:1282–1295. doi:10.1016/j.cell.2013.10.054
- Li J, Chen Y, Liu C, Hu Y, Li L. Intravenous immunoglobulin treatment for repeated IVF/ICSI failure and unexplained infertility: a systematic review and a meta-analysis. Am J Reprod Immunol. 2013;70:434–447. doi:10.1111/aji.12170
- Winger EE, Reed JL. Treatment with tumor necrosis factor inhibitors and intravenous immunoglobulin improves live birth rates in women with recurrent spontaneous abortion. Am J Reprod Immunol. 2008;60:8–16. doi:10.1111/j.1600-0897.2008.00585.x
- Tempfer CB, Kurz C, Bentz EK, et al.. A combination treatment of prednisone, aspirin, folate, and progesterone in women with idiopathic recurrent miscarriage: a matched-pair study. Fertil Steril. 2006;86:145–148. doi:10.1016/j.fertnstert.2005.12.035
- Vomstein K, Feil K, Strobel L, et al.. Immunological risk factors in recurrent pregnancy loss: guidelines versus current state of the art. J Clin Med. 2021;10:869. doi:10.3390/jcm10040869
- Lee JH, Ulrich B, Cho J, Park J, Kim CH. Progesterone promotes differentiation of human cord blood fetal T cells into T regulatory cells but suppresses their differentiation into Th17 cells. J Immunol. 2011;187:1778–1787. doi:10.4049/jimmunol.1003919
- Lee JH, Lydon JP, Kim CH. Progesterone suppresses the mTOR pathway and promotes generation of induced regulatory T cells with increased stability. Eur J Immunol. 2012;42:2683–2696. doi:10.1002/eji.201142317
- Piccinni MP, Scaletti C, Maggi E, Romagnani S. Role of hormone-controlled Th1- and Th2-type cytokines in successful pregnancy. J Neuroimmunol. 2000;109:30–33. doi:10.1016/S0165-5728(00)00299-X